KLİNİK ÇALIŞMA
Tuberk Toraks 2021;69(2):133-143
Can LENT Prognostic score (LDH, ECOG performance score, blood neutrophil/lymphocyte ratio, tumor type) change the clinical approach in malignant pleural effusion?
Mine GAYAF1 , Ceyda ANAR2 , Mustafa CANBAZ1 , Betül İkbal DOĞAN2 , Ahmet Emin ERBAYCU1 , Filiz GÜLDAVAL1
1Clinic of Chest Diseases, Dr. Suat Seren Chest Diseases and Surgery Training and Research Hospital, Izmir, Turkey.
1Dr. Suat Seren Göğüs Hastalıkları ve Cerrahisi Eğitim ve Araştırma Hastanesi, Göğüs Hastalıkları Kliniği, İzmir, Türkiye.
2Clinic of Chest Diseases, Katip Çelebi University Atatürk Training and Research Hospital, İzmir, Turkey.
2Katip Çelebi Üniversitesi Atatürk Eğitim Araştırma Hastanesi, Göğüs Hastalıkları Kliniği, İzmir, Türkiye.
Cite this article as: Gayaf M, Anar C, Canbaz M, Doğan Bİ, Erbaycu AE, Güldaval F. Can LENT Prognostic score (LDH, ECOG performance score, blood neutrophil/lymphocyte ratio, tumor type) change the clinical approach in malignant pleural effusion? Tuberk Toraks 2021;69(2):133-143.
ÖZ
LENT prognostik skoru (LDH, ECOG performans skoru, kan nötrofil/lenfosit oranı, tümör tipi) malign plevral efüzyonda klinik yaklaşımı değiştirebilir mi?
Giriş: Bu çalışmanın amacı güncel bir prognostik skor olan LENT (plevral mayide LDH, Eastern Cooperative Oncology Group [ECOG] performans durumu, serumda nötrofil-lenfosit oranı ve tümör tipi) skorunun MPE’li hastalarda, sağkalıma etkisinin ve klinik karar vermedeki durumunun prediktif gücünü değerlendirmektir. Ayrıca LENT skorunu konvansiyonel ancak subjectif skor olan ECOG ile karşılaştırmaktır.
Materyal ve Metod: 2008-2018 yılları arasında MPE (malign plevral efüzyon) için tedavi edilen hastaların tıbbi kayıtları gözden geçirilerek geriye dönük gözlemsel bir çalışma yapıldı. Hastalarda LENT prognostik skoru hesaplandı. Aynı hastalar için hesaplanan ECOG skoru mortalite açısından karşılaştırıldı.
Bulgular: Çalışmaya 118 erkek (%61,7) ve 73 kadın (%38,2) olmak üzere toplam 191 malign plevral efüzyonlu hasta dahil edildi. Genel sağkalımı belirlemek için duyarlılık, özgüllük, pozitif prediktif değeri (PPV) ve negatif prediktif değeri (NPV) LENT skoru >4’te sırasıyla %69,8, % 00,%100 ve %18,8 idi (p= 0,000. ECOG PS >2’de, genel sağkalımı tanımlamak için duyarlılık, özgüllük, PPV, NPV, LENT skoru >4 ile aynıydı.Tüm hastalarda, LENT skoruna göre genel medyan sağkalım, düşük/orta/yüksek risk gruplarında sırasıyla 662/119/33 gündü. Cox regresyon analizi, LENT skorunun orta (p= 0,004, OR: 2,21, CI: 1,29-%3,78) ve yüksek düzeyde olmasının (p= 0,000, OR: 4, 50 CI: 2,57-%7,89) MPE tüm hastalarda genel sağkalımı öngörmekteydi. ROC analizinde 1., 6. ve 12. aylarda hem LENT hem de ECOG açısından mortalitede fark yoktu.
Sonuç: LENT erken mortaliteyi öngörmede ECOG’dan daha iyi bir skorlama sistemi iken, her ikisi de ECOG ve LENT mortaliteyi tahmin etmede hemen hemen aynı güce sahiptir. Ancak LENT biraz daha objektiftir ancak laboratuvar bulgularını içerdiğinden hesaplanması daha zordur. Bu nedenle, her iki skorlama sistemi de malign plevral efüzyonlu hastalarda mortaliteyi tahmin etmek için kullanılabilir. Hiçbirinin birbirine üstünlüğü yoktur.
Anahtar kelimeler: Malign plevral effüzyon; LENT; sağkalım; prognoz
ABSTRACT
Can LENT Prognostic score (LDH, ECOG performance score, blood neutrophil/lymphocyte ratio, tumor type) change the clinical approach in malignant pleural effusion?
Introduction: The aim of this study was to evaluate the predictive power of LENT (LDH in pleural fluid, Eastern Cooperative Oncology Group [ECOG] performance status, neutrophil–lymphocyte ratio in the serum, and tumor type) score which is a current prognostic score in patients with MPE and to determine its effect on survival and its status in clinical decision making. In addition, it was aimed to compare LENT score with the conventional but subjective score ECOG.
Materials and Methods: A retrospective observational study was conducted reviewing the medical records of patients managed for MPE (malign pleural effusion) between 2008 and 2018. LENT prognostic score was calculated in the patients. The ECOG score calculated for the same patients was compared in terms of mortality.
Results: A total of 191 patients with malignant pleural effusion, 118 males (61.7%) and 73 females (38.2%), were included in the study. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for identifying overall survival were 69.8%, 100%, 100% and 18.8%, respectively at the LENT score > 4 (p= 0.000). At ECOG PS >2, the sensitivity, specificity, PPV, NPV were as the same as the LENT score >4 for identifying overall survival. In all patients, overall median survival according to the LENT score was 662/119/33 days in low/moderate/high risk groups, respectively. Cox regression analysis indicated that having a moderate LENT score (p= 0.004, OR: 2.21, CI: 1.29 -3.78%) and high LENT score (p= 0.000, OR: 4, 50 CI: 2.57-7.89%) were predictors for overall survival in all patients due to MPE. In ROC analysis, there was no difference in mortality in terms of both LENT and ECOG at 1st, 6th and 12th months.
Conclusion: LENT is a better scoring system than ECOG in predicting early mortality, while both ECOG and LENT have almost the same power in predicting mortality. However, LENT is slightly more objective but more difficult to calculate because it contains laboratory findings. Thus, both scoring systems can be used to predict mortality in patients with malignant pleural effusions. Neither of them has superiority to each other.
Key words: Malignant pleural effusion; LENT; survival; prognosis
Geliş Tarihi/ Received: 25.11.2020 - Kabul Ediliş Tarihi/ Accepted: 11.03.2021
INTRODUCTION
Malignant pleural effusion (MPE) is the presence of malignant cells in the pleural fluid and/or parietal pleura (1). As the incidence of cancer and treatment advances in this area increase, the survival time of patients prolongs, and the visibility of MPE increases. MPE occurs in about 15% of all cancer patients (2). Approximately 75% of MPE are caused by breast and lung metastasis and 40% are caused only by lung cancer ((1),(3)). The presence of MPE is associated with reduced life expectancy (1). Median survival after diagnosis varies depending on the type of underlying malignancy but is reported to be 3-12 months in new guidelines ((4),(5)). As oncologic and pleural treatment options develop, accurate prognostic evaluation of malignant pleural fluid is important for planning the appropriate treatment that will benefit the patient in a survival-related manner and the damage will be minimal (6). The treatments to be applied may require hospitalization as well as morbidity and this causes an additional burden on the patient, decrease in the quality of life of the patient and an additional cost for health expenses. On the other hand, it provides good palliation in patients with long survival. The British Thoracic Society Guideline suggests that for patients with a life expectancy up to 30 days, treatment of pleural effusion should be carried out with thoracentesis as needed (5). The question here is to determine which patients will have this survival (5). Therefore, accurate prognostic evaluation of the patients is clinically important (7).
The combination of tumor characteristics, stage of the disease, comorbidities and effusion is known to be effective in predicting prognosis and survival in patients with malignant pleural disease. ((3),(8)-(13)). Inflammation-based scoring systems have been associated with survival in some cancer types including mesothelioma ((2),(14),(15)).
The LENT score (Serum Lactate dehydrogenase (LDH), Eastern Cooperative Oncology Group (ECOG) Performance Score, Blood Neutrophil/Lymphocyte Ratio, Tumor Type) is a compound scoring established and validated when investigating a stronger predictor in malignant pleural fluid developing oncology patients ((2),(8)).
The aim of this study was to evaluate the predictive power of LENT score which is a current prognostic score in patients with malignant metastasis and to determine its effect on survival and its status in clinical decision making. In addition, it was aimed to compare LENT score with the conventional but subjective score ECOG.
MATERIALS and METHODS
Study Population and Data Collection
We retrospectively reviewed all patients diagnosed with cancer who presented with malignant pleural effusion between 2008-2018 at our clinic. Patients with malignant cells confirmed in the pleural fluid or on pleural biopsy were included in the study. In order to identify malignant cells in effusion fluid and/or pleural biopsy tissue, a conventional cytology examination and/or histological analyses were performed independently. Patients with mutational drivers positive and treated with targeted therapies were excluded. The Institutional Ethical Committee approved the study (04-12-2017;12072/57776580).
Measurements
Baseline prognostic clinical and laboratory variables were collected retrospectively from the electronic medical record system. Data were collected on age, sex, side of pleural effusion, serum LDH serum protein, pleural LDH, pleural protein, pleural fluid and serum differential cell count, cytology, ECOG status, pleural biopsy result, and survival. The neutrophil/lymphocyte ratio (NLR) was calculated by dividing the blood neutrophil count by the blood lymphocyte count.
Survival time was calculated from the date of diagnostic thorasynthesis to death. Follow-up data were available for all patients at least 12 months. LENT score was calculated for each patient according to the published literature (2). The model stratifies patients into low, moderate, and high-risk groups on the basis of pleural fluid lactate dehydrogenase, Eastern Cooperative Oncology Group (ECOG) performance status, serum NLR and tumor type. Patients were divided into low-risk (score 0-1), moderate-risk (score 2-4) and high-risk (score 5-7) prognostic groups based on their LENT score calculated at the time of presentation with MPE.
Statistical Analysis
We used SPSS software, version 17 (SPSS, Chicago, IL, USA) for all statistical analyses. The results were compared using a Wilcoxon 2-sample test or Fisher exact test. p values were 2-sided and considered indicative of a significant difference if < 0.05. Overall survival (OS) was measured as an outcome and was estimated from the time of diagnosis until death as a result of any cause. Survival analysis was performed statistically according to LENT score risk grading in cases where lung carcinoma or other organs metastasized to pleura or mesothelioma histologically proven. Survival analyses were performed using the Kaplan-Meier method and log-rank test. Overall survival according to the LENT score was assessed using a Cox model. The area under the curve (AUC) was calculated for 1-month, 3-month and 6-month prediction of mortality. The results of the Cox regression modeling are presented as hazard ratios and associated 95% confidence intervals. Variables with p-values less than 0.05 were considered statistically significant.
RESULTS
Patient Characteristics
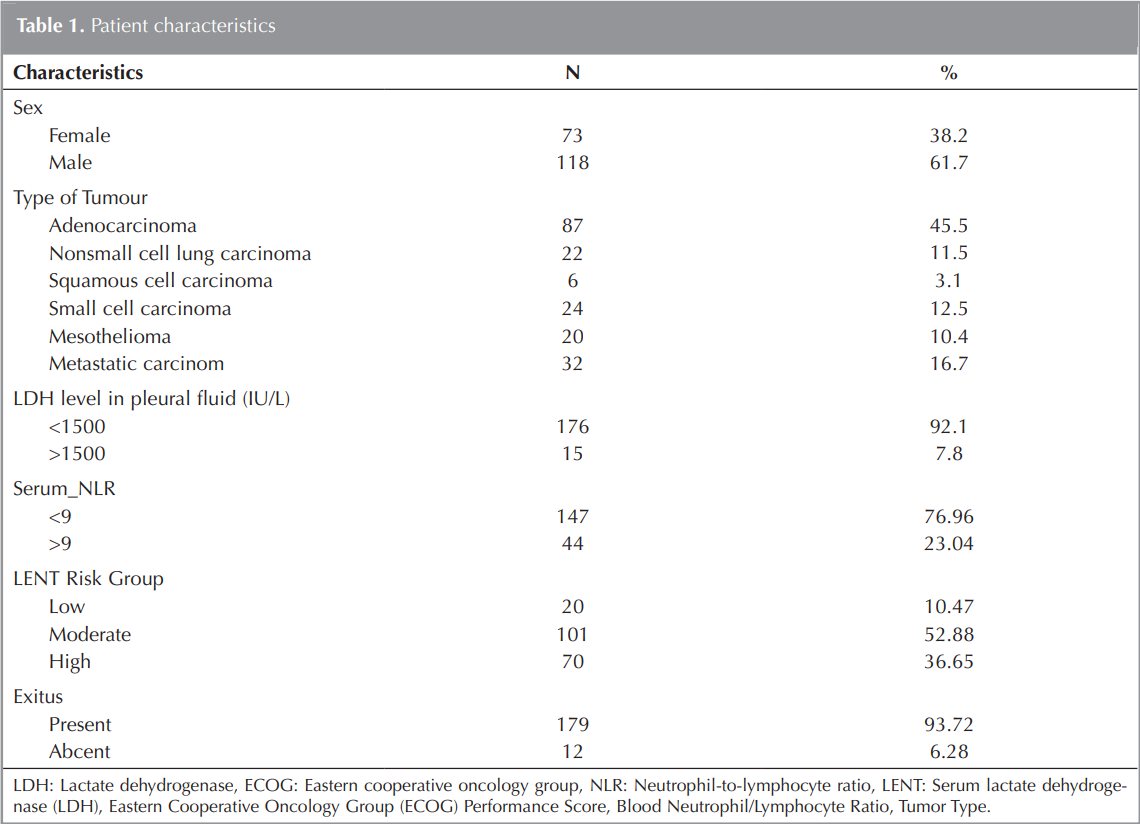
A total of 191 patients with malignant pleural effusion, 118 males (61.7%) and 73 females (38.2%), were included in the study. The general characteristics of the patients are shown in (Table 1). Pleural fluid LDH, serum neutrophil, and age were found to be significantly higher in patients with high LENT score.
LENT Score and ECOG Performance Score (PS) ROC Curve Analysis for Survival Analysis
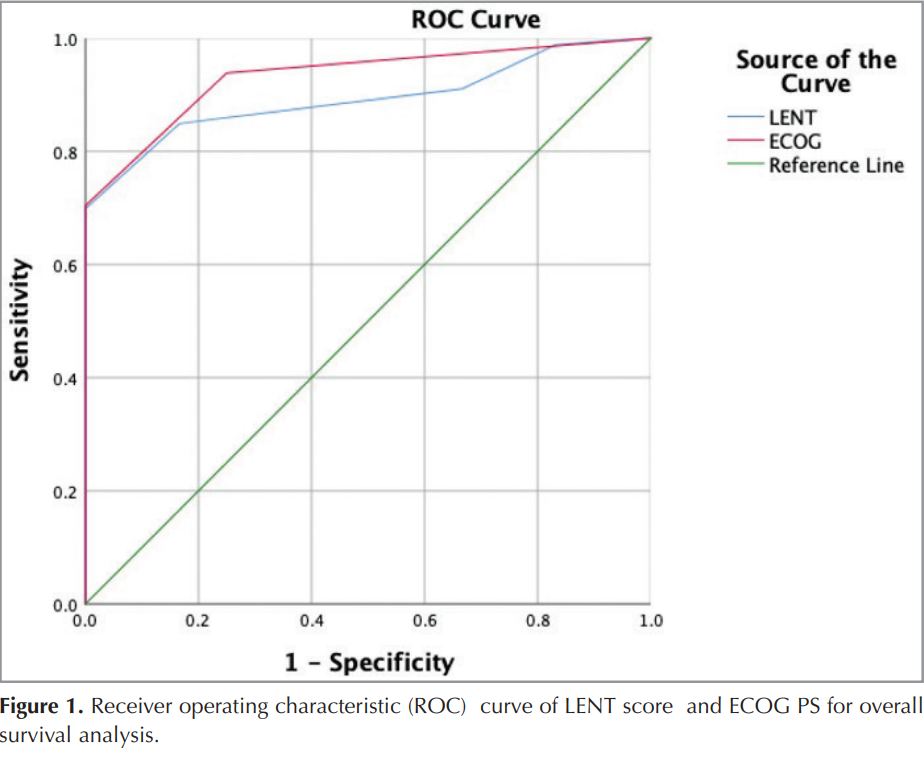
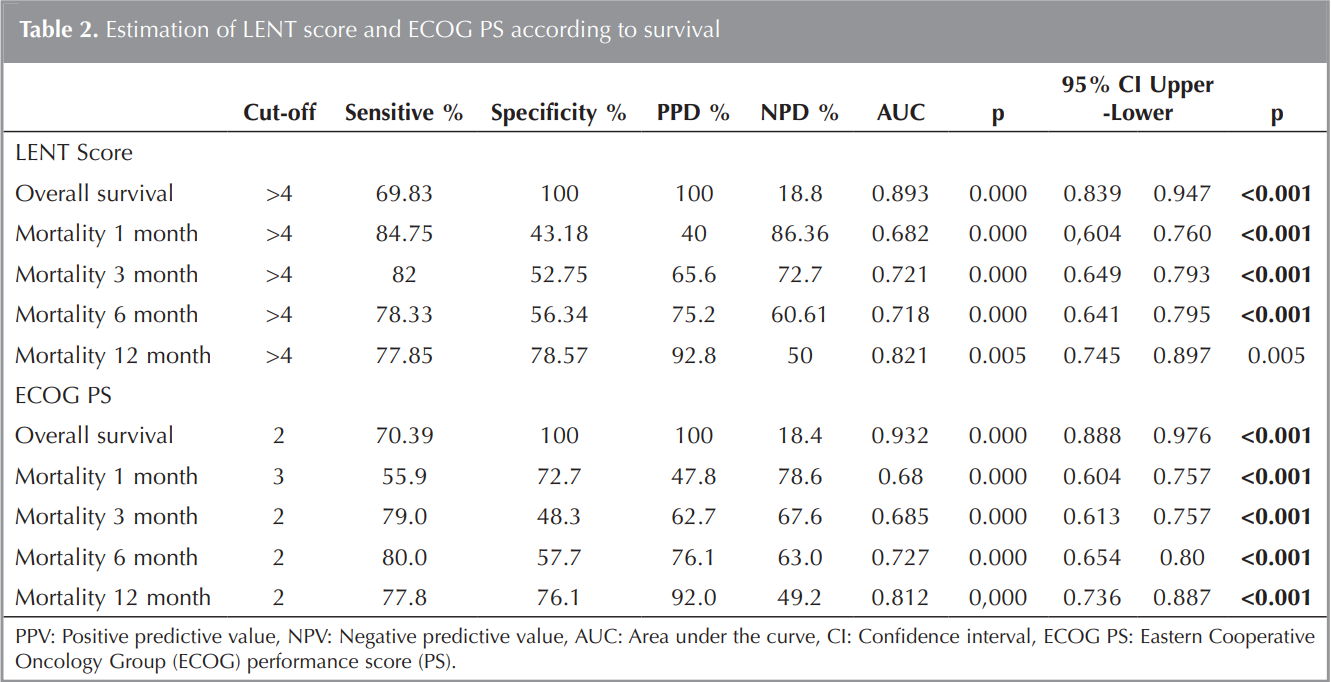
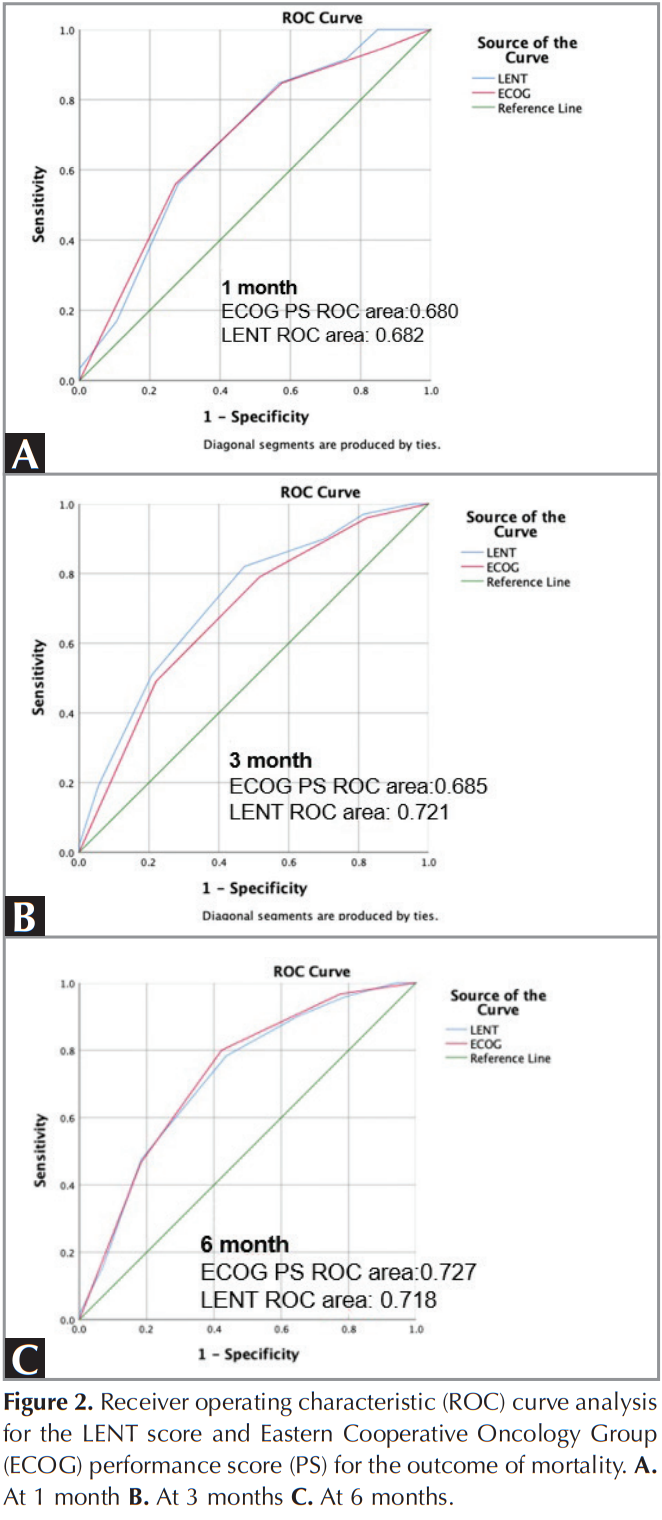
In overall survival, 179 (93.7%) patients died; 12 (6.2 %) were alive. An area under the curve (AUC) value (AUC = 0.893) and AUC= 0.932 were obtained using the LENT score and ECOG PS for overall survival analysis in all patients respectively. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for identifying overall survival were 69.8%, 100%, 100% and 18.8%, respectively at the LENT score >4 (p= 0,000). At the ECOG PS >2, the sensitivity, specificity, PPV, NPV were the same as LENT score >4 for identifying overall survival ((Figure 1), (Table 2)). The receiver operating characteristic (ROC) analysis for mortality at 1, 6 and 12 months using the LENT score gave the same AUC values as ECOG PS. At 1 month, AUC for the LENT score was 0.682 (95% CI 0.604 to 0.762) compared with 0.680 (0.60 to 0.76) for ECOG PS (p= 0.000). AUC at 3 months for the LENT score was better than ECOG PS (0.72 (0.65 to 0.79) and 0.68 (0.61 to 0.75), respectively) ((Table 2), (Figure 2)).
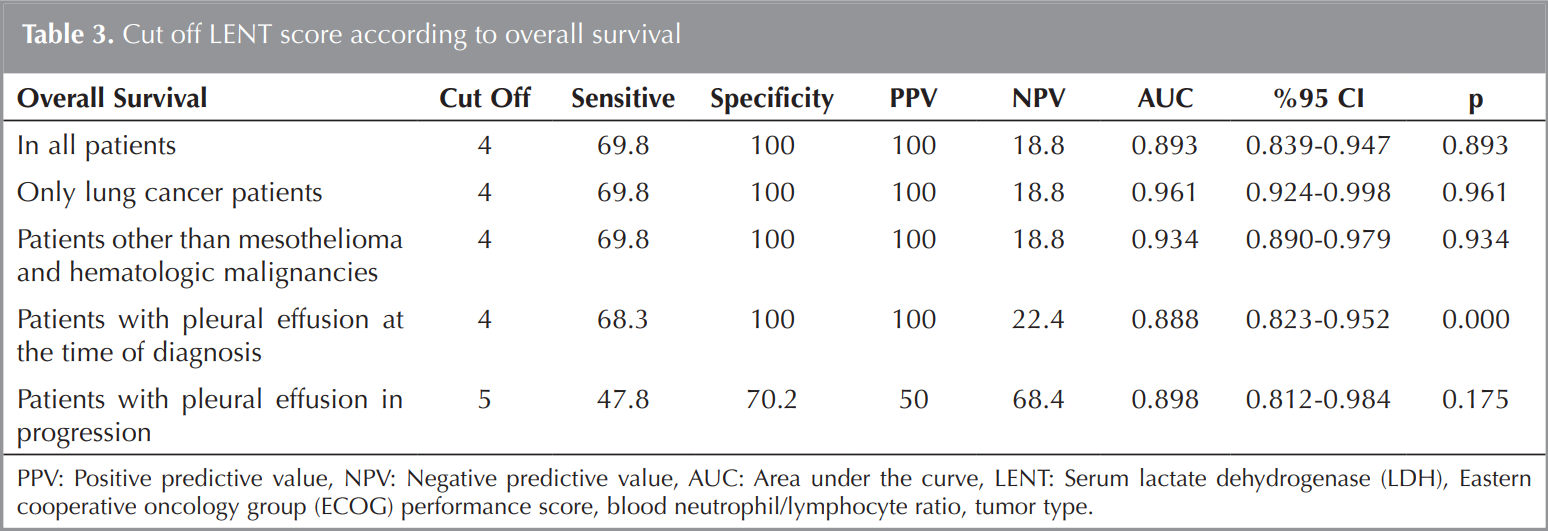
The cut off value of LENT score was 4 and the sensitivity, specificity, NPV and PPV values were found to be the same as overall survival values in patients with lung cancer only and in patients other than mesothelioma and hematologic malignancies (Table 3). Among all patients, the LENT score was 4 only in lung cancer patients, in patients other than hematologic and mesothelioma, in patients with pleural effusion at the time of diagnosis or in patients with pleural effusion in progression (Table 3).
Kaplan Meier Survival Analysis According to LENT Score
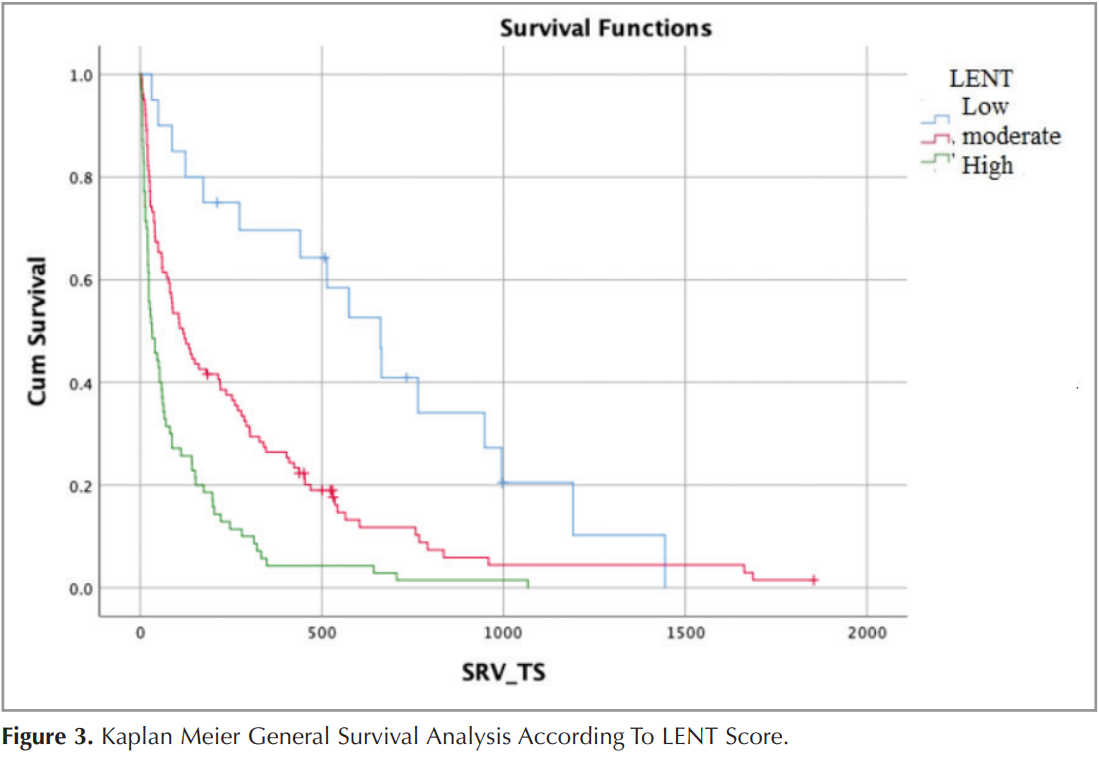
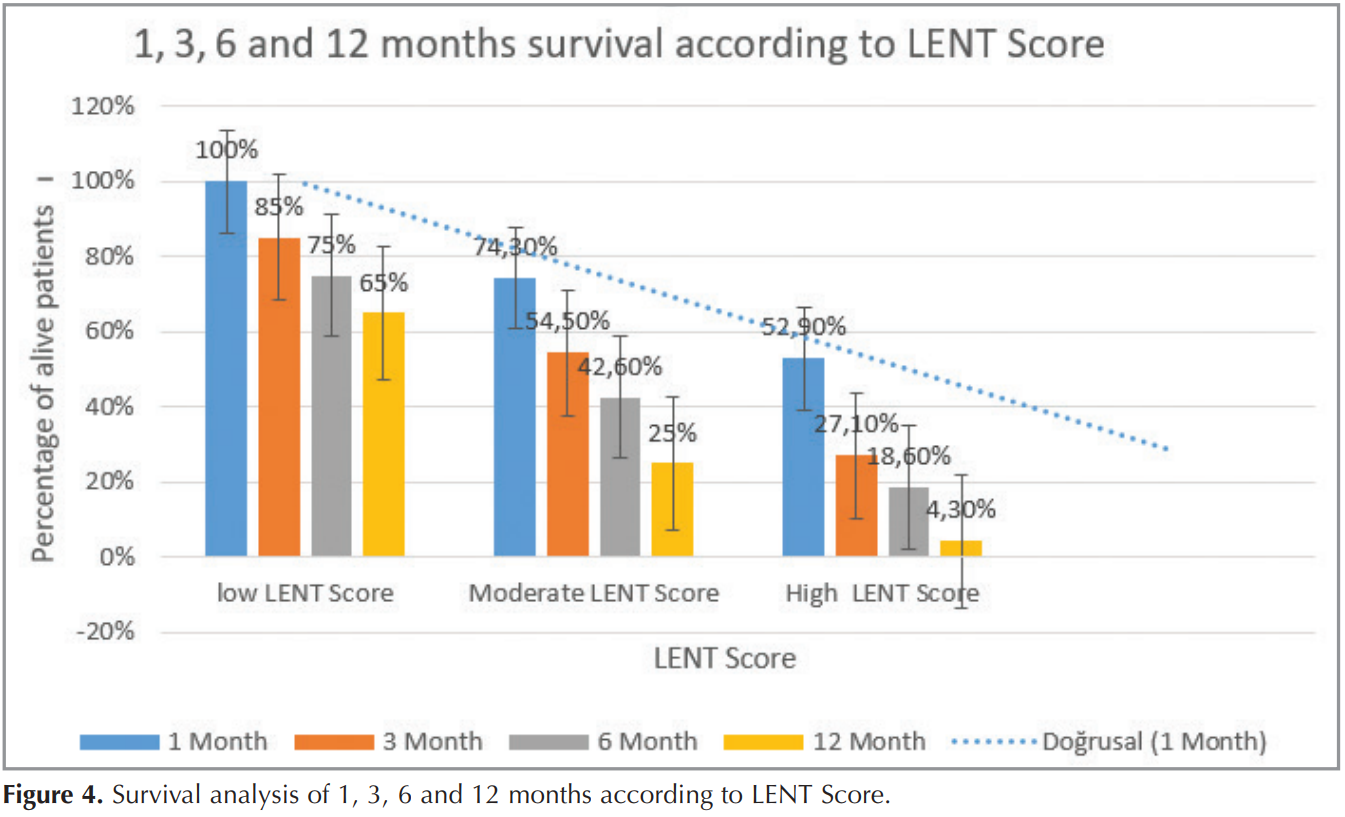
In all patients, overall median survival according to the LENT score was 662/119/33 days in low/moderate/high risk groups, respectively (Figure 3). Survival analysis for 1 month, 3 months, 6 months and 12 months according to the LENT score in all patients is also shown in (Figure 4). While the survival of 1, 3, 6 and 12 months in patients with low LENT score was 100%, 80%, 75% and 65%, in patients with moderate LENT score 74.3% up to 1 month, 54.5% up to 3 months and 42.6% survived for 6 months and 25% for 12 months. Those with a high LENT score had a 52.9%, 27.1%, 18.6% and 4.3% survival chance at 1, 3, 6 and 12 months, respectively (Figure 4).
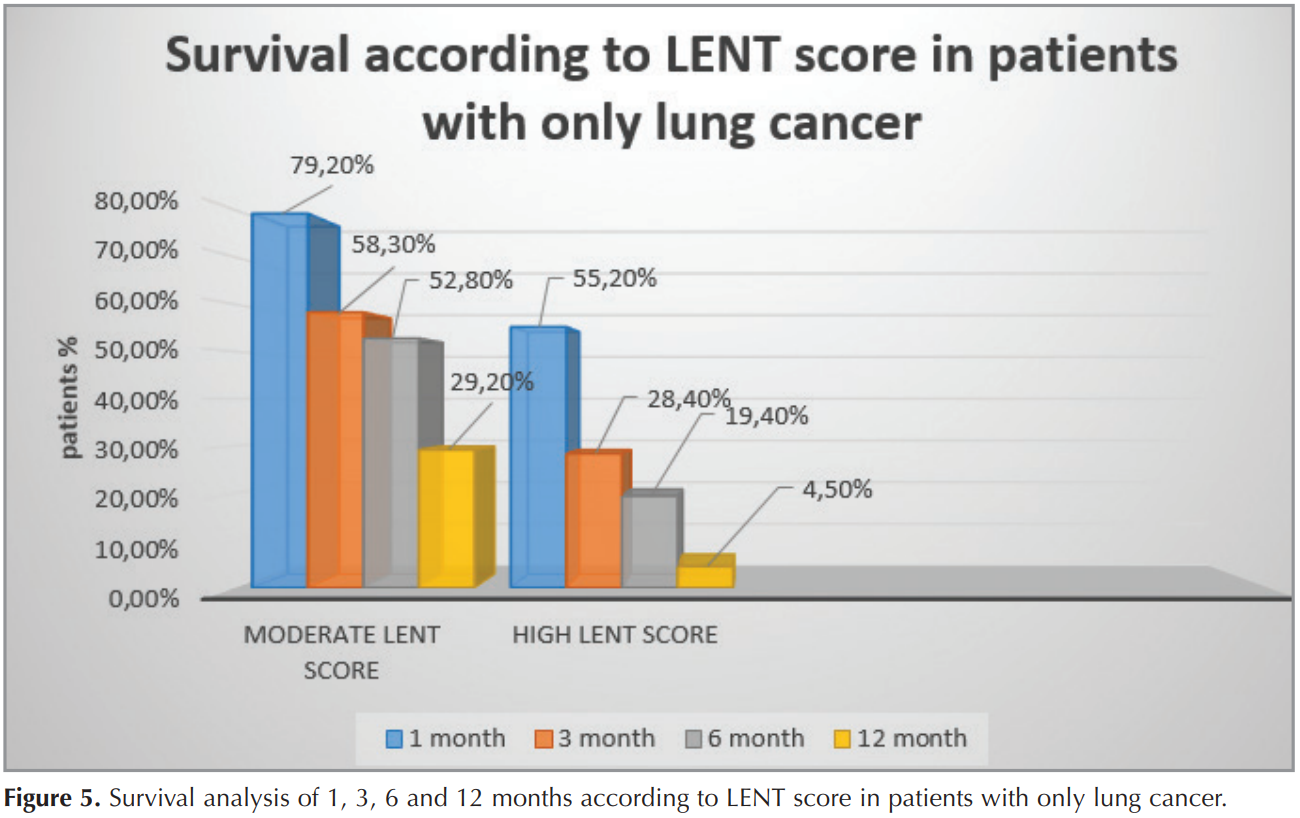
In our subgroup of patients with lung carcinoma alone, there was no patient with low LENT score as two points is given for lung carcinoma tumor type according to LENT scoring system. The patients with a moderate risk LENT score had a median survival of 215 days (955 CI 64-365; n= 72); 79.2%, 58.3%, 52.8% and 29.2% survived to 1, 3, 6 and 12 months, respectively in patients with only lung cancer patients. Those with a high-risk LENT score had a median survival of 41 days (15-66; n= 67) and 55.2% survived to 1 month, 28.4% to 3 months, 19% survived to 6 months and 4% survived to 12 months (Figure 5).
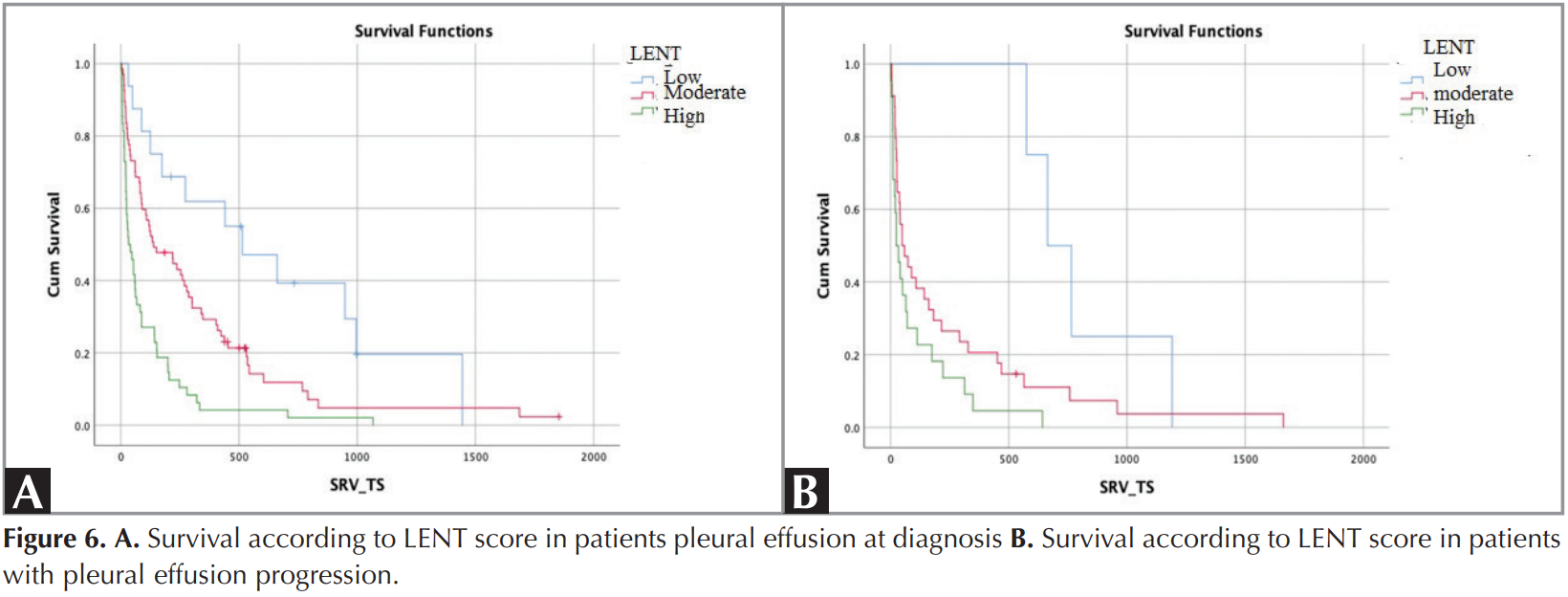
Median overall survival in patients with low, moderate and high LENT scores was 664,112 and 33 days, respectively, except for mesothelioma and hematologic malignancies. Median overall survival in pleural effusion patients at the time of diagnosis was 514, 138 and 33 days, respectively, according to the low, moderate and high LENT scores, and median survival of patients with pleural effusion at progression was 664, 50, and 24 days according to LENT score (Figure 6).
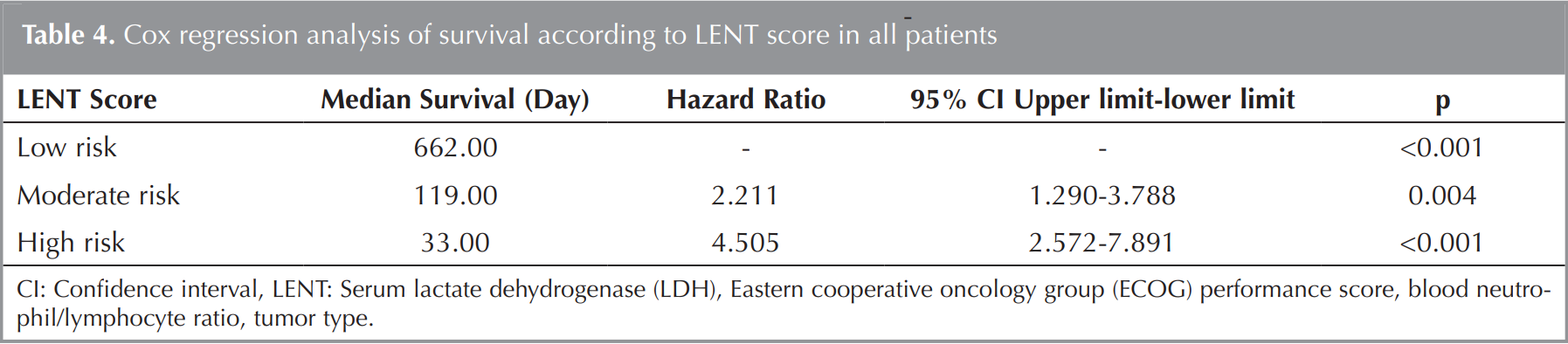
Cox regression analysis indicated that having moderate LENT score (p= 0.004, OR: 2.21, CI: 1.29 -3.78%) and high LENT score (p= 0.000, OR: 4, 50 CI: 2.57-7.89%) were predictors for overall survival in all patients due to MPE (Table 4).
DISCUSSION
In our study, we assessed the performance of LENT score in predicting prognosis in population of MPE. We found that survival time was lower in patients with high LENT score. In addition, we determined that the survival time was low in patients with malignant pleural effusions of different tumor types (not only lung cancer) with high LENT score. Furthermore, we calculated the cut off value of LENT score as 4 in malignant pleural effusions in different tumor types. Several studies have shown that performance status affects survival of cancer patients ((16),(17)). Specifically, in patients with MPE, performance status has also been associated with prognosis ((3),(9)). LENT score in patients with malignant pleural effusion is a predictor of survival. Although performance of LENT is superior to ECOG in predicting early survival, it decreases in long-term survival analysis.
In our study, we found that pleural fluid LDH levels and serum neutrophil values were high in patients with high LENT score and in those who died. Previous studies have indicated that high pleural fluid LDH levels (reflecting localized, acute inflammation, necrosis and cell death within the pleural cavity) are indicative of a poor prognosis in MPE ((9),(18)). In addition, some systematic reviews have shown that the numbers of leucocyte subtypes, specifically the neutrophil and lymphocyte counts, are objective parameters with the ability to express the severity of the systemic inflammatory response in patients with cancer ((19),(20)). These studies have reported that an elevated serum NLR has a consistent effect on adverse overall survival (OS) among patients with various solid tumors and the tumor stages. Recently, a study on the prediction of survival in patients with MPE has shown that the serum NLR is a significant prognostic factor in a multivariable analysis and that the LENT prognostic score has significantly higher accuracy than ECOG PS alone (2). Therefore, serum NLR has enormous potential as a readily available and inexpensive biomarker. Lee et al. have found that serum NLR and pleural fluid NLR scores are significant prognostic factors for adverse OS in lung cancer patients with MPE (21). In our study, LENT was superior or equal in predicting 1- and 3-months mortality. Whereas LENT score had almost the same effect as ECOG PS in terms of overall survival mortality.
In our study, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for identifying overall survival were 69.8 %, 100%, 100% and 18.8%, respectively at the LENT score >4. The development and initial validation of the LENT score on the basis of international cohorts of patients with MPE and different underlying malignancies was investigated (2). Receiver operating characteristic (ROC) analysis for mortality at 1, 3, 6 and 12 months using the LENT score gave significantly higher AUC values in our study were as the same as in their UK Cohort 2 (2). LENT score values in patients with lung cancer only and in patients other than mesothelioma and hematologic malignancies had the same AUC values in our study at the LENT score 4. This may be due to the small number of subgroups of mesothelioma and hematologic diseases. In addition, the highest risk score was “2” that was attributed to lung cancer in the LENT score may have affected this.
Histologic cell types are prognostic in patients with MPE secondary to lung cancer. Mean survival in malignant pleural effusions due to lung cancer is reported to be 6.5-8 months ((7)-(14)). Despite oncologic developments, overall survival did not change in this patient group. In the study of Clive et al., mean survival has been reported as 136 days in all patients and 74 days in patients with MPE due to lung cancer alone (2). In our study, the patients with only lung cancer had a median survival of 215 and 41 days according to moderate and high risk LENT score respectively. Also, among all patients, overall median survival according to the LENT score was 662/119/33 days in low/moderate/high risk groups, respectively. In the study of Clive et al. the patients with low, moderate and high risk groups had 319, 130 and 44 days, respectively. The difference in survival in the low-risk group may be attributed to the fact that the primary tumor type of the patients in this group was not of a similar number and that the ones with better ECOG performance status may have been referred by an oncologist for examination. In the study of Clive et al. The patients with a low-risk LENT score had a median survival of 319 days survived to 1, 3 and 6 months, respectively. Those with a moderate-risk LENT score had a median survival of 130 days and 81% survived to 1 month, 59% to 3 months and 47% survived to 6 months. Those with a high-risk LENT score who had a median survival of only 44 days (22-77, n= 31) and their chances of surviving 1, 3 and 6 months were 65%, 13% and 3%, respectively (2). In our study, the survival rates of 1, 3 and 6 months according to the LENT score were similar to those found in Clive’s study.
Another factor affecting survival is targeted therapies. The OS of patients with MPE due to lung adenocarcinoma was longer if they were treated with tyrosine kinase inhibitors (TKIs), which is best explained by the presence of EGFR mutations ((7),(22),(23)). Median survival was found longer in a study conducted in Singapore that included more than half of the patients with EGFR mutation with MPE due to pulmonary adenocarcinoma receiving TKI treatment (7). Among those who received TKI’s, median survival was 437 days, even higher than the survival reported in the “lung cancer” group by Clive et al. (2) in their LENT validation cohort. So, the authors indicated that the LENT score was found to have limitations in predicting survival in patients having MPE from lung adenocarcinoma, especially in those treated with EGFR TKI’s. Hence, they argued that LENT score may need modification before applying to such patients. In our study, patients who received targeted lung cancer treatment were excluded. Furthermore, we would like to state that the frequency of EGFR mutation in our country is not as common as in Singapore.
In our study, another factor affecting survival is the condition of MPE at the time of diagnosis or progression. According to the LENT score, in the moderate and high-risk group, median survival at the time of diagnosis was found to be longer than progression. However, we have no data about the treatment for their malignancy especially metastatic carcinoma due to the MPE. In the study of Clive et al., there was lack of data on the extent that patients had been pretreated for their malignancy as ours. They only had data for ‘UK Cohort 1’ on whether their effusion represented a new malignant diagnosis or recurrent/progressive disease. The numbers were small, but an univariable Cox model found no statistically significant difference in survival between progressive disease versus new presentations for UK Cohort 1 (HR 1.06 (95% CI 0.56 to 2.00); n= 66) (2). In our study, Cox regression analysis indicated that there was a statistically significant difference in survival between moderate and high risk groups according to LENT scores in all patients.
LENT prognostic score is a simple score that is possible in patients in whom pleural fluid analysis is available. Factors such as the severity of symptoms and access to care are other important factors to consider in choosing between pleurodesis and less invasive interventions, especially in high-risk patients. LENT prognostic score can be used to guide decision‑making in the treatment of MPE, especially in routine clinical care (24). According to the results of our study, the clinical use of LENT can be considered as repeated thoracentesis or supportive treatment in patients with a LENT score of 4 and above, and surgery or intrapleural catheter application in patients with a LENT score below 4.
The limitations of our study include the small sample size of metastatic carcinoma and the retrospective design.
CONCLUSION
In conclusion, the LENT score is the first approved risk classification system in MPE and may be useful in clinical practice in predicting survival. LENT is a better scoring system than ECOG in predicting early mortality, while both ECOG and LENT have almost the same power for in predicting mortality. However, LENT is slightly more objective but more difficult to calculate because it contains laboratory findings. Thus, both scoring systems can be used to predict mortality in patients with malignant pleural effusions. Neither of them has superiority to each other. In the future, changes in adenocarcinoma treatment are likely to occur, so other prognostic scoring systems or modifications will be needed considering ethnic mutation differences.
Ethical Committee Approval: The approval for this study was obtained from Dr. Suat Seren Chest Diseases and Surgery Training and Research Hospital Ethical Committee (Decision no: 5128, Date: 10.07.2018).
CONFLICT of INTEREST
The authors of this meta-analysis declare that they have no conflict of interest.
AUTHORSHIP CONTRIBUTIONS
Concept/Design: MG, CA, BD
Analysis/Interpretation: CA, MC, BD
Data Acqusition: AEE, FG
Writing: CA, FG
Clinical Revision: CA, BD
Final Approval: MG, MC
REFERENCES
- Kasapoglu U, Arınç S, Gungor S, Irmak I, Guney P, Aksoy, et al. Prognostic factors affecting survival in non-small cell lung carcinoma patients with malignant pleural effusions. Clin Respir J 2015; 10: 791-9.
- Clive AO, Kahan BC, Hooper CE, Bhatnagar R, Morley AJ, Evans NZ, et al. Predicting survival in malignant pleural effusion: development and validation of the LENT prognostic score. Thorax 2014; 69(12): 1098-104.
- Anevlavis S, Kouliatsis G, Sotiriou I, Koukourakis MI, Archontogeorgis K, Karpathiou G, et al. Prognostic factors in patients presenting with pleural effusion revealing malignancy. Respiration 2014; 87(4): 311-6.
- Bibby AC, Dorn P, Psallidas I, Porcel JM, Janssen J, Froudokıs M, et al. ERS/EACTS statement on the management of malignant pleural effusions. Eur J Cardiothorac Surg 2019; 55(1): 116-32.
- Roberts ME, Neville E, Berrisford RG, Antunes G, Ali JN. Management of a malignant pleural effusion: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65(Suppl 2): ii32-40.
- Tan C, Sedrakyan A, Browne JS, Swift S, Treasure T. The evidence on the effectiveness of management for malignant pleural effusion: a systematic review. Eur J Cardiothorac Surg 2006; 29(5): 829-38.
- Abisheganaden J, Verma A, Dagaonkar RS, Light RW. An observational study evaluating the performance of LENT score in the selected population of malignant pleural effusion from lung adenocarcinoma in Singapore. Respiration 2018; 96(4): 308-13.
- Ozyurtkan MO, Balci AE, Cakmak M. Predictors of mortality within three months in the patients with malignant pleural effusion. Eur J Intern Med 2010; 21(1): 30-4.
- Bielsa S, Salud A, Martinez M, Esquardo A, Martin A, Panadore FR, et al. Prognostic significance of pleural fluid data in patients with malignant effusion. Eur J Intern Med 2008; 19(5): 334-9.
- Pilling JE, Dusmet ME, Ladas G, Goldstraw P. Prognostic factors for survival after surgical palliation of malignant pleural effusion. J Thorac Oncol 2010; 5(10): 1544-50.
- Burrows CM, Mathews WC, Colt HG. Predicting survival in patients with recurrent symptomatic malignant pleural effusions: an assessment of the prognostic values of hysiologic, morphologic, and quality of life measures of extent of disease. Chest 2000; 117(1): 73-8.
- Zamboni MM, da Silva CT Jr, Baretta R, Cunha ET, Cardoso GP. Important prognostic factors for survival in patients with malignant pleural effusion. BMC Pulm Med 2015; 15: 29.
- Heffner JE, Nietert PJ, Barbieri C. Pleural fluid pH as a predictor of survival for patients with malignant pleural effusions. Chest 2000; 117(1): 79-86.
- Pinato DJ, Mauri FA, Ramakrishnan R, Wahap L, Lyold T, Sharma R. Inflammation-based prognostic indices in malignant pleural mesothelioma. J Thorac Oncol 2012; 7(3): 587-94.
- Proctor MJ, Morrison DS, Talwar D, Balmer SM, Fletcher CD, O’Reilly SD, et al. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur J Cancer 2011; 47(17): 2633-41.
- Su J, Barbera L, Sutradhar R. Do repeated assessments of performance status improve predictions for risk of death among patients with cancer? A population-based cohort study. Palliat Med 2015; 29(6): 547-53.
- Nishikawa H, Kita R, Kimura T, Ohara Y, Sakamoto A, Saito S, et al. Clinical implication of performance status in patients with hepatocellular carcinoma complicating with cirrhosis. J Cancer 2015; 6(4): 394-402.
- Martinez-Moragon E, Aparicio J, Sanchis J, Menendez R, Rogado MC, Sanchis F. Malignant pleural effusion: prognostic factors for survival and response to chemical pleurodesis in a series of 120 cases. Respiration 1998; 65(2): 108-13.
- Paramanathan A, Saxena A, Morris DL. A systematic review and metaanalysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumours. Surg Oncol 2014; 23(1): 31-9.
- Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil-lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol 2013; 88(1): 218-30.
- Lee YS, Nam HS, Lim JH, Kim JS, Moon Y, Cho JH, et al. Prognostic impact of a new score using neutrophil-to-lymphocyte ratios in the serum and malignant pleural effusion in lung cancer patients. BMC Cancer 2017; 17(1): 557.
- Yang J, Lee OJ, Son SM, Woo CG, Jeong Y, Yang Y, et al. EGFR mutation status in lung adenocarcinoma-associated malignant pleural effusion and efficacy of EGFR tyrosine kinase inhibitors. Cancer Res Treat 2018; 50(3): 908-16.
- Wu SG, Yu CJ, Tsai MF, Liao WY, Yang CH, Jan IS, et al. Survival of lung adenocarcinoma patients with malignant pleural effusion. Eur Respir J 2013; 41(6): 1409-18.
- Murray J, Turner R, Bothamley GH, Bhowmik A. A response to the LENT score. Thorax 2014; 69(12): 1144.
Yazışma Adresi (Address for Correspondence)
Dr. Betül İkbal DOĞAN
Dr. Suat Seren Göğüs Hastalıkları ve Cerrahisi Eğitim ve Araştırma Hastanesi,
Göğüs Hastalıkları Kliniği,
İZMİR - TÜRKİYE.
E-mail: betuldogan1993@hotmail.com