RESEARCH ARTICLE
Tuberk Toraks 2019;67(1):15-21
Fleksibl bronkoskopik kriyoekstraksiyon uygulamaları rijit bronkoskopiye bir alternatif mi?
Cengiz ?ZDEMİR1, Sinem Nedime S?K?C?1, Celalettin İbrahim KOCAT?RK2, Kaan KARA1, Seda TURAL ?N?R1, Sedat ALTIN1, Levent DALAR3
1 İstanbul Yedikule G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği, İstanbul, T?rkiye
1 Clinic of Chest Diseases, Istanbul Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey.
2 İstanbul Yedikule G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, G?ğ?s Cerrahisi Kliniği, İstanbul, T?rkiye
2 Clinic of Chest Surgery, Istanbul Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey.
3 Bilim ?niversitesi Avrupa Florence Nightingale Hastanesi, G?ğ?s Hastalıkları Anabilim Dalı, İstanbul, T?rkiye
3 Department of Chest Diseases, Bilim University, Europe Florence Nightingale Hospital, Istanbul, Turkey
?ZET
Fleksibl bronkoskopik kriyoekstraksiyon uygulamaları rijit bronkoskopiye bir alternatif mi?
Giriş: Hava yolu obstr?ksiyonunun altta yatan nont?m?ral nedenleri arasında yer alan kan pıhtısı ve mukus plaklarının tedavisinde fleksibl bronkoskopik girişimler ilk tercih edilecek y?ntemdir. Fakat bazı hastalarda rijit bronkoskopik girişime ihtiya? duyulmaktadır.? Bronkoskopik kriyoekstraksiyon, benign ve malign endoluminal lezyonlar yanında yabancı cisim, kan pıhtıları ve sekresyon gibi benign nedenlere bağlı hava yolu obstr?ksiyonlarında etkindir. Bizde fleksibl bronkoskop eşliğinde yapılan kriyoektraskiyonun mukus plak ve kan pıhtısına bağlı gelişen hava yolu obstr?ksiyonundaki etkinliğini ve deneyimimizi sunmayı ama?ladık.
Materyal ve Metod: ?alışmada girişimsel pulmonoloji ?nitesine Ocak 2013-Kasım 2017 tarihleri arasında başvuran, daha ?nce yapılan fleksibl bronkoskopi ile santral hava yolundaki sekresyon ve kan pıhtılarının temizlenemediği ve fleksibl bronkoskopik kriyoekstraksiyon uygulanan hastaların verileri değerlendirildi.
Bulgular: ?alışmaya yaş ortalaması 58.29 ? 18.56 (28-76) olan 7 hasta alındı. ?? hastaya yoğun bakım ?nitesinde yatak başı, 4 hastaya bronkoskopi odasında işlem yapıldı. Yedi hastaya toplamda 9 seans kriyoekstraksiyon uygulandı. Kriyoekstraksiyon seansları sırasında ciddi bir komplikasyon ve mortalite izlenmedi. Girişim ile hastaların hepsinde tam hava yolu a?ıklığı sağlandı ve hi?birinde rijit bronkoskopik girişime ihtiya? olmadı.
Sonu?: Fleksibl bronkoskopi eşliğinde yapılan kriyoekstraksiyon, kan pıhtısı ve mukus plakları ile oluşan hava yolu obstr?ksiyonlarının tedavisinde etkin bir y?ntemdir. Bu y?ntem diğer fleksibl bronkoskopik girişimlerle hava yolu a?ıklığının sağlanamadığı hastalarda, rijit bronkoskopiye alternatif bir tedavi stratejisi olarak uygulanabilen g?venli bir y?ntemdir.
Anahtar kelimeler: Fleksibl bronkoskopi, kriyoekstraksiyon, mukus plak, kan pıhtısı
SUMMARY
Are flexible bronchoscopic cryoextraction practices an alternative to rigid bronchoscopy?
Introduction: We aimed to evaluate the efficacy of flexible bronchoscopic cryoextraction in the treatment of airw ay obstruction arise from mucus plugs and blood clots and present our experience.
Materials and Methods: The present study evaluated patients who previously underwent unsuccessful flexible bronchoscopy for the removal of secretions and blood clots in the central airway and who underwent flexible bronchoscopic cryoextraction between January 2013-November 2017.
Results: The study included seven patients with a mean age of 58.29 ? 18.56 years (28-76). Three patients underwent bedside intervention in the intensive care unit, and four patients underwent an intervention in the bronchoscopy unit. Seven patients underwent a total of nine sessions of cryoextraction. Severe complications or mortality did not occur during the cryoextraction sessions.
Conclusion: Flexible bronchoscopic cryoextraction offers a safe treatment strategy as an alternative to rigid bronchoscopy in patients in whom airway patency cannot be achieved using other flexible bronchoscopic interventions. and accuracy of PET was higher compared to CT with this cut-off value.
Key words: Flexible bronchoscopy, cryoextraction, mucus plug, blood clot
Geliş Tarihi/Received: 29.05.2018 - Kabul Ediliş Tarihi/Accepted: 17.02.2019
INTRODUCTION
Airway obstruction caused by benign and malignant causes is a life-threatening condition and patients may require emergency bronchoscopic interventions that depend on the degree of airway obstruction. Blood clots and mucus plugs that complicate the drainage of secretions are among the nontumoral underlying causes of airway obstruction and these are not rare conditions. Restoring the patency of the airway through bronchoscopic interventions in patients with airway obstruction caused by blood clots and mucus plugs is the first step in rectifying respiratory problems that occur to varying degrees. Other methods used for this purpose include bronchoscopic aspiration, extraction using grasping basket or forceps, Fogarty catheter, and topical thrombolytic applications. Although flexible bronchoscopy is the first-choice method for restoring airway patency, the removal of mucus plugs and blood clots is not always possible with flexible bronchoscopy (1-3). In this regard, rigid bronchoscopic interventions may be useful in effectively establishing airway patency. However, the use of rigid bronchoscopy has some disadvantages as it depends on the operator?s experience, requires general anesthesia, equipment and an operating room.
Cryotherapy performed using probe cryotherapy and cryoextraction methods involving freeze-thaw cycles is used with bronchoscopy to treat benign and malignant causes of airway obstructions (4). Among these methods, cryoextraction involves the adhesion of the probe to the target tissues and extraction due to the cryo-adhesive features of cold. Along with benign and malignant endoluminal lesions, cryoextraction may also be performed to treat benign causes of airway obstruction, such as foreign body, blood clots and secretion. Cryoextraction could be performed under rigid bronchoscope; however, it could also be performed under flexible bronchoscope using a flexible probe, and this minimizes the need for using rigid bronchoscope (3).
?We aimed to evaluate the efficacy of flexible bronchoscopic cryoextraction in the treatment of airway obstruction caused by mucus plugs and blood clots in bronchoscopy and intensive care units and present our experience.
MATERIALS and METHODS
Our hospital is a tertiary health care facility, and various bronchoscopic procedures have been performed at the interventional pulmonology unit since 2005 in the treatment of benign and malignant causes of central airway obstruction. As being one of these methods, cryotherapy is performed both under rigid and flexible bronchoscopy. The present study evaluated patients who previously underwent unsuccessful flexible bronchoscopic intervention for the removal of secretions and blood clots in the central airway and who were scheduled for rigid bronchoscopy between January 2013-November 2017. Among these patients, those undergoing cryoextraction under flexible bronchoscope without using rigid bronchoscopy were included in the present study. Approval of the local ethics committee was obtained for this study (1139/15.12.2017). A written informed consent was obtained from the patients or their legal guardians. Demographic characteristics, diagnoses, place of procedure, procedural success and complications were retrieved from the medical charts of the patients. Patients that underwent rigid bronchoscopy were excluded from the study.
Bronchoscopy Procedure
Bronchoscopy procedure was performed in the bronchoscopy unit, or bedside bronchoscopy was performed in the intensive care unit. All patients underwent standard cardiovascular monitorization during bronchoscopy. The interventions were performed through the mouth, endotracheal tube or tracheostomy cannula after local anesthesia. Outpatients did not receive sedation during the bronchoscopy. Patients connected to the mechanical ventilator in the intensive care unit received deep sedation with intravenous propofol administration by the anesthesia specialist during bronchoscopy. Bronchoscopy was performed with a flexible bronchoscope (Olympus BF-TE2, Japan) and cryotherapy was performed with the ERBOKRYO system (Elektromedizine GBMH, T?bingen, Germany) and 1.9-mm flexible cryoprobe. Oxygen was delivered to the patients during bronchoscopy. The inspired oxygen (FiO2) was set to 100% during the procedure in patients connected to the mechanical ventilator. After inspecting the airway with a flexible bronchoscope, the cryoprobe was advanced through the working channel, and the probe was protruded > 5 mm outside the distal tip of the scope. The probe was applied to the blood clot, and mucus plugs and the probe tip was cooled for 10 seconds by pressing the foot switch. Care was taken to avoid contact of the probe with airway mucosa while cooling. After cooling, probe and coagulum/mucus plugs adhered to the probe were removed en bloc. The foot switch was released after removing the clot from the airway, and distal tip of the probe was dipped into the saline solution to accelerate melting. After melting, the probe was removed from the working channel and then re-introduced with the bronchoscope into the airway. The procedure was repeated if residual secretion or clots were observed in the lumen. The procedure was completed after achieving airway patency. Blood pressure, heart rate and oxygen saturation were monitored during and after the procedure.
Procedure-related desaturation, hypo/hypertension and the amount of bleeding were recorded if any. The procedure was considered successful if complete airway patency was achieved.
Statistical Analysis
The SPSS 16.0 software (Chicago, IL, USA) package was used in the statistical analysis. Descriptive statistics included mean ? standard deviation and percentage.
RESULTS
During the study period, 120 patients with airway obstruction caused by benign and malignant etiologies underwent a total of 180 cryotherapy sessions using flexible or rigid bronchoscope at the interventional pulmonology unit. Of these patients, 28 underwent cryoextraction due to mucus plug/blood clot/foreign body in the airway and 21 patients were excluded from the study as they underwent rigid bronchoscopic intervention. The study included seven patients who previously underwent unsuccessful flexible bronchoscopic intervention and who subsequently underwent flexible bronchoscopic cryoextraction for restoring airway patency.
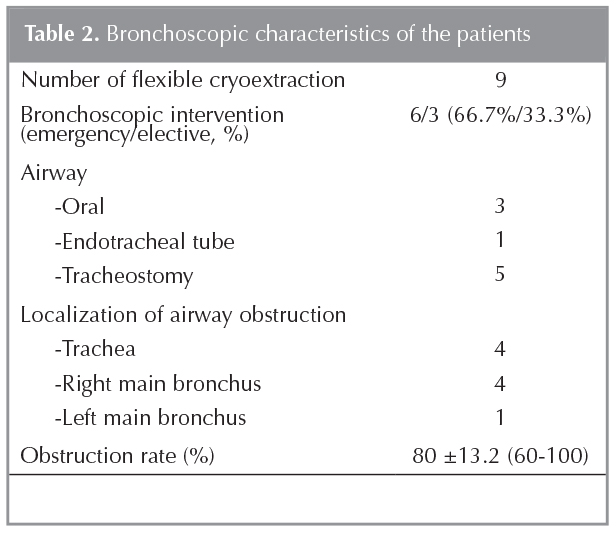
The mean age was 58.29 ? 18.56 years (28-76) and 57.1% of the patients were male (Table 1). Seven patients underwent a total of 9 sessions of cryoextraction. In these patients, cryoextraction was performed at the bedside in three patients and in the bronchoscopy room in four patients. Of these patients, two patients with lung cancer were under monitorization in the postoperative intensive care unit due to respiratory failure that occurred following thoracotomy, three underwent tracheal silicone stent implantation due to post-intubation tracheal stenosis, one patient was intubated due to massive hemoptysis, and one patient had indwelling tracheostomy tube after being operated for laryngeal carcinoma.
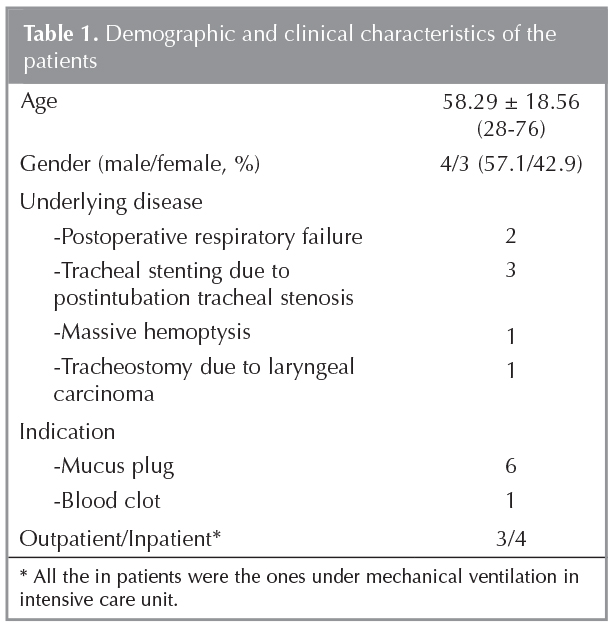
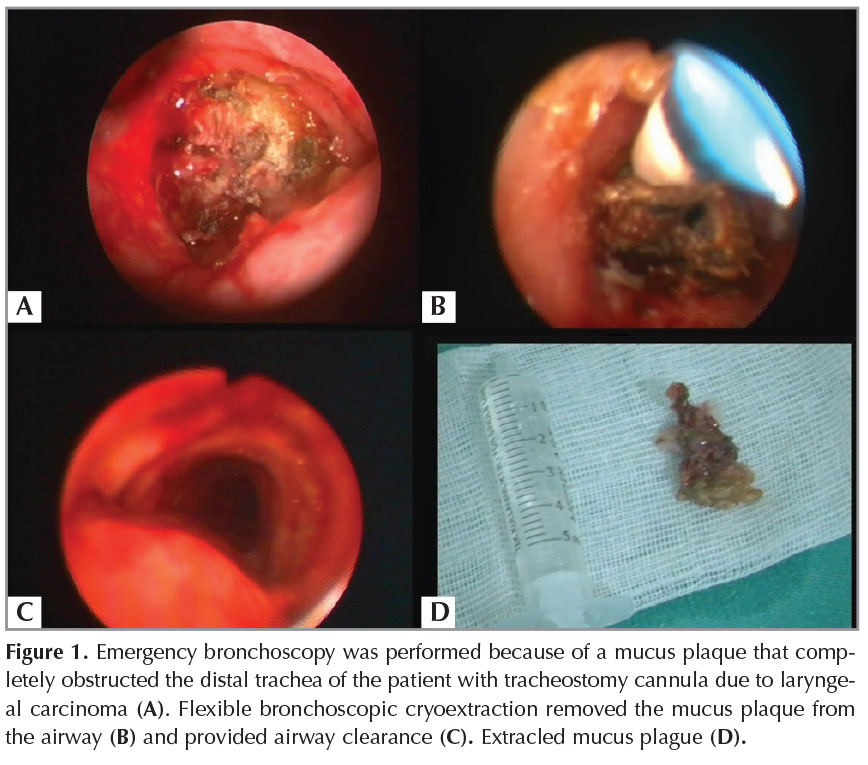
Six patients had developed airway obstruction caused by mucus plug, and one patient had airway obstruction caused by blood clots developing after massive hemoptysis. The emergency intervention was performed in 66.7% of the patients due to clinical and laboratory findings caused by ventilation disorder. The route of cryoextraction and localization of the lesions are summarized in Table 2. The interventions were most commonly performed through the tracheostomy tube, and the lesions were mostly located in the trachea and right main bronchus. Blood clots and mucus plugs caused a mean 80 ? 13.2% (60-100) obstruction of the airway (Figure 1). No severe procedure-related complications or mortality were observed during the cryoextraction sessions. Complete airway patency was achieved with the intervention in all patients. The rigid bronchoscopic intervention was not required in any patient.
DISCUSSION
The present study showed that blood clots and mucus plugs that cause airway obstruction could be removed and airway patency could be achieved using flexible bronchoscopic cryoextraction. Flexible bronchoscopic cryoextraction eliminates the need for rigid bronchoscopic interventions in the emergency treatment of airway obstruction caused by nontumoral causes, but it is also a safe and efficient method as a bedside application in the intensive care unit.
Cryotherapy was used for the first time in 1968 as an endobronchial intervention with rigid bronchoscopy, and currently, it is used in a wide range of bronchoscopic interventions. Endobronchial and transbronchial cryobiopsy has utility in the diagnosis of lung diseases, whereas its efficacy has also been shown in malignant and benign endobronchial tumors. The cryogenic temperature delivered by the cryogenic gas distal to the flexible or rigid probe is the basis of cryotherapy applications. Nitric oxide and carbon-dioxide are the most commonly used cryogenic gases in bronchoscopic interventions. Cryogenic gas is capable of delivering a cryogenic temperature of approximately -89?C distal to the probe. When compared with other thermal methods performed through endobronchial routes, such as laser and electrocautery, its effects occur in a late period within hours and days (5). Cryotherapy is used in the emergency treatment of airway obstructions for bronchoscopic cryorecanalization (6).
Many case reports and studies have been reported in the literature regarding the use of flexible bronchoscopic cryoextraction for the removal of foreign bodies, blood clots and secretions (7-12). Among these studies, a retrospective study of 38 flexible cryoextraction sessions reported by Sriratanaviriyakul et al. is the largest series of patients reported in the literature (3). Their study included patients with blood clots (n= 20), airway secretions (n= 5), foreign body aspirations (n= 4), and plastic bronchitis (n= 1). Airway patency was achieved in 84.2% of the cases and complications occurred only in one patient. Bronchoscopic cryotherapy applications are generally considered as safe methods, although hemorrhage, pneumothorax and mediastinal emphysema are among the complications that can occur. The majority of these complications occur during biopsy and extraction interventions to the endoluminal tumoral lesions in the airway (3). Cryoextraction achieved airway patency in all patients with airway obstruction caused by blood clots, and mucus plugs and no procedure-related complications were observed. During the study, cryoextraction was performed in seven cases with foreign body aspiration. However, these patients were not included in this study as these patients underwent rigid bronchoscopic interventions.
Mechanical ventilatory support in the intensive care unit, tracheostomy and thoracotomy are the most important risk factors for the development of mucus plugs (13-15). Although flexible bronchoscopy is the first-choice method in the management of these patients, rigid bronchoscopic remains as the single option where other options fail to achieve airway patency. The transport of intensive care unit patients connected to the mechanical ventilator to the operating room for bronchoscopic intervention and the need for general anesthesia entail important risks for critically-ill patients. The ability to perform flexible bronchoscopic cryoextraction at the bedside and a lesser dependence on operator experience compared to rigid bronchoscopy are the advantages of flexible bronchoscopic cryoextraction. Other important points to consider in flexible bronchoscopic cryoextraction applications include the use of an appropriate-size bronchoscope with a diameter of working channel that allow passage of the probe, outer diameter of flexible bronchoscope being smaller than inner diameter of endotracheal tube-tracheostomy cannula, and the use of the oral route for intervention as nonintubated patients may require repeated insertions into the airway (3).
Silicone or metal stenting is performed in appropriate patients with benign and malignant central airway obstruction, and these patients require close follow-up for complications that may occur in relation to airway stents. The development of mucus plugs due to the compromised drainage of airway secretions is a common complication of airway stenting, and this requires repeated bronchoscopic interventions by causing stent obstruction (16,17). Mucus plugs increase the risk of developing lower airway infections due to compromised drainage of secretions, and mucus plugs have been shown to be a risk factor for the development of stent-related granulation tissue (18). Patients being monitored after stent implantation to the airway should undergo evaluation of the airway if they develop sudden-onset dyspnea, severe cough and show findings of pneumonia due to compromised drainage of secretions. This would allow diagnosing stent-related mucostasis, granulation tissue formation and airway obstruction caused by tumor invasion, and thereby prompting therapeutic interventions. Rigid bronchoscopic interventions are required if flexible bronchoscopy fails to achieve airway patency. In the present study, three patients underwent silicone stent implantation to the airway due to inoperable post-intubation tracheal stenosis, and they developed airway obstruction caused by stent-related mucus plugs. There are an increasing number of patients treated with airway stenting, and therefore, stent-related complications occur more frequently in daily practice. Flexible bronchoscopic cryoextraction could be an important option in the removal of retained secretions and mucus plugs without the need for rigid bronchoscopic intervention. It is expected that flexible bronchoscopic cryoextraction will be common practice in bronchoscopy and intensive care units as compared with rigid bronchoscopy it is less dependent on experience.
Retained blood clots related to massive hemoptysis caused by various etiologic factors may further aggravate the clinical condition by compromising ventilation (8). Bronchoscopic aspiration may aggravate bleeding during the removal of the blood clot from the airway, and it may not always be useful in removing the blood clot. The cryoextraction of blood clots both increases the success rate due to adhesion of the freezing probe to the blood clot because of its fluid content, and helps control the bleeding due to vasoconstrictive properties (8). In our series of patients, cryoextraction was performed in one patient who was intubated and followed in the intensive care unit after sustaining massive hemoptysis. Although rigid bronchoscopic interventions are generally preferred in the control of hemoptysis, bronchoscopy was performed in this patient only to remove the clot that caused ventilation disorder, and flexible cryoextraction was preferred for this purpose. However, we should consider that the removal of blood clots with aspiration or cryoextraction may cause rebleeding in patients with massive hemoptysis in whom hemostasis has been achieved and bleeding has been controlled with coagulum formation. The authors consider that rigid bronchoscopy would offer a safer approach to clot removal if localization of the bleeding site in massive hemoptysis is intended and bronchoscopic therapeutic interventions are planned.
In one study, diagnostic efficacy of cryobiopsy through flexible bronchoscopy was shown to be superior then forceps biopsy. Use of cryobiopsy can be a rational option in cases? with exophytic airway lesions and also in cases in which forceps biopsy is nondiagnostic. Flexible bronchoscopic cryoextraction can be though as a method to be used in central airway lesions in which conventional bronchoscopic interventions are ineffective in diagnosis and treatment (19).
The most important limitation of our study is the limited number of patients. However, the cryoextraction of blood clots and secretions is already performed in patients in whom other flexible bronchoscopic methods failed to achieve success, which seems to be the most important reason for the small number of patients even though this study covered a long period (3).
Conclusion
Flexible bronchoscopic cryoextraction is a safe method that could be used as an alternative to other flexible bronchoscopic methods that fail to treat of airway obstruction caused by blood clots and mucus plugs and it offers a treated strategy aimed to decrease the need for rigid bronchoscopic interventions.
CONFLICT of INTEREST
The authors reported no conflict of interest related to this article.
AUTHORSHIP CONTRIBUTIONS
Concept/Design: C?, SNS
Analysis/Interpretation: C?, SNS, SA
Data Acquisition: CİK, KK, ST?
Writting: C?, SNS
Critical Revision: CİK, SA, LD
Final Approval: All of authors.
REFERENCES
- Arney KL, Judson MA, Sahn SA. Airway obstruction arising from blood clot: three reports and a review of the literature. Chest 1999;115:293-300.
- Thomson DB. Endobronchial streptokinase to dissolve a right mainstem clot. Chest 1986;89:904.
- Homasson JP, Vergnon JM. Cryotherapy to extract obstructing blood clots. J Bronchol Interv Pulmonol 2002;9:158-9.
- Sriratanaviriyakul N, Lam F, Morrissey BM, Stollenwerk N, Schivo M, Yoneda KY. Safety and clinical utility of flexible bronchoscopic cryoextraction in patients with non-neoplasm tracheobronchial obstruction: a retrospective chart Review. J Bronchology Interv Pulmonol 2015;22:288-93.
- Tomic R, Podgaetz E, Andrade RS, Dincer HE. Cryotechnology in diagnosing and treating lung diseases. J Bronchology Interv Pulmonol 2015;22:76-84.
- Maiwand MO. Cryotherapy for advanced carcinoma of the trachea and bronchi. BMJ 1986;293:181-2.
- Hetzel M, Hetzel J, Schumann C, Marx N, Babiak A. Cryorecanalization: a new approach for the immediate management of acute airway obstruction. J Thorac Cardiovasc Surg 2004;127:1427-31.
- Mehta AC, Rafanan AL. Extraction of airway foreign body in adults. J Bronchol 2001;8:123-31.
- Weerdt SD, Noppen M, Remels L, Vanherreweghe R, Meysman M, Vincken W. Successful removal of a massive endobronchial blood clot by means of cryotherapy. J Bronchol Interv Pulmonol 2005;12:23-4.
- Schummer W, Schummer C. Hemorrhagic tracheobronchial obstruction. J Bronchol Interv Pulmonol 2001;8:236.
- Schumann C, Kropf C, Rudiger S, Wibmer T, Stoiber KM, Lepper PM. Removal of an aspirated foreign body with a flexible cryoprobe. Respir Care 2010;55:1097-9.
- Bhardwaj B, Youness BH, Awab HA. Bronchoscopic cryoextraction: a novel approach for the removal of massive endobronchial blood clots causing acute airway obstruction. Southwest J Pulm Crit Care 2013;7:184-9.
- Lee H, Leem CS, Lee JH, Lee CT, Cho YJ. Successful removal of endobronchial blood clots using bronchoscopic cryotherapy at bedside in the intensive care unit. Tuberc Respir Dis 2014;77:193-6.
- Kreider ME, Lipson DA. Bronchoscopy for atelectasis in the ICU: a case report and review of the literature. Chest 2003;124:344-50.
- Rowe BH, Rampton J, Bota GW. Life-threatening luminal obstruction due to mucous plugging in chronic tracheostomies: three case reports and a review of the literature. J Emerg Med 1996;14:565-7.
- Gallon AM. Evaluation of nebulised acetylcysteine and normal saline in the treatment of sputum retention following thoracotomy. Thorax 1996;51:429-32.
- Murgu SD, Colt HG. Complications of silicone stent insertion in patients with 19 expiratory central airway collapse. Ann Thorac Surg 2007;84:1870-7.
- Casal RF. Update in airway stents. Curr Opin Pulm Med 2010;16:321-8.
- Ost DE, Shah AM, Lei X, Godoy MCB, Jimenez CA, Eapen GA, et al. Respiratory infections increase the risk of granulation tissue formation following airway stenting in patients with malignant airway obstruction. Chest 2012;141:1473-81.
- Aktas Z, Gunay E, Hoca NT, Yilmaz A, Demirag F, Gunay S, et al. Endobronchial cryobiopsy or forceps biopsy for lung cancer diagnosis. Ann Thorac Med 2010;5:242-6.
Yazışma Adresi (Address for Correspondence)
Dr. Cengiz ?ZDEMİR
İstanbul Yedikule G?ğ?s Hastalıkları ve
G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi,
İstanbul - T?RKİYE
e-mail: cengizoz78@yahoo.com