RESEARCH ARTICLE
Doi: 10.5578/tt.67434
Tuberk Toraks 2018;66(4):312-316
Endobronşiyal hamartomların endoskopik tedavisinde n?ksleri ?nleyebilir miyiz?
Zafer AKTAŞ1, Aydın YILMAZ1, Ayperi ?ZT?RK1, Mevl?t KARATAŞ1
1 Ankara Atat?rk G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, Girişimsel Pulmonoloji Kliniği, Ankara, T?rkiye
1 Clinic of Interventional Pulmonology, Ankara Ataturk Chest Diseases and Chest Surgery Training and Research Hospital, Ankara, Turkey
?ZET
Endobronşiyal hamartomların endoskopik tedavisinde n?ksleri ?nleyebilir miyiz?
Giriş: Endobronşiyal hamartomların girişimsel bronkoskopik y?ntemlerle tedavisi m?mk?nd?r. Tedavi edici etkinlikleri ile ilgili birka? bildiri olmasına rağmen uygulama protokol? merkezler arasında değişmekte ve y?ksek n?ks oranları problem olmaya devam etmektedir. Bu ?alışmada, girişimsel bronkoskopik y?ntemlerle endobronşiyal hamartomun intraluminal kısmının ?ıkarılmasından sonra bronş duvarındaki lezyon k?k?ne uygulanan kriyoterapinin n?ksleri ?nleyebileceğini g?stermeyi ama?ladık.
Materyal ve Metod: 2012-2016 yılları arasında semptomatik endobronşiyal hamartomu olan ve girişimsel bronkoskopik y?ntemlerle tedavi ettiğimiz ardışık 21 hastanın tedavi sonu?ları ve uzun d?nem takipleri prospektif olarak kayıt edildi. Veriler retrospektif olarak incelendi.
Bulgular: Hastaların 20 (%95.2)'sinde tam rezeksiyon, yalnızca 1 (%4.8)'inde inkomplet rezeksiyon yapıldı. Debulking sonrası t?m lezyonların bronş duvarında izlenen k?k kısımlarına kriyoterapi yapıldı. İnkomplet rezeksiyon yapılan 1 (%4.8) hasta takibinin 20. ayında n?ks etti ve sağ alt lobektomi ile tedavi edildi. Diğer 20 (%95.2) hasta periyodik toraks bilgisayarlı tomografi ve bronkoskopilerle ortalama 36.0 ? 15.0 ay takip edildi. N?ks saptanmadı. İşlemlere bağlı komplikasyon veya ?l?m izlenmedi.
Sonu?: Endobronşiyal hamartomların bronkoskopik y?ntemlerle debulkingi etkili ve g?venli tedavi y?ntemidir. Lezyon k?k?ne yapılan kriyoterapi, y?ksek n?ks oranlarını ?nleyebilir.
Anahtar kelimeler: Endobronşiyal hamartomlar; kriyoterapi; girişimsel bronkoskopi; endobronşiyal tedavi; benign t?m?r
SUMMARY
Can we prevent recurrences in the endoscopic treatment of endobronchial hamartomas?
Introduction: Recently, treatment of endobronchial hamartomas with interventional bronchoscopic methods has become possible. Although there are several reports of therapeutic benefits, the protocol of administration varies between centers and high recurrence rates continue to be a problem. In this study, we aimed to show that cryotherapy applied to the root of the bronchial wall after removal of the intraluminal portion of endobronchial hamartoma with interventional bronchoscopic methods can prevent recurrences.
Materials and Methods: Between 2012-2016, the treatment outcomes and long-term follow-up data of patients with symptomatic endobronchial hamartomas treated by interventional bronchoscopic methods were prospectively recorded. After debulking, cryotherapy was applied to the root of the bronchial wall of all lesions. The data were analyzed retrospectively.
Results: A total of 21 consecutive patients were studied. Twenty (95.2%) of the patients underwent complete resection and only 1 (4.8%) had incomplete resection with various interventional bronchoscopy techniques. One (4.8%) patient who underwent incomplete resection and ineffective cryotherapy relapsed. The other 20 (95.2%) patients were followed up periodically for an average of 36.0 ? 15.0 months. No recurrence was detected. No complications or deaths related to the procedure were observed.
Conclusion: Debulking of endobronchial hamartomas with interventional bronchoscopic methods is effective and safe. Cryotherapy to the root of the lesion may prevent high recurrence rates.
Key words: Endobronchial hamartomas; cryotherapy; interventional bronchoscopy; endobronchial treatment; benign tumor
Geliş Tarihi/Received: 27.10.2018 - Kabul Ediliş Tarihi/Accepted: 15.12.2018
INTRODUCTION
Hamartomas are the most common benign pulmonary tumors. The incidence varies between 0.025% and 0.032% (1). Endobronchial hamartomas constitute 10-20% of all pulmonary hamartomas (2). Pulmonary hamartomas are usually asymptomatic and are diagnosed incidentally. In endobronchial hamartomas, at least one of the symptoms of airway obstruction such as cough, hemoptysis and dyspnea are most commonly seen (80%) (3,4). The results of bronchoscopic removal of symptomatic endobronchial hamartomas and recurrence rates have been the subject of several studies (4-10).
Cryotherapy is an endobronchial therapy based on the cytotoxic effects of extreme cold on tumor tissues. Excessive cold causes intracellular and extracellular ice crystals to form in the affected tissue (11-15). These crystals damage intracellular organelles, especially mitochondria. The most lethal effect is the formation of intracellular ice crystals. This effect results from fast freezing and slow thawing cycles (16). In clinical practice, cryotherapy is used as an endobronchial treatment method capable of destroying tumor cells at a depth of 10 mm with a rigid probe and at a depth of 3 mm with a flexible probe (17-18).
We investigated the treatment and long-term follow-up results of patients who underwent cryotherapy to the site of origin on the airway wall after the luminal part of the symptomatic endobronchial hamartomas was removed by interventional bronchoscopic methods. We aimed to determine the benefit of cryotherapy to conventional endobronchial debulking at the sites of origin of hamartomas.
MATERIALS and METHODS
Twenty-one consecutive patients who were treated with interventional bronchoscopic methods for endobronchial hamartoma between 2012-2016 at our Interventional Pulmonology Clinic were included in the study. Patients with coagulation anomalies or low platelet counts, pregnancy, or who were younger than 18 years of age and those who did not sign the informed consent were excluded from the study. The data were collected prospectively and analyzed retrospectively.
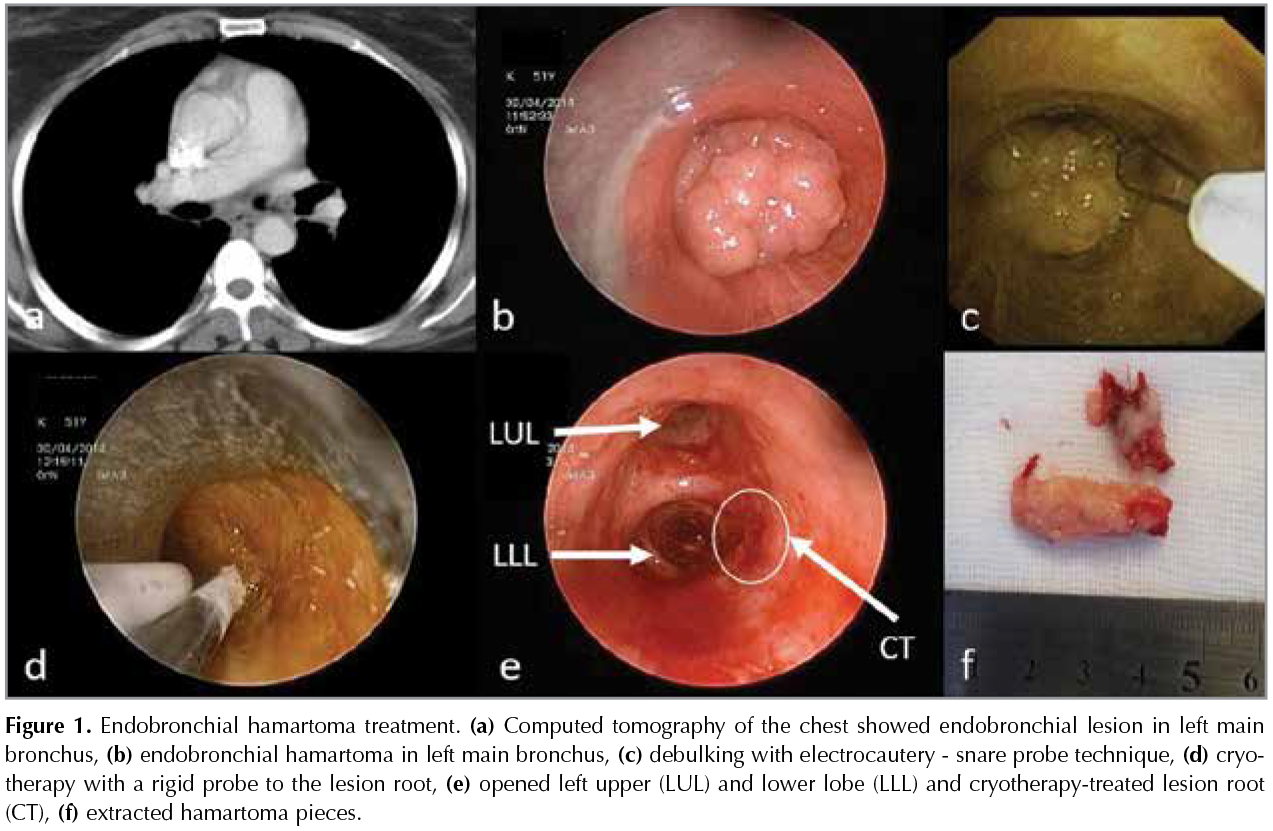
General anesthesia was administered by an intravenous anesthesia technique. Patients were intubated with a rigid bronchoscope (Effer-Dumon, 11 mm diameter, 43 cm length, Efer Endoscopy, Marseille, France). Debulking procedures were performed by mechanical tumor resection (MTR) using the tip of the rigid bronchoscope, rigid pliers or argon plasma coagulation assisted MTR (ERBE ICC 200/APC 300 electrosurgical unit, rigid APC probe, 50 cm length, 2.3 mm diameter; ERBE, Medizintechnik, GmbH, T?bingen, Germany) or cryorecanalization (ERBOKRYO? CA unit, ERBE flexible cryoprobe 2.4 mm diameter, 90 cm length or ERBE rigid cryoprobe 3 mm diameter, 53 cm length; ERBE, Medizintechnik, GmbH, T?bingen, Germany) or electrocautery-snare probe (Erbotom ICC 200 electrosurgical unit ERBE, Medizintechnik GmbH, T?bingen, Germany and Electrosurgical snare probe SD-7C-1, loop diameter 23 mm, length 1050 mm, Olympus EndoTherapy, Tokyo, Japan). An innovation of our study was that cryotherapy (Using the same equipment as cryorecanalization) was performed in the regions where the lesions originated after debulking (Figure 1).
Descriptive statistics were expressed as the mean ? standard deviation for intermittent and continuous numerical variables, and categorical variables were expressed as number of cases and "(%)".
This study has been approved by the local ethics committee. Informed consent was obtained from all patients.
RESULTS
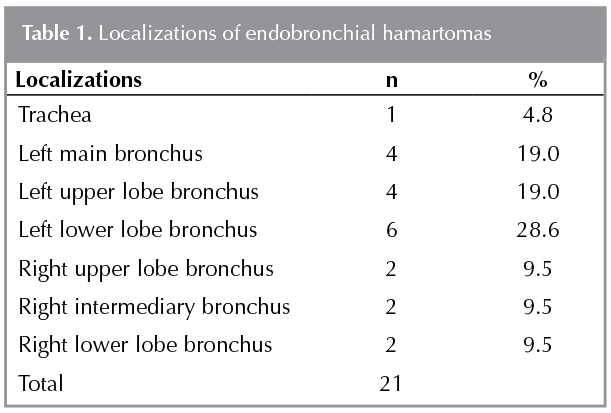
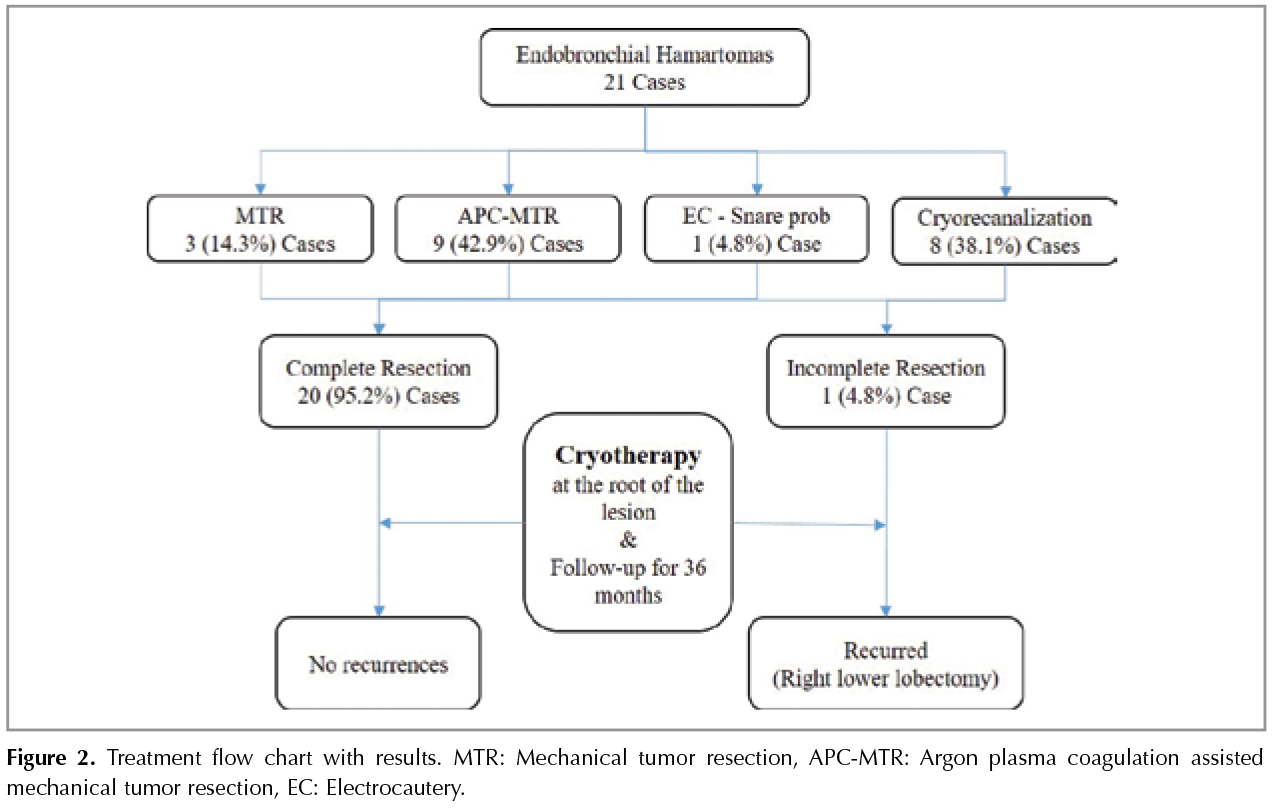
The mean age of the study cases was 58.7 ? 10.7 years. Most of the patients were male (18 cases). The locations of the lesions were the trachea, main bronchi, and lobe bronchi (1,4,16) (Table 1). APC-assisted MTR (42.9%) was the most common debulking method. Twenty (95.2%) of the patients had a complete resection and only 1 (4.8%) had an incomplete resection. After debulking, cryotherapy was applied to the root portion of the bronchial wall of all lesions. One (4.8%) patient who underwent incomplete resection and ineffective cryotherapy (due to lesion root not reached with cryprobe) relapsed at the 20th month follow-up and was treated with right lower lobectomy. The other 20 (95.2%) patients were followed up periodically by chest computerized tomography and bronchoscopy for a mean of 36.0 ? 15.0 months. No recurrences were detected (Figure 2). No complications or deaths related to the procedure were observed.
DISCUSSION
Debulking of endobronchial hamartomas with bronchoscopic methods is indicated as the first-line treatment (4-10). In 5 studies, pooled recurrence was observed in 10 (14.5%) of 69 patients who underwent endobronchial debulking by various methods (Table 2). Recurrent bronchoscopic procedures are recommended for these high recurrence rates (10). For intraluminal hamartomas, there is insufficient data in the literature explaining the association of tumor recurrence with complete or partial resection during endobronchial treatment. Miller and Jhun's studies did not reveal any recurrences in 4 cases with partial resection (Table 2). However, in Miller's study, the duration of follow-up was not specified, and in Jhun's study the follow-up duration was only 12.2 months. The only case of incomplete resection in our study recurred at 20 months post-treatment. The likelihood of recurrent tumor growth from tumor tissue remaining in an incomplete resection is reasonable. We think that these 4 cases should be followed longer for recurrence.
In Kim's study, at least 1 case of complete resection (mean follow-up of 26 months) recurred (Table 2). This result suggests that residual tumor cells from which endobronchial hamartoma originate may remain in the bronchial wall even if a complete resection is performed. In our study, there were no recurrences in 20 patients who underwent complete resection and cryotherapy at the root of the lesion and were followed for 36 months. These data suggest that cryotherapy at the root of the lesion can prevent recurrences by destroying residual tumor cells in the bronchial wall. The local recurrence protective effect of endobronchial cryotherapy has also been demonstrated for the treatment of typical carcinoid tumors and early stage squamous cell lung cancers, which are expected to have a more aggressive biological behavior (19,20).
The strength of our study is that our follow-up period is longer than similar studies. The weakness of our study is that it is retrospective as in similar studies, and randomization is not possible because of the rarity of these tumors.
CONCLUSION
Debulking of endobronchial hamartomas with interventional bronchoscopic methods is effective and safe. After complete resection, cryotherapy to the root of the lesion may prevent high recurrence rates.
REFERENCES
- Murray J, Kielkowski D, Leiman G. The prevalence and age distribution of peripheral pulmonary hamartoma in adult males: an autopsy-based study. S Afr Med J 1991;79:247-9.
- David HB, Samuel PH. Pulmonary pathology; 2nd ed. Springer, New York 1994.
- Gjevre JA, Myers JL, Prakash UB. Pulmonary hamartomas. Mayo Clin Proc 1996:71:14-20.
- Cosio BG, Villena V, Echave-Sustaeta J, de Miquel E, Alfaro J, Hernandez L, et al. Endobronchial hamartoma. Chest 2002;122:202-5.
- Kim SA, Um SW, Song JU, Jeon K, Koh WJ, Suh GY, et al. Bronchoscopic features and bronchoscopic intervention for endobronchial hamartoma. Respirology 2010;15:150-4.
- Jhun BW, Lee K, Jeon K, Um SW, Suh GY, Chung MP, et al. The clinical, radiological and bronchoscopic findings and outcomes in patients with benign tracheobronchial tumors. Yonsei Med J 2014;55:84-91.
- Wang J, Huang M, Zha W, Zhou L, Qi X, Wang H. Flexible bronchoscopic intervention for endobronchial hamartoma. Chinese J Tuberc Respir Dis 2013;36:963-7.
- Miller SM, Bellinger CR, Chatterjee A. Argon plasma coagulation and electrosurgery. J Broncho Interv Pulmonol 2013;20:38-40.
- Shah H, Garbe L, Nussbaum E, Dumon JF, Chiodera PL, Cavaliere S. Benign tumors of the tracheobronchial tree. Endoscopic characteristics and role of laser resection. Chest 1995;107:1744-51.
- Abdel Hady SM, Elbastawisy SE, Hassaballa AS, Elsayed HH. Is surgical resection superior to bronchoscopic resection in patients with symptomatic endobronchial hamartoma? Interact Cardiovasc Thorac Surg 2017;24:778-82.
- Vergnon JM. How I do it: bronchoscopic cryotherapy. J Bronchol 1995;2:323-7.
- Mazur P. The freezing of biological systems. Science 1970;168:939-49.
- Neel HG, Farrell KH, Payne WS. Cryosurgery of respiratory structures 1-cryonecrosis of trachea and bronchus. Laryngoscope 1973;83:1062-71.
- Vergnon JM. Cryothe?rapie endobronchique: techniques et indications. [Endobronchial cryotherapy: techniques and indications]. Rev Mal Respir 1999;16:619-23.
- Homasson JP. Bronchoscopic cryotherapy. Journal Bronchol 1995;2:145-53.
- Vergnon JM, Guichenez Ph, Fournel P, Emonot A. Efficiency of cryotherapy in bronchial tumors. Am Rev Respir Dis 1990;141:A402.
- Vergnon JM, Huber RM, Moghissi K. Place of cryotherapy, brachytherapy and photodynamic therapy in therapeutic bronchoscopy of lung cancers. Eur Respir J 2006;28:200-18.
- Homasson JP, Renault P, Angebault M, Bonniot JP, Bell NJ. Bronchoscopic cryotherapy for airway strictures caused by tumors. Chest 1986;90:159-64.
- Bertoletti L, Elleuch R, Kaczmarek D, Jean-Fran?ois R, Vergnon JM. Bronchoscopic cryotherapy treatment of isolated endoluminal typical carcinoid tumor. Chest 2006;130:1405-11.
- Deygas N, Froudarakis M, Ozenne G, Vergnon JM. Cryotherapy in early superficial bronchogenic carcinoma. Chest 2001;120:26-31.
Yazışma Adresi (Address for Correspondence)
Dr. Zafer AKTAŞ
Ankara Atat?rk G?ğ?s Hastalıkları ve
G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi,
Girişimsel Pulmonoloji Kliniği,
ANKARA - T?RKİYE
e-mail: zaferaktas88@gmail.com