CASE REPORT
Doi: 10.5578/tt.66180
Tuberk Toraks 2018;66(1):68-71

Gebelikte yabancı cisim aspirasyonu: Başarıyla ?ıkarılan leblebi tanesi
Barış Mustafa POYRAZ1, Ayşeg?l ALKILI?2, Murat ?ZKAN3, Servet Se?kin Tun? KASAP3, Numan NUMANOĞLU1, G?khan TULUNAY4
1 TOBB ET? Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, Ankara, T?rkiye
1 Department of Chest Diseases, Faculty of Medicine, TOBB ETU, Ankara, Turkey
2 TOBB ET? Hastanesi, Kadın Hastalıkları ve Doğum B?l?m?, Ankara, T?rkiye
2 Department of Obstetrics and Gynecology, TOBB ETU Hospital, Ankara, Turkey
3 Ankara ?niversitesi Tıp Fak?ltesi, G?ğ?s Cerrahisi Anabilim Dalı, Ankara, T?rkiye
3 Department of Chest Surgery, Faculty of Medicine, Ankara University, Ankara, Turkey
4 TOBB ET? Tıp Fak?ltesi, Kadın Hastalıkları ve Doğum Anabilim Dalı, Ankara, T?rkiye
4 Department of Obstetrics and Gynecology, Faculty of Medicine, TOBB ETU, Ankara, Turkey
?ZET
Gebelikte yabancı cisim aspirasyonu: Başarıyla ?ıkarılan leblebi tanesi
Yabancı cisim aspirasyonu, t?m yaş grupları i?in ciddi bir sağlık sorunudur ve ?zellikle gebelerde hem anne adayı hem de fet?s i?in ciddi komplikasyonlara yol a?abilir. Burada g?lerken leblebi tanesi aspire eden 36 yaşında 22 haftalık gebe bir olgumuzu sunuyoruz. ?ks?r?k ve nefes darlığı şikayetiyle başvuran hastada yapılan bronkoskopi sonucunda sağ alt lob girişini tıkayan leblebi tanesi başarılı bir şekilde ?ıkartıldı, alt lob a?ıklığı sağlandı ve işlem sonrasında hastamızda ve fet?ste komplikasyon izlenmedi. Yabancı cisim aspirasyonunda bronkoskopi, tecr?beli bir ekip tarafından uygulandığı zaman, gebelerde de g?receli olarak g?venli bir işlemdir.
Anahtar kelimeler: Yabancı cisim aspirasyonu, gebelik
SUMMARY
Foreign body aspiration in a pregnant woman: successfully removed roasted chickpea
Foreign body aspiration is a serious health problem in all age groups, and in pregnancy it may cause serious complications for the fetus as well as the pregnant woman. Here we present our case of a 36 years old 22 weeks pregnant woman, accidentally aspirating roasted chickpea upon laughing. She had the complaints of coughing and shortness of breath on admission, bronchoscopy was performed, and the roasted chickpea blocking the entrance of right lower lobe bronchus was removed without any complications. For foreign body aspiration in pregnancy, bronchoscopy is a rather safer procedure when performed by an experienced team.
Key words: Foreign body aspiration, pregnancy
Geliş Tarihi/Received: 28.11.2017 - Kabul Ediliş Tarihi/Accepted: 27.12.2017
Introduction
Foreign body aspiration (FBA)? is a serious health problem, concerning the potentially life threatening consequences. It necessitates prompt recognition and treatment as soon as possible (1).? Although, it is mostly seen in children population with peak frequency in 1-2 years age group, accidental aspiration of various materials (nuts, food remnants, small toys, etc.) may occur in all age groups (2).? There is little published data on FBA in pregnant patients. In pregnant population, hypoxemia as a complication of FBA may contribute to low birth weight, spontaneous abortion and placenta previa (3). Thus, rapid diagnosis and treatment is crucial for not only the mother but the fetus. Here we present our case of? a 36 years old 22 weeks pregnant woman, accidentally aspirating roasted chickpea upon laughing.
Case Report?
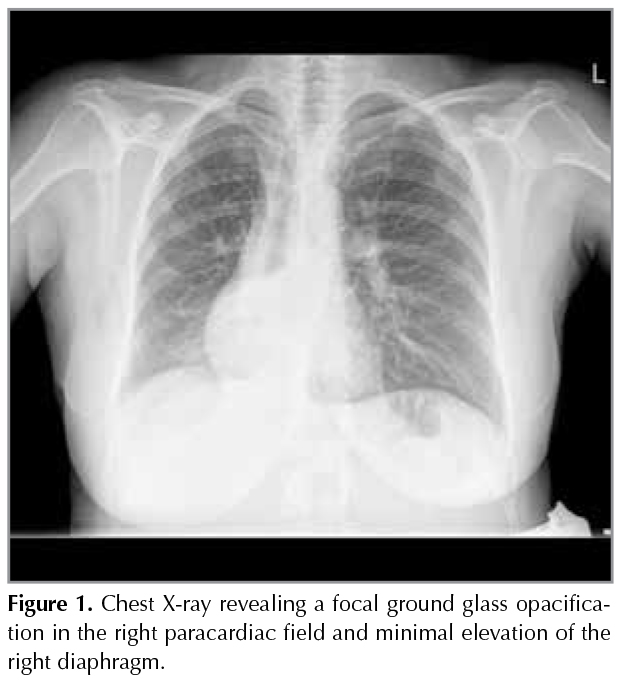
A 36-year-old G2P1 at 22 weeks gestation female was admitted to our hospital with complaints of cough, and shortness of breath? for 4 days. She had no fever or sputum, but she had a slight chest pain on the right side. She mentioned that , these complaints started after a laughter episode while she was eating roasted chickpea. There was not any significant point in her history. Physical examination revealed body weight of 82.6 kg, pulse rate of 80 beats/min, respiratory rate of 15/min, blood pressure of 110/70 mmHg, body heat of 36?C and oxygen saturation was 96% by pulse oxymetry.? Coarse crackles at the end of inspirium? were heard in auscultation of the right middle zone. Blood tests showed a white blood cell count of 7040 /L, hemoglobin 11.4 g/dL, platelets 156.000/L, d-dimer to 0.37 mg/L and CRP level of 79.1 mg/L. In the light of these findings, a chest X-ray was offered to the patient. Hesitation was understandable as she was a pregnant woman, but then, after the permisson from the following obstetrician and with informed consent, a PA chest X-ray was obtained while the womb is covered with radioprotective plate.? The X-ray revealed a focal ground glass opacification in the right paracardiac field and minimal elevation of the right diaphragm (Figure 1) .
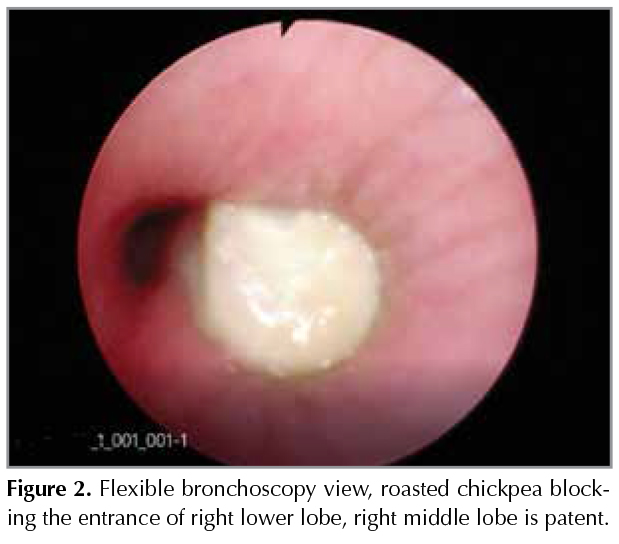
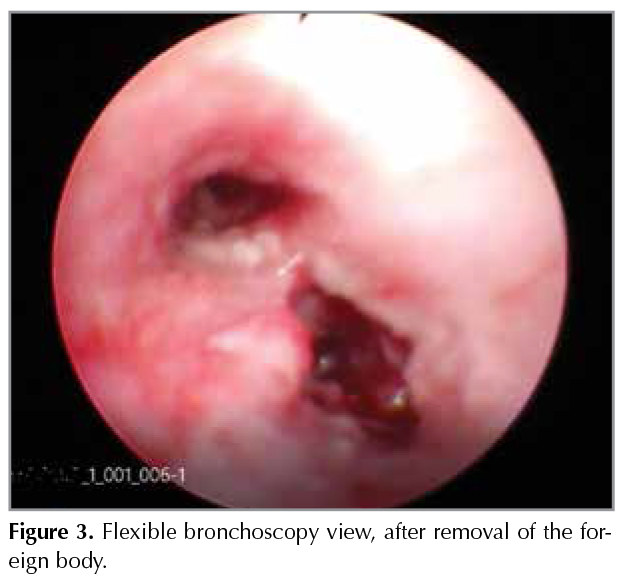
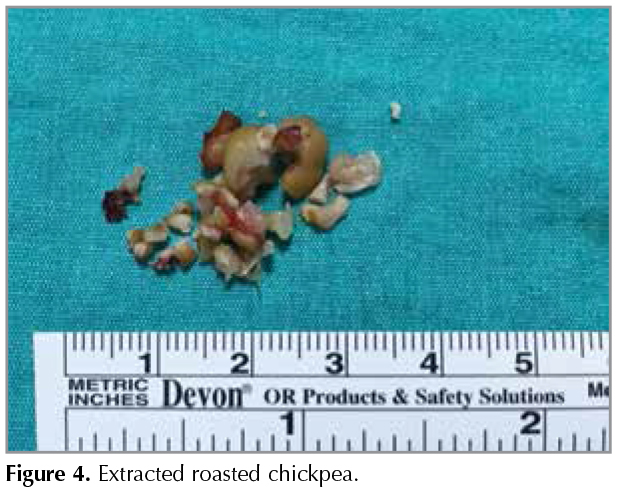
The results increased the suspicion of FBA, and the patient was offered to have a bronchoscopy. She was transferred to Ankara University Chest Surgery Department in case of need for rigid bronchoscopy. Under general anesthesia, flexible fiberoptic bronchoscopy was performed, and the roasted chickpea was seen in right main bronchus, blocking the entrance of the right lower lobe bronchus. The surrounding mucosa was hyperemic and the right lower lobe atelectasia was obvious (Figure 2) . The bronchoscopy team was able to retrieve the foreign body and clear the whole area. After the removal of the roasted chickpea, all segments were open distal to the obstruction site (Figure 3) . The swollen roasted chickpea and its pieces were completely removed ( Figure 4). The patient were discharged the day after with no complications and she is having a healthy pregnancy follow-up after then.
Discussion
Foreign body aspiration is a clinical problem that the physician needs to be alert about. The delay time till the diagnosis is critical for the patients. The first bronchoscopy was performed by Gustav Killian in 1897 after a piece of pork bone aspiration and the bone was successfully removed (4).? Several materials like nuts, food remnants, seeds, toy parts and even tracheostomy canulas were reported since then (5,6). In adults, there is predominancy of the? obstruction of right bronchial system which can be explained by a more direct pathway of the right main bronchus and flexible bronchoscopy has a high success rate and should be the preferred initial procedure for diagnosis and removal of the foreign body (1,7).
As in our case, pregnancy is a special condition for FBA and bronchoscopy is considered as an emergent condition for marked lung collapse caused by an obstructing foreign body. It is recommended that, during pregnancy, bronchoscopy should be performed in a well-equipped hospital with ready access to anesthesia, obstetrics and neonatology services( 8). Maybe the biggest problem for pregnant women with FBA is the decision making and the timing of the procedure. There is no clear study results? for the utility and safety of bronchoscopy and other diagnostic procedures during pregnancy except some rare case reports, so we have to decide if the indication could be postponed till post partum period (8,9).
We strongly suspected of right lower lob atelectasia with physical examination and chest X-ray? findings and our patient was only 22 weeks pregnant, with expected delivery date is at least 17 weeks ahead. The delay could result in drastic situations and at least observation was necessary by bronchoscopy. And the clear history given by the patient about the starting time of the complaints was so helpful. As we know, organic materials cause a more severe mucosal inflammation and beans, seeds has the potential of absorbing water thus subsequent swelling could lead to more severe obstruction (1). The resulting bronchoscopy showed that we were right about our concerns, the roasted chickpea totally obstruction lower lobe was removed successfully and possible future complications for fetus and mother were prevented after this intervention.
In conclusion, in case of FBA in pregnancy, physician? must not only think about the mother but also the fetus, which may be effected by subsequent complications like hypoxia and infections. Prompt decision making and intervention is necessary and flexible bronchoscopy is a rather safer procedure.
REFERENCES
- Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: clinical utility offlexible bronchoscopy. Postgrad Med J 2002;78(921):399-403.
- Salih AM, Alfaki M, Alam-Elhuda DM. Airway foreign bodies: a critical review for a common pediatric emergency. World J Emerg Med 2016;7(1):5-12.
- Atkinson AL, Canterino J. Foreign body aspiration in pregnancy. Case Rep Obstet Gynecol 2012;2012:890106.
- Prowse SJ, Makura Z. Gustav Killian: beyond his dehiscence. J Laryngol Otol 2012;126(11):1164-8.
- Blanco Ramos M, Botana-Rial M, Garc?a-Font?n E, Fern?ndez-Villar A, Gallas Torreira M. Update in the extraction of airway foreign bodies in adults. J Thorac Dis 2016;8(11):3452-56.
- Sent?rk E, Sen S. An unusual case of foreign body aspiration and review of the literature. Tuberk Toraks 2011;59(2):173-7.
- Sehgal IS, Dhooria S, Ram B, Singh N, Aggarwal AN, Gupta D, Behera D, Agarwal R. Foreign body inhalation in the adult population: experience of 25,998 bronchoscopies and systematic review of the literature. Respir Care 2015; 60(10):1438-48.
- Bahhady IJ, Ernst A. Risks of and recommendations for flexible bronchoscopy in pregnancy: a review. Chest 2004;126(6):1974-81.
- Patil MH, Siddiqi A, Jeffrey Mador M. Successful bronchoscopy in a pregnant patient with plastic bronchitis. Respir Med Case Rep 2016;18:8-9.
Yazışma Adresi (Address for Correspondence)
Dr. Barış Mustafa POYRAZ
TOBB ET? Hastanesi
Yaşam Cad. No: 5 S?ğ?t?z?,
ANKARA - TURKEY
e-mail: bmpoyraz@yahoo.com