RESEARCH ARTICLE
Doi: 10.5578/tt.66752
Tuberk Toraks 2018;66(1):37-42

Kaynak?ıların akciğerlerine daha dikkatli bakalım
İpek ?ZMEN1, Elif YILDIRIM1, Reyhan YILDIZ1, Hamza OGUN2, Emine AKSOY1, T?lay T?R?N1, Peri ARBAK3, Haluk ?ALIŞIR4
1 Sağlık Bilimleri ?niversitesi S?reyyapaşa G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği, İstanbul, T?rkiye
1 Clinic of Chest Diseases, Health Sciences University Sureyyapasa Chest Disease and Thoracic Surgery Training and Research Hospital, Istanbul, Turkey
2 Tokat Turhal Devlet Hastanesi, G?ğ?s Hastalıkları Kliniği, Tokat, T?rkiye
2 Clinic of Chest Diseases, Tokat Turhal State Hospital, Tokat, Turkey
3 D?zce ?niversitesi Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, D?zce, T?rkiye
3 Department of Chest Disesases, Faculty of Medicine, University of Duzce, Duzce, Turkey
4 Acıbadem ?niversitesi Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, İstanbul, T?rkiye
4 Department of Chest Disesases, Faculty of Medicine, University of Acibadem, Istanbul, Turkey
?ZET
Kaynak?ıların akciğerlerine daha dikkatli bakalım
Giriş: Kaynak işlemi, ?rettiği gaz ve partik?ller ile solunum sistemi ?zerinde etkiler yaratır ve uzun d?nem maruziyet ile "kaynak?ı akciğeri" oluşabilir. Bu ?alışmanın amacı, kaynak?ıların radyolojik bulgularını tanımlamak ve bu konuda farkındalık yaratmaktır.
Materyal ve Metod: Ocak 2010-Ocak 2017 tarihleri arasında solunumsal yakınmalar ile polikliniğe başvuran kaynak?ıların klinik, radyolojik ?zellikleri retrospektif olarak incelendi.
Bulgular: Ortalama yaşları 37 ? 8 toplam 16 erkek kaynak?ının ortalama kaynak?ılık s?releri 12 ? 7 yıldı. En sık rastlanan semptomlar ?ks?r?k (%87), balgam ?ıkarma (%63) ve dispne (%63) idi. On ?? kaynak?ı tersanede, ??? inşaat ve diğer işlerde ?alışıyordu. ?? hastada (%19) fizik muayene ronk?s saptandı, bu hastalarda spirometride FEV1/FVC değerleri %70'in altına saptandı. Y?ksek ??z?n?rl?kl? toraks bilgisayarlı tomografide (YRBT), akciğer filminde net olarak g?r?lemeyen, silik sınırlı sentrilob?ler mikronod?ller g?r?ld?. Yedi hastaya bronkoskopi yapıldı. Demir pozitif pigment gran?lleri ve ferrigin?z cisimler 3 hastanın bronkoalveolar lavaj sıvısında saptandı.
Sonu?: Kaynak?ıların akciğer grafileri daha yakından incelenmeyi hak etmektedir. Akciğer grafisinde, k???k sınırları net olmayan milimetrik nod?llerden, buzlu cam alanlarına kadar değişen radyolojik bulgular olabilir. Kaynak?ıların akciğer filmlerine daha dikkatli bakılmalı ve ş?pheli olgularda YRBT ile değerlendirme yapılmalıdır. Radyolojik bulgular i?in oluşacak farkındalık ile bu hastalarda girişimsel işlemler azaltacaktır. Buradan da yola ?ıkarak mesleki ?yk? hekimlerin g?nl?k pratiğine dahil edilmelidir.
Anahtar kelimeler: Kaynak; Siderozis; Radyoloji; Pn?mokonyoz; Mesleki maruziyet
SUMMARY
Look closer to welders' lung
Introduction: Welding produces miscellaneous gases and particles that has various impact on respiratory system and long term exposure may result "welders'lung". The aim of this study is to describe the radiological findings of welders' and make an awereness for welders radilogical findings.
Materials and Methods: The clinical and radiological findings of welders' who had hospital applications with respiratory symptoms between January 2010-January 2017 were evaluated retrospectively.
Results: A total of 16 male welders with mean age 37 ? 8 years had the mean duration of welding occupation 12 ? 7 years. The most common symptoms were coughing (87%), sputum production (63%) and dyspnoea (63%).Thirteen welders were working in shipyards and 3 in construction business and other workplaces. Three (19%) patients had rhonchi on physical examination and these patients had decreased FEV1/FVC values below 70% on spirometry. Poorly-defined centrilobular micronodules that were not clearly visible on chest radiographs observed on thorax high resolution computed tomography. Bronchoscopy was performed to 7 patients. Iron-positive pigment granules and ferruginous bodies were revealed in 3 patients' bronchoalveolar lavage.
Conclusion: Welders' chest X-ray deserve a closer look. In pulmonary radiology, there may be radiographical findings ranging from small ill defined nodules to groundglass opacites. Physcians should look more careful to welders' chest X-ray and incase of suspicious findings best can be detected on high HRCT. An awareness for the radiological findings will also reduce interventional procedures in these patients hereby, occupational history must be included in daily practice of physicians.
Key words: Welding; Siderosis; Radiology; Pneumoconiosis; Occupational exposure;
Geliş Tarihi/Received: 23.01.2018 - Kabul Ediliş Tarihi/Accepted: 06.04.2018
INTRODUCTION
Welding is a method of joining metals and similar alloys together, consequently it is widely used in industry. Welding produces miscellaneous gases and particles that has various impact on respiratory system. Long-term exposure to welding fumes may result "welders'lung" (1,2).
Welders' lung is a result of complex effects of welding fumes which together affect the airways and parenchyma together, et all levels of the respiratory tract (2,3). Siderosis develops by deposition of iron oxide in alveolar macrophages and interstitium which result in prolonged exposure to welding fumes (2,4). Respiratory complaints such as chronic cough, dyspnoea, secretions increase in welders (3).
The most common types of pneumoconiosis are silicosis, coal worker pneumoconiosis, and asbestosis whereas, berylliosis, siderosis, stannosis, and baritosis are more rare that are also known as nonfibrotic forms of pneumoconiosis. Siderosis involves poorly defined nodules on chest X-ray, and centrilobular nodules which have blurred borders or ground-glass opacities on computed tomography (5,6).
In daily life practice occupational exposure is occationaly ignored in these poorly defined nodules.
The aim of the study is to describe the radiological findings of welders' that are not prominent on chest X-ray and make an awereness for welders radilogical findings.
MATERIALS and METHODS
This is a retrospective study performed in a tertiary chest disease hospital between January 2010- January 2017. The clinical and radiological findings of welders' who had hospital applications with respiratory symptoms were evaluated.
The study was approved by the local Ethics Committee. Ethical approval was provided in accordance with the Declaration of Helsinki. The informed consent was not obtained due to the retrospective nature of the study.
Patients symptoms, exposure time, smoking status, radiological findings, spirometry were recorded.
High resolution computed tomography (HRCT) was performed during inspiration with 1 mm collimation without intravenous contrast medium.
Spirometry was performed with (ZAN 300)
Bronchoalveolar lavage (BAL) was performed during bronchoscopy with 120-200 cc saline. Cell count; neutrophils, alveolar macrophages, eosinophilia, lymphocytosis, CD4/CD8 ratio (he ratio of T helper cells to cytotoxic T cells), presence of ferriginous body in BAL were recorded.
Statistical Analysis
The SPSS portable 20.0 package program (IBM Corporation, Armonk, NY, USA) was used for analysis. The mean ? standard deviation was used for parametric continuous variables. Count and percentage were used when applicable.
RESULTS
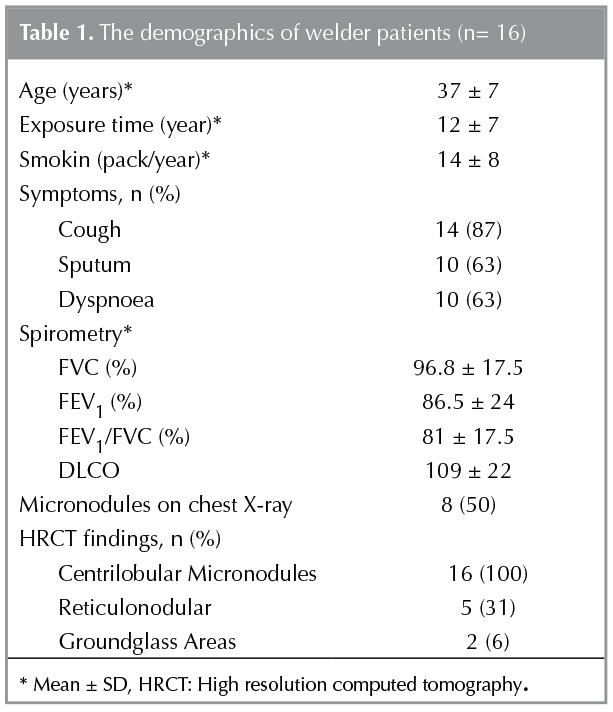
A total of 16 male welders were included in the study. The mean age was 37 ? 8 years and the mean duration of welding occupation was 12 ? 7 years. Twelve (75%) patients were smokers. The mean smoking pack year was 14 ? 8. The most common symptoms were coughing (87%), sputum production (63%) and dyspnoea (63%). Table 1 shows the patients demographics.
The distribution of patients according to their work is; 13 welders were working in shipyards and 3 in construction business and other workplaces. Patients had used manual metal arc welding and gas metal arc welding.
Three (29%) patients had rhonchi on physical examination and these patients had decreased FEV1/FVC values below 70% on pulmonary function tests. The rest of the patients had pulmonary function tests within the normal limits.
According to the patients' own expressions they did not regularly use masks during welding. They were working in doors, even in small spaces and sometimes outside.
Radiological Findings
There were lesions compatible with pneumoconiosis (p or q) in the chest X-ray of 8 (50%) welders.
HRCT was present in all of the patients. Poorly-defined centrilobular micronodules that were not clearly visible on chest radiographs observed on thorax HRCT. Sixteen patients had centrilobular micronodules, five patients also had retikulonoduler pattern and 2 had groundglass areas. Figure 1 shows the poorly-defined centrilobular micronodules and ground glass areas on chest X-ray and HCRT of welders.
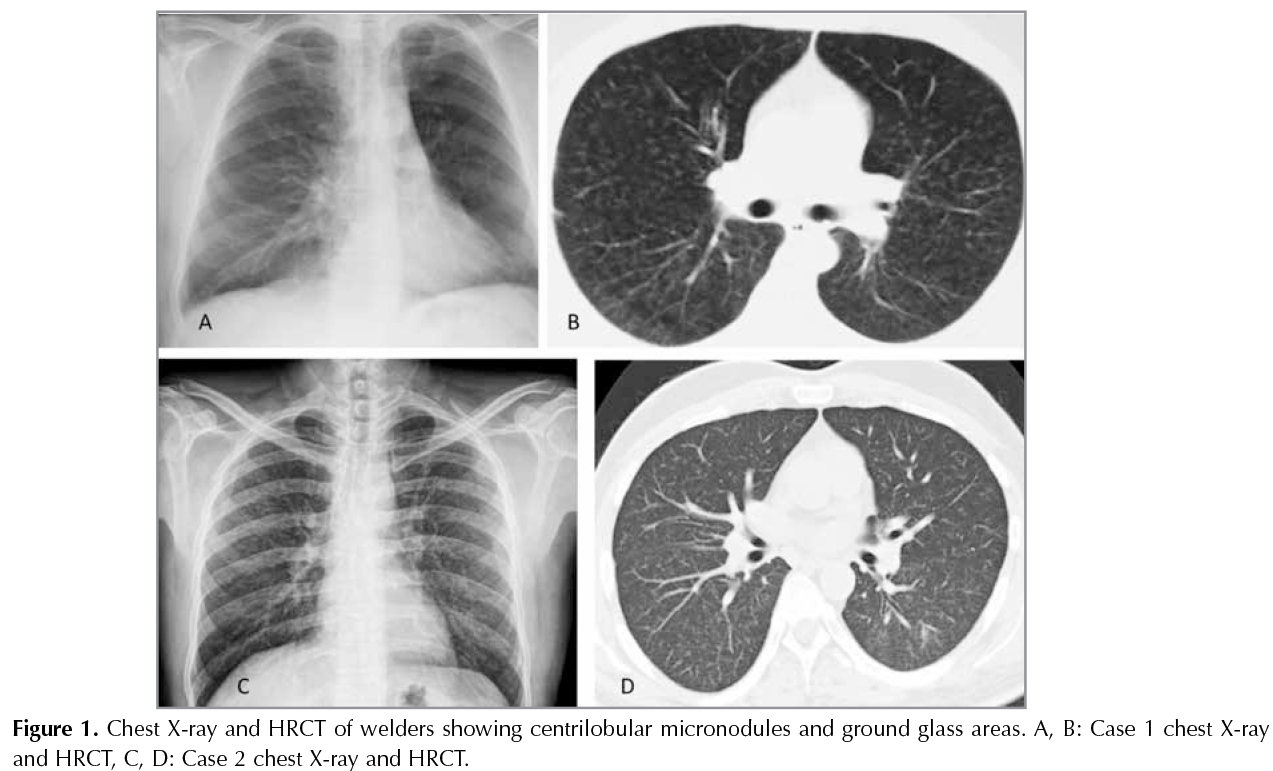
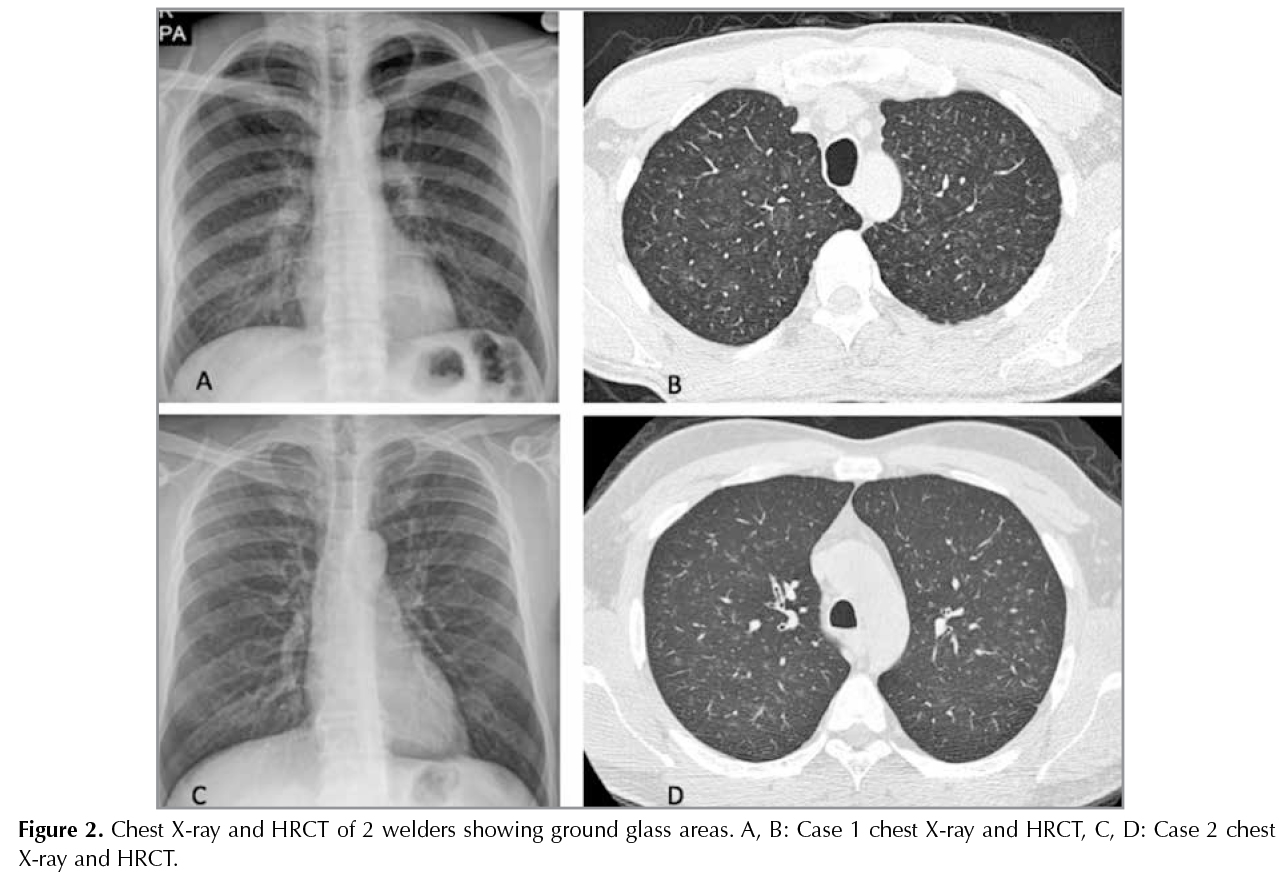
Figure 2 demonstrates chest X-ray and HRCT findings of 2 welders showing ground glass areas.
Bronchoscopic Findings
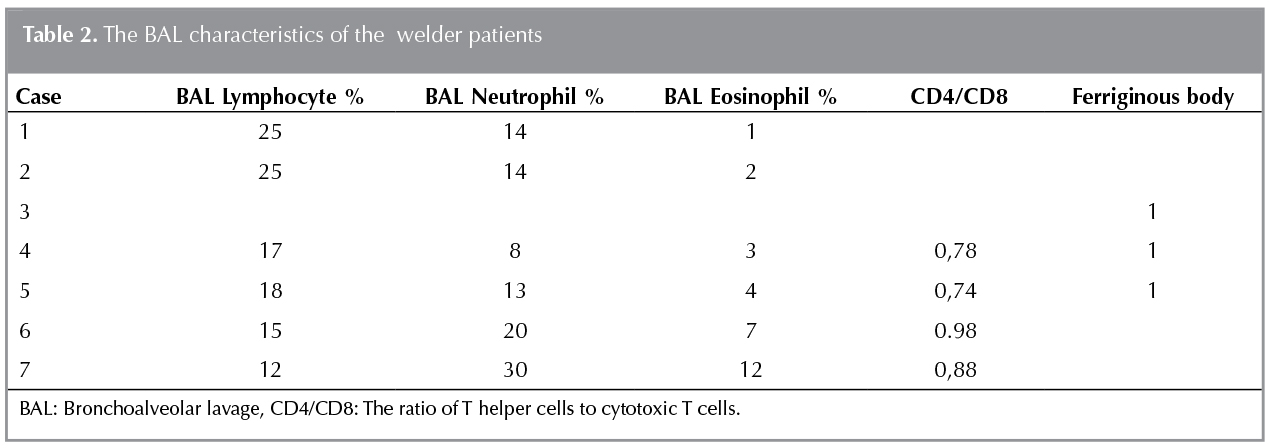
Fiberoptic bronchoscopy was performed to 7 (44%) patients. BAL was evaluated in 6 patients; 5 had mixed alveolitis and one had lymphocytic alveolitis. Iron-positive pigment granules and ferruginous bodies were revealed in 3 patients' BAL. There was no endobronchial abnormalities were observed in bronchoscopy. Table 2 shows the BAL chacteristics of the patients.
DISCUSSION
Welders' chest X-ray deserve a closer look. Welders may have less noticeable radiological findings than other pneumoconiosis (4,5). In pulmonary radiology, there may be radiographical findings ranging from small indistinct millimetric nodules to groundglass opacites (5,6).
Welding fumes can create metal fume, siderosis and chemical pneumonitis in the respiratory system (4,7). In formation of the welders' lungs, the content of the source of smoke, the working environment (closed area, ventilation status, other exposures in the workplace), personal factors (use of protective materials, smoking) play important role (7,8). In this study the most of the welders were working in shipyard, so they were also exposed to processes such as paint, asbestos and scraper.
The main component of welding dust is iron?oxide that causes "welders' siderosis". Welders' lung is a result of mixed inhalant exposures that effect airways and parenchyma together. Long-term exposure may result welders' lung (benign pneumoconiosis/siderosis) (7-9). Siderozis has widespread bilateral poorly defined centrilobular nodules and branched small linear opacities but not fibrosis. Fibrosis is expected if silica is also present with iron exposure or as a result of high exposure to welding fumes or gases (10-12).
Siderosis (silver polisher's lung) is a non-fibrogenic form of pneumoconiosis as a result of exposure of iron particles which is also called as "benign pneumoconiosis". Iron and steel rolling mills, steel grinding, electric arc welding, silver polishing, mining and crushing iron ores can cause this kind of pneumoconiosis (5,6,13,14).
Welders' lung may have small millimetric nodules, groundglass areas, and late-onset radiological findings such as fibrosis and honeycombing (8,9). Pulmonary lesions often seem to be confused with hypersensitivity pneumonia and other interstitial lung diseases. If occupational history is ignored, advanced interventional procedures may be required for diffrential diagnosis. Therefore we emphasize the importance of occupational history one again as early recognition radiological features will reduce invasive interventional procedures in these patients. Tutkun et al. mentioned that HRCT rather than CXR to evaluate parenchymal changes much better in early diagnosis of welders (14). In the present study bronchoscopy was performed in 7 patients. Bronchoscopies and BAL (no transbronchial biopsies performed) had been made to exclude other interstitial lung diseases in this period when our awareness was still developing.
Moa L et al. followed the welders with welders' pneumoconiosis by time and reported that small round opacities get, improved after a time (2-10 years), supporting the diagnosis of siderosis (7). In an animal study of Sung et al. they reported that the pulmonary fibrozis due to welding fumes would be preventable when the exposure is moderate (4).
Temel et al. reported occupational asthma (22%) among welders working in a by cycle factory (15). Tun? et al. reported chronic bronchitis (21.9%) among welders working in sugar factory (11). This can be explained by the contents of the electrodes used during the welding process, the composition of the welded surfaces, their dyes and the exposure to welding gases.In the present study coughing, sputum and dyspnoea were present (63-87%) of the patients. One issue that is discussed in welders is that there are more symptoms such as coughing and sputum in smoker welders. Emphysema may develop due to cigarette smoke or welding fumes, but differential diagnosis is not easy (11-13). In this study 12 (75%) patients were smokers with mean smoking pack year 14 ? 8. In our study we observed mainly reserved FEV1, FEV1/FVC, DLCO, beside that 19% of the patients had rhonchi on physical examination and decreased FEV1/FVC values below 70%.
Welding also creates a risk for lung cancer (16-18). Ambroise et al. reported in a meta-analysis that 26% lung cancer risk for welders (17). At this point it should also be noted that exposure to other carcinogenic agents such as smoking and asbestos.
One of the limitations of our study is that this is a retrospective study, in addition, the study covered welders applied to outpatient clinics not in a certain workplace of welders. Furthermore, the follow up of the patients are missing, there is no control group. On the other hand, a strength of our study is that it was conducted to make an awereness to welders lung and decrease the invasive procedures for these patients.
In conclusion radiological findings on chest X-ray is not rich in welders' lung, chest physcians should look more careful to welders' chest X-ray incase of suspicious findings even at best can be detected on HRCT. Good awareness for the radiological features will reduce interventional procedures in these patients. Chest X-rays of welders should be evaluated carefully for welders that may not be rich in radiological findings, therefore suspicious cases can be evaluated well in HRCT. Considering the importance of occupational exposure, history must be included in daily practice of chest physicians.
REFERENCES
- Kahraman F, Sever K, Karadeniz S. Kaynaklı imalatta insan sağlığı. mmo.org.tr.
- Mann BT, Lecutier ER. Arc-welders' lung. Br Med J 1957 19;2(5050):921-922.
- Kalliom?ki PL, Sutinen S, Kelh? V, Lakomaa E, Sortti V, Sutinen S. Amount and distribution of fume contaminants in the lungs of an arc welder post mortem. Br J Ind Med 1979;36(3):224-30.
- Sung JH, Choi BG, Maeng SH, Kim SJ, Chung YH, Han JH, et al. Recovery from welding-fume-exposure-induced lung fibrosis and pulmonary function changes in sprague dawley rats. Toxicol Sci 2004;82(2):608-13.
- Karkhanis VS, Joshi JM. Pneumoconioses. The Indian Journal of Chest Diseases & Allied Sciences 2013;55:25-34.
- Chong S, Lee KS, Chung JM, Han J, Kwon OJ,Kim TS. Pneumoconiosis comparison of imaging and pathologic findings. Radiographics 2006;26(1):59-77.
- Stanescu DC, Pilat L, Gavrilescu N, Teculescu DB, Cristescu I. Aspects of pulmonary mechanics in arc welders? siderosis. Br J Ind Med 1967;24(2):143-7.
- C?mert MA, Yılmaz H, Gebeşoğlu BE, Tutkun E, Keskinkılı? B, Soydal T. Evaluation of risk factors in pneumoconiosis development among welders. Ankara Medical Journal 2014;14(1).
- Han D, Goo JM, Im JG, Lee KS, Paek DM, Park SH. Thin-section CT findings of arc-welders' pneumoconiosis. Korean J Radiol 2000;1(2):79-83.
- Yoshii C, Matsuyama T, Takazawa A, Ito T, Yatera K, Hayashi T, et al. Welder's pneumoconiosis: diagnostic usefulness of high-resolution computed tomography and ferritin determinations in bronchoalveolar lavage fluid. Intern Med 2002;41(12):1111-7.
- Tun? OK, Ayg?n R, K?kt?rk N, Ekim N, Tun? I. Respiratory findings and pulmonary function tests among the welders working for the sugar plant factory. Tuberk Toraks 2003;51(3):271-6.
- Şimşek C. Kaynak?ı akciğeri. Turkiye Klinikleri J Med Sci Sciences 1992;12(3), 212-8.
- Ozdemir O, Numanoğlu N, G?n?ll? U, Savaş I, Alper D,? G?rses H. Chronic effects of welding exposure on pulmonary function tests and respiratory symptoms. Occ Environ Med 1995;52(12):800-3.
- Tutkun E, Abusoglu S, Yilmaz H, Gunduzoz M, Evcik E, Ozis TN, et al. Farewell to an old friend: chest X-ray vs high-resolution computed tomography in welders' lung disease. Clin Respir J 2014;8(2):220-4.
- Temel O, Sakar Coşkun A, Yaman N, Sarioğlu N, Alka? C, Konyar I, et al. Occupational asthma in welders and painters. Tuberk Toraks 2010;58(1):64-70.
- Hansen KS, Lauritsen JM, Skytthe A. Cancer incidence among mild steel and stainless steel welders and other metal workers. Am J Ind Med 1996;30(4):373-82.
- Ambroise W, Wild P, Moulin JJ. Update of a meta-analysis on lung cancer and welding. Scand J Work Environ Health 2006;32(1):22-31.
- Moulin JJ. A meta-analysis of epidemiologic studies of lung cancer in welders. Scand J Work Environ Health 1997;23(2):104-13.
Yazışma Adresi (Address for Correspondence)
Dr. İpek ?ZMEN
Sağlık Bilimleri ?niversitesi S?reyyapaşa G?ğ?s Hastalıkları ve
G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi,
G?ğ?s Hastalıkları Kliniği,
İSTANBUL - TURKEY
e-mail: ipekozmen2011@gmail.com