RESEARCH ARTICLE
Doi: 10.5578/tt.59675
Tuberk Toraks 2017;65(4):291-295

Akciğer kanseri ile eş zamanlı teşhis edilen Mycobacterium tuberculosis veya
nont?berk?loz mikobakteri infeksiyonları
Abdullah ŞİMŞEK1, Serdar KALEMCİ2, Nevin MUTLU3, İlhami YAPICI1, Nil?fer Aylin ACET ?ZT?RK1
1 Bursa Prof. Dr. T?rkan Akyol G?ğ?s Hastalıkları Hastanesi, G?ğ?s Hastalıkları Kliniği, Bursa, T?rkiye
1 Clinic of Chest Diseases, Bursa Prof. Dr. Turkan Akyol Chest Diseases Hospital,?Bursa, Turkey
2 Muğla Sıtkı Ko?man ?niversitesi Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, Muğla, T?rkiye
2 Department of Chest Diseases, Faculty of Medicine, Mugla Sitki Kocman University, Bursa, Turkey
3 Bursa Ali Osman S?nmez Onkoloji Hastanesi, G?ğ?s Hastalıkları Kliniği, Bursa, T?rkiye
3 Clinic of Chest Diseases, Bursa Ali Osman Sonmez Oncology Hospital, Bursa, Turkey
?ZET
Akciğer kanseri ile eş zamanlı teşhis edilen Mycobacterium tuberculosis veya nont?berk?loz mikobakteri infeksiyonları
Giriş: Akciğer kanseri ile Mycobacterium tuberculosis veya nont?berk?loz mikobakteri (NTM) eş zamanlı birlikteliği daha ?nceki ?alışmalarda g?sterilmiştir. Bu ?alışmada akciğer kanseri ile M. tuberculosis veya NTM eş zamanlı birlikteliği g?r?len hastaların karakteristik ?zelliklerinin saptanması ama?landı.
Materyal ve Metod: 2010-2015 yılları arasında akciğer kanseri ile M. tuberculosis veya NTM eşzamanlı birlikteliği g?r?len hastalar ?alışmaya dahil edildi. Hasta bilgileri retrospektif olarak toplandı.
Bulgular: Akciğer kanseri ile M. tuberculosis veya NTM eş zamanlı birlikteliği 17 olguda (t?m akciğer kanseri olgularının %1.2'si, t?m t?berk?loz hastalarının %0.9'u) saptandı. M. tuberculosis 11 (%64.8) hastada ve NTM 6 (%35.2) hastada izole edildi. Skuam?z h?creli akciğer kanseri en sık g?r?len histolojik tipti. T?m?rler en sık ileri evrede idi (Evre III-IV, %76.5). Bronşiyal lavaj (BL) aside diren?li bakteri (ARB) sadece 4 (%23.5) hastada tespit edildi. T?berk?loz tedavisi sadece bu ARB (+) olan 4 (%23.5) hastaya başlandı. B?ylece BL ARB (-) olan 13 (%76.5) hastaya TB tedavisi başlanmadı. On yedi hastanın 7? (%41.1)'si ?ld?.
Sonu?: Doktorlar akciğer kanseri hastalarını değerlendirirken M. tuberculosis veya NTM birlikteliğini akıllarında tutmalıdır. T?berk?loz hastaları yanlışlıkla akciğer kanseri tanısı alabilir veya tam tersi de olabilir.
Anahtar kelimeler: Akciğer kanseri, Mycobacterium tuberculosis, nont?berk?loz mikobakteri.
SUMMARY
Lung cancer diagnosed with Mycobacterium tuberculosis or nontuberculosis mycobacteria concomitantly
Introduction: The concomitant occurrence of disease of Mycobacterium tuberculosis or nontuberculosis mycobacteria (NTM) and lung cancer has been reported in previous studies. We aimed to determine characteristics of the patients with lung cancer diagnosed with M. tuberculosis or NTM concomitantly.
Materials and Methods: From 2010 to 2015, the patients diagnosed with lung cancer and M. tuberculosis or NTM concomitantly were enrolled in the study. Patient data were collected retrospectively.
Results: Concomitant M. tuberculosis or NTM and lung cancer were diagnosed in 17 cases (1.2% of total lung cancer cases, 0.9% of total tuberculosis?? cases). M. tuberculosis was isolated from 11 (64.8%) patients and NTM disease was from 6 (35.2%) patients. Squamous cell carcinoma was the most common histological type. Tumoral stage was often advanced as stage III- IV (76.5%). Bronchial lavage smear positivity foracid-fast bacilli was found only in 4 (23.5%) patients. Tuberculosis treatment therapy was started only in 4 (23.5%) patients who had bronchial lavage smear positivity for acid-fast bacilli. So tuberculosis treatment was delayed for other 13 (76.5%) patients with bronchial lavage smear negative for acid-fast bacilli. Seven out of 17 (41.1%) patients died.
Conclusion: Physicians should consider concomitant M. tuberculosis or NTM when managing lung cancer. Tuberculosis patients may be mis diagnosed as lung cancer or vice versa.
Key words: Lung cancer, Mycobacterium tuberculosis, nontuberculosis mycobacteria
Geliş Tarihi/Received: 10.08.2017 - Kabul Ediliş Tarihi/Accepted: 28.08.2017
INTRODUCTION
Lung cancer (LC) is the most deadly type of cancer. Mycobacterium tuberculosis is also important cause of morbidity and mortality, especially in developing countries (1). The concomitant occurrence of diseases of pulmonary tuberculosis (TB) and LC has been reported in previous studies (2-8). Some scientists suggested that TB leads to development of cancer; others state that TB and cancer are antagonists. Also relationship between LC and nontuberculosis mycobacteria (NTM) disease was found in previous studies (9,10).???????????
It has been suggested that inflammation and pulmonary fibrosis caused by TB can induce genetic damage, which can increase LC risk (11-13). Infection-induced immunosuppression can be cause of LC in patients with TB (14). Also, cancer-induced or chemotherapy-induced immunosuppression can be reasons of TB reactivation in patients with solid tumors (15). In the present study, we aimed to determine characteristics of the patients with LC diagnosed with M. tuberculosis or NTM concomitantly and radiological characteristics and bronchoscopic locations of LC, the types and stages of LC and to calculate mortality rate in one-year.
MATERIALS and METHODS
The study involved patients diagnosed with M. tuberculosis or NTM and LC concomitantly between 2010-2015. This was a retrospective study involving 1325 patients with a confirmed diagnosis of LC by cytological and histopathological evaluation of bronchial lavage (BL) specimens or endobronchial biopsy specimens.
The diagnosis of pulmonary TB was based on consensus criteria (16): positive Ziehl-Neelsen staining for AFB and/or a single positive culture for M. tuberculosis. NTM disease was diagnosed by finding NTM bacteria in BL.
The diagnoses of LC and M. tuberculosis or NTM were classified as simultaneous when the diagnoses of M. tuberculosis or NTM and LC occurred concomitanly or when the time between the two diagnoses was < 2 months.
The patients' characteristics, radiological, bronchoscopic and microbiological features were recorded retrospectively.
Tumor staging has been made according to the seventh edition of the "TNM classification of (IASLC) malignant tumours" (17).
Mortality rate in one-year was calculated.
RESULTS
During the study period (2010-2015) a total of 1325 patients have been diagnosed with LC and 1776 patients with TB at our hospital.
Concomitant M. tuberculosis or NTM and LC were diagnosed in 17 cases (1.2% of total LC cases, 0.9% of total TB cases). M. tuberculosis was isolated from 11 (64.8%) and NTM disease was from 6 (35.2%) patients. NTM species could not be identified because of technical problem at that time. All of the patients were men. Patients age were ranging between 49 and 85. The mean age was 69.
Radiological view of 15 patients could be reached.Radiologic findings revealed mass lesion (10 cases, 66.7%), consolidation (7 cases, 46.7%), acinar infiltration (7 cases, 46.7%), nodular infiltration (7 cases, 46.7%), pleural effusions (7 cases, 46.7%), atelectasia (4 cases, 26.7%), fibrotic infiltrates (4 cases, 26.7%), ground glass appearance (3 cases, 20%), lymphadenopathy (3 cases, 20%), cavitary infiltration (3 cases, 20%), pericardial effusion (1 case, 6.6%) (Figure 1). Lesions were mostly unilateral and in the right lung (10 cases, 66.7%). Multilobar involvement were found in 8 cases (53.3%).
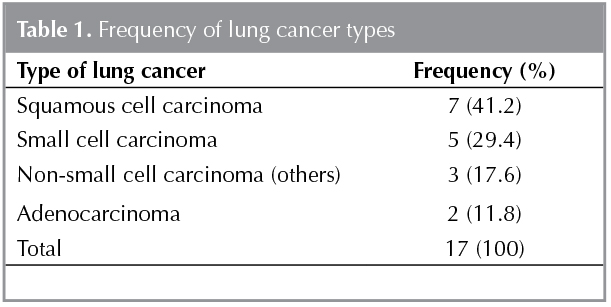
If a subtype of non-small cell carcinoma case could not be determined it was called non-small cell carcinoma others. Squamous cell carcinoma was the most common histological type diagnosed with TB concomitantly (41.2%) (Table 1). Small cell carcinoma was diagnosed in 5 (29.4%) patients.
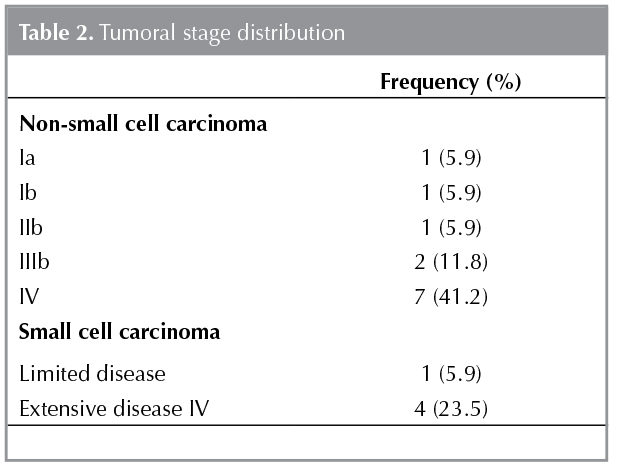
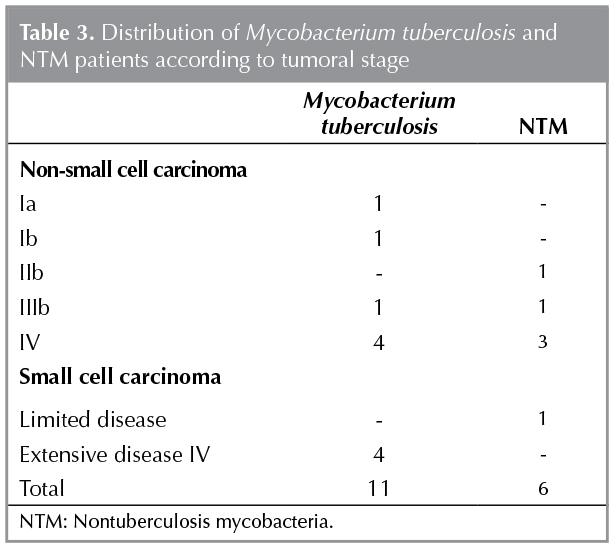
Tumoral stage was of ten advanced as stage III-IV (53%) for non-small cell carcinoma, extensive disease IV (23.5%) for small cell carcinoma (Table 2). So, 76.5% of all LC were advanced. Four out of 6 NTM patients were in stage III-IV (66.6%), 9 out of 11 TB patients were in stage III-IV (81.8%) (Table 3).
BL smear positivity for AFB was found only in 4 (23.5%) patients. BL smear was negative for AFB in 13 (76.5%) patients. BL culture for TB was positive in all the patients.
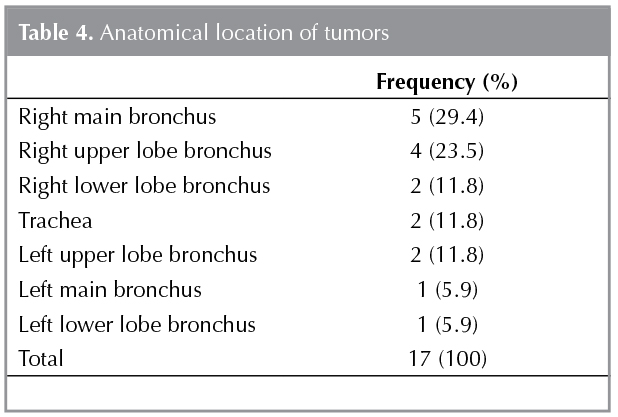
Anatomically, the bronchoscopic findings were located primarily in the right main bronchus in 5 (29.4%) patients, and the right upper lobe bronchus in 4 (23.5%) patients (Table 4).
Seven out of 17 (41.1%) patients died in one year.? Two out of 6 NTM patients (33.3%) and 5 out of 11 TB patients (45.4%) died in one year.
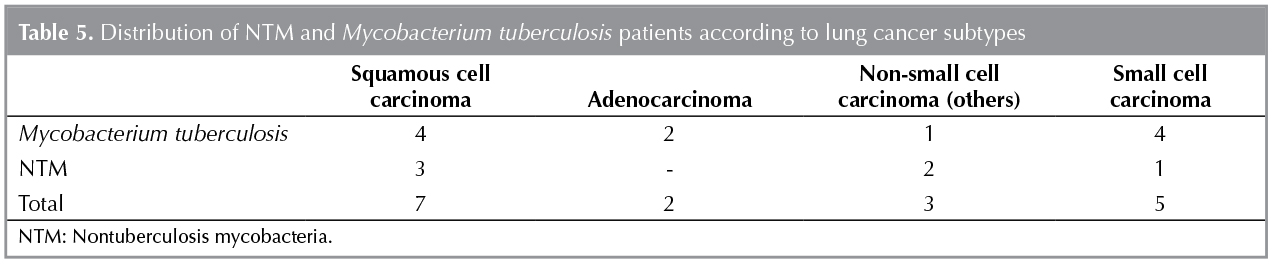
Both M. tuberculosis and NTM was diagnosed mostly with squamous cell carcinoma concomitantly (Table 5). Four out of 5 patients with small cell carcinoma (80%) was diagnosed concomitant with M. tuberculosis, only 1 of them (20%) was with NTM. None of the patients with adenocarcinoma was found with NTM concomitantly.
DISCUSSION
In present study, concomitant M. tuberculosis or NTM and LC were diagnosed in 1.2% of total LC cases, and in 0.9% of total TB cases. We consider that these ratioswould be higher, if physicians had thought about the possibility of concomitant M. tuberculosis or NTM when managing LC. Because then they would investigate BL in all patients to prove TB. These findings similar to the literature that the frequency of LC accompanying pulmonary TB is around 1% and that of active pulmonary TB accompanying LC is closeto 4% (18). Watanabe et al. published analysis of 758 of LC and coexistence of cancer and TB was found in 2.1% of cases (19,20). The frequency of concomitant development of LC is 25-fold in patients with pulmonary TB compared to the expected incidence of LC in healthy individuals, which appears to indicate a higher morbidity rate of LC in patients affected by pulmonary TB (18). Some research showed that scars, which remain after healing of tuberculoses' lesion, could cause development of LC (21). Although it was previously believed that patients with pulmonary TB are less likely to be affected by LC, the reverse may be true (18).
In this study, most commonly seen radiologic findings were mass lesion (66.7%), consolidation (46.7%), acinar infiltration (46.7%), nodular infiltration (46.7%), pleural effusions (46.7%), respectively. Lesions were mostly unilateral and in the right lung (66.7%) and also multilobar (53.3%). Bronchoscopic findings were located primarily in the right bronchial system (64.7%).
Squamous cell carcinoma was the most common histological subtype in our study (41.2%) that was similar to the studies of Morales-Cardia et al. Varol Y et al (22,23). But, adenocarcinoma was the most common subtype in other series (20,24).
Both M. tuberculosis and NTM was diagnosed mostly with squamous cell carcinoma concomitantly. Most of the patients with small cell carcinoma (80%) was diagnosed concomitant with M. tuberculosis. None of the patients with adenocarcinoma was found with NTM concomitantly.
In this study, LC stage was advanced (76.5%). Similar results were reported in previous studies (22,23,25,26).
In our study, NTM was isolated from 35.2% of the 17 patients and M. tuberculosis was from 64.8% of them. NTM patients were in advanced stage (66.6%) that was similar to the study of Tamura et al. (9). Relationship between LC and NTM was found in previous studies (9,10). Tuberculosis patients were also in advanced stage (81.8%). So LC in the TB group were in far-advanced.
In present study, 41.1% of patients died in one year. 33.3% of NTM patients and 45.4% of TB patients died in one year. The difference in mortality rates between TB and NTM patients might be due to presence of more advanced LC in TB group than NTM group. Leung et al. have suggested that TB is independently associated with subsequent mortality due to LC (27). Patients with LC diagnosed with TB had worse prognosis than those with LC without TB (28).
TB treatment was started only in 4 (23.5%) patients at the beginning who had BL smear positivity for AFB. The other 13 patients with BL smear negative for AFB were referred to onchology department without TB treatment. So TB treatment was delayed for these patients. These findings are reverse to that of Agrawal who suggested that large numbers of the bronchogenic carcinoma patients were mis diagnosed as a case of TB, this leads to significant delay in diagnosis and progression of cancer and results in poor outcome and lower survival (29). But according to present study, TB patients were also mis diagnosed as only LC and that contributed diagnostic and treatment delay in TB. So once LC has been diagnosed, possible presence of concomitant TB should be kept in mind.
Our study has certain limitations. Primarily, due to the retrospective nature of the study, we relied on electronic medical records as our source of patient data.
CONCLUSION
Physicians should consider concomitant M. tuberculosis or NTM when managing lung cancer. TB patients may be mis diagnosed as LC or vice versa.
REFERENCES
- World Health Organization [homepage on the Internet]. Geneva: World Health Organization. [cited 2013 Apr 1]. WHO REPORT 2009 Global Tuberculosis Control- Epidemiology, Strategy, Financing.
- Brenner AV, Wang Z, Kleinerman RA, Wang L, Zhang S, Metayer Cet al. Previous pulmonary diseases and risk of lung cancer in Gansu Province, China. Int J Epidemiol 2001;30:118-24.
- Dacosta NA, Kinare SG. Association of lung carcinoma and tuberculosis. J Postgrad Med 1991;37:185-9.
- Liang HY, Li XL, Yu XS, Guan P, Yin ZH, He QC, et al. Facts and fiction of the relationship between preexisting tuberculosis and lung cancer risk: a systematic review. Int J Cancer 2009;125:2936-44.
- Shiels MS, Albanes D, Virtamo J, Engels EA. Increased risk of lungcancer in men with tuberculosis in the alpha-tocopherol, beta-carotene cancer prevention study. Cancer Epidemiol Biomarkers Prev 2011;20:672-8.
- Wu CY, Hu HY, Pu CY, Huang N, Shen HC, Li CP, et al. Pulmonary tuberculosis increases the risk of lung cancer: a population-based cohort study. Cancer 2011;117:618- 24.
- Yu YH, Liao CC, Hsu WH, Chen HJ, Liao WC, Muo CH, et al. Increased lung cancer risk among patients with pulmonary tuberculosis: a population cohort study. J Thorac Oncol 2011;6:32-7.
- Baysungur V, Mısırlıoglu AK. Tuberculosis and lung cancer concomitance. Toraks Cerrahisi B?lteni 2015;9:324-30.
- Tamura A, Hebisawa A, Sagara Y, Suzuki J, Masuda K, Baba M, et al. Pulmonary nontuberculous mycobacteriosis in patients with lung cancer. Kekkaku 2004;79:367-73.
- Tamura A, Hebisawa A, Kusaka K, Hirose T, Suzuki J, Yamane A, et al. Relationship between lung cancer and Mycobacterium avium complex isolated using bronchoscopy. The Open Respiratory Medicine Journal 2016;10:20-8.
- Ballaz S, Mulshine JL. The potential contributions of chronic inflammation to lung carcinogenesis. Clin Lung Cancer 2003;5:46-62.
- Coussens LM, Werb Z. Inflammation and cancer. Nature 2002;420:860-7.
- Engels EA. Inflammation in the development of lung cancer: epidemiological evidence. Expert Rev Anticancer Ther 2008;8:605-15.
- Rybacka-Chabros B, Madziuk S, Berger-Lukasiewicz A, Dako-Mroziska M, Milanowski J. The coexistence of tuberculosis infection and lung cancer in patients treated in pulmonary department of Medical Academy in Lublin during last ten years (1990-2000). Folia Histochem Cytobiol 2001;39:73-4.
- Kim HR, Hwang SS, Ro YK, Jeon CH, Ha DY, Park SJ, et al. Solid-organ malignancy as a risk factor for tuberculosis. Respirology 2008;13:413-9.
- Conde MB, Melo FA, Marques AM, Cardoso NC, Pinheiro VG, Dalcin P, et al. III Brazilian Thoracic Association Guidelines on tuberculosis. J Bras Pneumol 2009;35:1018-48.
- Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. International Association for the Study of Lung Cancer International Staging Committee, Participating Institutions. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forth coming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol 2007;2:706-14.
- Komatsu H. Clinical characteristics and problems in patients with coexistent lung cancer and pulmoner tuberculosis. IRYO 1999;53:499-503.
- Tamura A, Hebisawa A, Hayashi K, Sagara Y, Kawabe Y, Nagayama M, et al. Lung cancer in patients who had received thorocoplasty for pulmonary. Kekkaku 1999;74:797-802.
- Watanabe A, Tokue Y, Takashi H, Sato K, Nukiwa T, Honda Y, et al. Management of mycobacteriosis in general hospital without isolation word for tuberculosis patients. Clinical study on pulmonary tuberculosis associated with lung cancer patients. Kekkaku 1999;74:157-62.
- Zhingel IP, Tsimmerinov IE. Diagnosis of cancer of the lung in patients with tuberculosis subjects with post-tuberculosis changes of the lungs. Probl Tuberkuloza 1999;6:26-9.
- Morales-Garcia C, Parra-Ruiz J, Sanchez-Martinez JA, Delgado-Martin AE, Amzouz-Amzouz A, et al. Concomitant tuberculosis and lung cancer diagnosed by bronchoscopy. Int J Tuberc Lung Dis 2015;19:1027-32.
- Varol Y, Varol U, Unlu M, Kayaalp I, Ayrancı A, Dereli MS, et al. Primary lung cancer coexisting with active pulmonary tuberculosis. Int J Tuberc Lung Dis 2014;18:1121-5.
- Silva DR, Valentinij Jr DF, M?ller AM, de Almeida CP, Dalcin P de T.? Pulmonary tuberculosis and lung cancer: simultaneous and sequential occurrence. J Bras Pneumol 2013;39:484-9.
- Martinez ME, Aparicio UJ, Cordero RP, Sanchis AJ, Leon FM, Perpina TM. Coexistence of bronchogenic carcinoma and active pulmonary tuberculosis. Arch Bronconeumol 1995;31:32-4.
- Erbaycu AE, G?lpek M, Tuksavul F, Uslu ?, G?neş ?, G??l? SZ. The comorbidity of pulmonary tuberculosis at the time of diagnosis of patients with lung cancer. İzmir G?g?s Hastanesi Dergisi 2006;20:11-4.
- Leung CC, Hui L, Lee RSY, Lam TH, Yew WW, Hui DSC, et al. Tuberculosis is associated within creased lung cancer mortality. Int J Tuberc Lung Dis 2013;17:687-92.
- Chen YM, Chao JY, Tsai CM, Lee PY, Perng RP. Shortened survival of lung cancer patients initially presenting with pulmonary tuberculosis. Jpn J Clin Oncol 1996;26:322-7.
- Agrawal A, Kumar P, Tandon R, Singh S, Singh L, Sharma S. Pulmonary tuberculosis as a confounder for bronchogenic carcinoma due to delayed and mis diagnosis. Ind J Comm Health 2013;25:438-44.
Yazışma Adresi (Address for Correspondence)
Dr. Abdullah ŞİMŞEK
Bursa Prof. Dr. T?rkan Akyol G?ğ?s Hastalıkları Hastanesi,
G?ğ?s Hastalıkları Kliniği,
Bursa - T?rkiye
e-mail: abdullahsimsek1@yahoo.com.tr