RESEARCH ARTICLE
Doi: 10.5578/tt.48618
Tuberk Toraks 2017;65(1):18-24

Sigara i?me durumlarına g?re ?ğretmenlerin sosyodemografik ?zelliklerinin ve
yaşam kalitelerinin değerlendirilmesi:
T?rkiye'nin Doğu Karadeniz b?lgesinden kesitsel bir ?alışma
Dilek ?AKMAK?I KARADOĞAN1, ?zg?r ?NAL2, Deniz SAY ŞAHİN3, Sonnur YAZICI4, Yal?ın KANBAY5
1 Clinic of Chest Diseases, Hopa State Hospital, Artvin, Turkey
1 Hopa Devlet Hastanesi, G?ğ?s Hastalıkları Kliniği, Artvin, T?rkiye
2 Society Health Center, Burdur Public Health Directorate, Burdur, Turkey
2 Burdur Halk Sağlığı M?d?rl?ğ?, Toplum Sağlığı Merkezi, Burdur, T?rkiye
3 Department of Individual and Community Problems, Faculty of Economic and Administrative Sciences,
Mehmet Akif Ersoy University, Burdur, Turkey
3 Mehmet Akif Ersoy ?niversitesi, İktisadi ve İdari Bilimler Fak?ltesi, Birey ve Toplum Sorunları Anabilim Dalı,
Burdur, Turkey
4 Health Services Directorate, Hopa State Hospital, Artvin, Turkey
4 Hopa Devlet Hastanesi, Sağlık Hizmetleri M?d?rl?ğ?, Artvin, T?rkiye
5 Department of Psychiatric Nursing, Faculty of Health Sciences, Artvin Coruh University, Artvin, Turkey
5 Artvin ?oruh ?niversitesi, Sağlık Bilimleri Fak?ltesi, Psikiyatri Hemşireliği B?l?m?, Artvin, T?rkiye
?ZET
Sigara i?me durumlarına g?re ?ğretmenlerin sosyodemografik ?zelliklerinin ve yaşam kalitelerinin değerlendirilmesi: T?rkiye'nin Doğu Karadeniz b?lgesinden kesitsel bir ?alışma
Giriş: Sigara ile ilişkili sağlık sorunları ?zellikle uzun s?reli kullanımından sonra sık g?r?l?r ve dolayısıyla sigaranın k?m?latif yan etkileri gen? yaşlarda pek g?r?lmez. Bu nedenle, sigaranın o andaki yan etkilerini değerlendirmede yaşam kalitesi temel bir kriter haline gelmiştir. Bu ?alışmamızda ama?larımız ?ğretmenlerin sigara i?melerini etkileyen fakt?rleri değerlendirmek ve sigara i?me durumlarına g?re yaşam kalitelerini kıyaslamaktır.
Materyal ve Metod: Bu kesitsel ?alışma 1 Mart 2015 ila 30 Haziran 2015 tarihleri arasında yapıldı ve Hopa'da bulunan b?t?n devlet okullarındaki ?ğretmenler ?alışmaya dahil edildi. Sosyodemografik veri formu ve WHOQOL-bref ?l?eği kullanıldı. İstatistiksel analiz i?in SPSS 20 kullanıldı. ?l?eğin g?venilirliğini değerlendirmek i?in her bir alanının Cronbach alfa değerleri hesaplandı.
Bulgular: İstatistiksel analiz 327 kişinin verilerine uygulandı. ?ğretmenlerin yaş ortalaması 34.2 ? 8.73 idi ve %50.2'si kadındı. ?ğretmenlerin ?oğu (%67.8) hi? sigara i?memişti, aktif i?icilerin oranı %20.1 idi. Aktif i?icilerin ortalama Fagerstr?m skoru 4.1 ? 1.96 idi. Multinominal lojistik regresyon analizi erkek cinsiyet ile aktif i?icilik arasında pozitif ilişki olduğunu g?sterdi (OR= 2.25;95% CI: 1.17-4.32; p< 0.05). Yaşam kalitesi algısı ve sağlık durumu algısı aktif i?icilerin hi? i?meyenlere g?re daha d?ş?kt? (p< 0.05). Ancak, diğer yaşam kalitesi alanlarında sigara i?me durumlarına veya bağımlılık durumlarına g?re farklılık saptanmadı.
Sonu?: Bu ?alışma ?ğretmenler arasında aktif sigara i?iciliği oranında ?nceki yıllara g?re bir d?ş?ş olduğunu, ayrıca aktif i?icilerin hi? i?meyenlere g?re yaşam kalitelerini ve sağlık durumlarını daha k?t? algıladıklarını g?stermiştir.
Anahtar kelimeler: Sigara, yaşam kalitesi, yaşam kalitesi algısı, sağlık durumu algısı, ?ğretmenler
SUMMARY
Evaluation of school teachers' sociodemographic characteristics and quality of life according to their cigarette smoking status: a cross-sectional study from the eastern Black Sea region of Turkey
Introduction: Smoking related health disorders are particularly common after long-term cigarette use and accordingly cumulative side effects of smoking usually do not appear in younger individuals. Therefore, for evaluating the contemporary effects of smoking in healthy individuals quality of life has become a fundamental criterion. In this study our aims are evaluating factors affecting school teachers' smoking status and comparing quality of life them according to their cigarette smoking status.
Materials and Methods: This cross-sectional study, conducted between March 1 and June 30, 2015, included all government school teachers in Hopa. A sociodemographic data form and World Health Organisation Quality of Life-bref (WHOQL-bref) questionnaire were used. Statistical analysis was performed via SPSS 20. To evaluate the reliability of the WHOQOL-bref questionnaire, Cronbach's alpha co-efficiency was calculated for each domain separately.
Results: Statistical analysis was performed on 327 participants' data. The mean age of the teachers was 34.2 ? 8.73 and 50.2% of them were female. Most of the teachers were never smokers (67.8%) and current smokers' made up 20.1% of the population. Mean Fagerstr?m score of current smokers was 4.1?1.96. Multinominal logistic regression analysis showed that there was a positive association between male gender and current smoking (OR= 2.25; 95% CI: 1.17-4.32; p< 0.05). Perception of quality of life and perception of health status scores were lower in the current smoker group as compared to never smokers (p< 0.05). However, other quality of life domains were not significantly different among smoking groups. Also, none of the quality of life domains differed significantly according to current smokers' nicotine dependence level.
Conclusion: This study reflected a decrease in current smoking prevalence among school teachers compared to previous years. Also, the perception of quality of life and perception of health status scores were lower in the current smoker group as compared to never smokers.
Key words: Cigarette smoking, quality of life, perception of quality of life, perception of health status, school teachers
Geliş Tarihi/Received: 10.10.2016 • Kabul Ediliş Tarihi/Accepted: 13.02.2017
INTRODUCTION
Smoking is one of the most prevalent causes of preventable disease worldwide. Besides its health-related harmful effects, it has also negative social and economic effects (1). Studies have shown that smoking-related health disorders are particularly common after long-term cigarette use (2). Accordingly, in younger individuals the cumulative side effects of smoking usually do not appear. When evaluating the current effects of smoking within that age group, quality of life is an important determinant. Therefore, in recent years, quality of life has become a fundamental criterion for evaluating the contemporary effects of smoking. The World Health Organisation Quality of Life-bref (WHOQL-bref) questionnaire is an appropriate meter to evaluate life quality among a healthy population; it is better suited to show overall quality of life than others, like the 36-Item Short Form Health Survey (SF-36), that prioritize health-related quality of life (3).
There is a basis in the literature for evaluating quality of life (QL) through the lens of smoking habits. In an international study Funahashi et al. have found no statistically significant difference between QL of smokers and non-smokers (4). In another study Heikkinen et al. have found HRQL and overall quality of life of daily smokers to be lower compared to individuals who had never smoked (2).
There are a few studies from Turkey that evaluate the relationship between smoking status and quality of life in healthy individuals, but the data is limited (5-7). Unsal et al. evaluated the health-related quality of life of 586 men according to smoking status and found lower scores in the smoker population as compared to non-smokers (7). Taspinar et al. evaluated 85 individuals between the ages of 19 and 64. They found a negative correlation between nicotine dependence level and quality of life (8).
It is well known that quality of life is also affected by gender, socioeconomic status, age, behavioral risk factors, environment, and diseases (9). None of the studies mentioned above used a study population from the same socioeconomic class. In our study we intended to evaluate the link between cigarette smoking and quality of life of in a population of individuals in the same socioeconomic class and geographic area. Therefore our study population consisted of school teachers in the eastern Black Sea region of Turkey. Our findings could be important in characterizing the relationship between quality of life and smoking, which may facilitate the development of patient-centered interventions.
MATERIALS and METHODS
Settings and Sample
This cross-sectional study, conducted between March 1 and June 30, 2015, used as its population government school teachers in Hopa, a seaside town in the eastern Black Sea region of Turkey with a population of approximately 20.000. There are 37 schools in Hopa, falling under the categories of primary, secondary, and high schools. There are 463 teachers in total working in government schools in Hopa. We aimed for full participation in the study but ultimately used data from 327 participants. The study was approved by Artvin ?oruh University's Ethics Committee and permission for study was given from the Artvin director of education and Artvin Government Hospital's general secretary. The researchers were granted permission from the WHO for the use of the WHOQL-bref.
Data Collection
Self-administered questionnaires following written informed consent were given to the teachers who agreed to join the study. The questions in the first part of the questionnaire covered the sociodemographic characteristics of the participants: age (in years), gender (male, female), marital status (single, married, divorced), spouse's job when applicable, and number of persons living within their house. There were then questions about comorbidities, weight, height, and smoking status. Smoking status was classified as never smoker, former smoker, or current smoker. Someone who has smoked greater than 100 cigarettes in their lifetime and has smoked in the last 28 days were classified as current smoker, someone who has smoked greater than 100 cigarettes in their lifetime but has not smoked in the last 28 days were classified as former smoker and someone who has not smoked greater than 100 cigarettes in their lifetime and do not currently smoke were classified as never smoker. Current and former smokers were also asked about the age at which they smoked their first cigarette. The Fagerstr?m Tolerance of Nicotine Dependence (FTND) test was performed on current smokers (10). Current smokers were also asked about their smoking cessation ideation ("Do you want to quit smoking?"), beliefs about quitting ("Do you think you can quit?"), and attempts at cessation ("Did you ever try to quit?").
The other part of the questionnaire was composed of the WHOQL-bref questionnaire (11). The reliability and validity of the Turkish version of the questionnaire have previously been established (12). WHOQL-Bref questionnaire begins with 2 questions about perception of quality of life and perception of health status of the participant and the rest of the questionnaire consists of 26 total questions and evaluates 4 domains. Physical domain evaluates 7 areas: managing daily tasks, drug/medicine requirements, livelines, movement, pain/disabilities, sleep/rest status, and work ability. Each is scored out of 5, with 35 points as the maximum score. Psychological domain includes topics: body image/appearance, negative feelings, self-esteem, positive feelings, religious/personal beliefs, and thinking/learning/concentration. Maximum score is 30 in that domain. Social relations domain has three questions, which cover relationships with others, social support, and sexual life. Maximum score is 15 in that domain. Environment domain consists of 8 areas of focus: economic resources, physical security, healthcare facilities, availability/quality of social support, home conditions, new knowledge learning availability, rest/free time activities, and physical environment, which includes pollution, traffic, noise pollution, climate, and transportation. Maximum score is 40 in that domain. After calculating the raw scores for each domain we transferred it to out of 100 points.
Statistical Analysis
Statistical analysis was performed via SPSS 20. To evaluate the reliability of the WHOQOL?bref questionnaire, Cronbach's alpha co-efficiency was calculated for each domain separately. Categorical variables were described using their absolute and relative frequencies, while quantitative variables were described by the mean and standard deviation. To evaluate the relationship between independent variables (demographic variables, quality of life domains) and dependent variables (smoking status, Fagerstr?m score), Pearson's chi-square test was used for categorical variables. One-way anova with Tukey tests or independent sample t tests were used where applicable for numerical variables. The associations were considered significant at a p< 0.05. A multinominal logistic regression analysis was done to investigate the factors associated with former smokers and current smokers, while never smokers were considered as a reference group. Results were expressed using beta and odds ratio with a 95% confidence interval (CI).
RESULTS
In total 400 teachers agreed to fill out the questionnaire. At the time of data evaluation 73 of them were excluded because of incomplete or contradictory statements. Statistical analysis was performed on 327 participants' data. Cronbach's alpha values in the physical, psychological, social relations, and environmental domains of the WHOQL-bref questionnaire were 0.757, 0.713, 0.705, and 0.825, respectively.
Mean age of the teachers was 34.2 ? 8.73 (min 21, max 63); 78.8% of them were younger than 41 years old. Male-female ratio was nearly equal (49.8% versus 50.2%). Mean age of female teachers was 31.9 ? 7.78, while that of males was 36.6 ? 9.65. Detailed sociodemographic characteristics of the participants are seen in Table 1.

Most of the teachers were never smokers (67.8%); former smokers made up 11.9% of the population, current smokers made up 20.1%. Mean age of initiation to smoking was 21.07 ? 2.19.
When never smokers were used as the reference group in multinominal logistic regression analysis, the majority of current smokers were male (OR= 2.25; 95% CI: 1.17-4.32; p< 0.05). Among former smokers, there were more married teachers than unmarried teachers (OR= 4.14; 95% CI: 1.17-14.5; p< 0.05). Among former smokers more had a BMI greater than or equal to 25 kg/m2 (OR= 2.54; 95% CI: 1.16-5.5; p< 0.05) (Table 1).
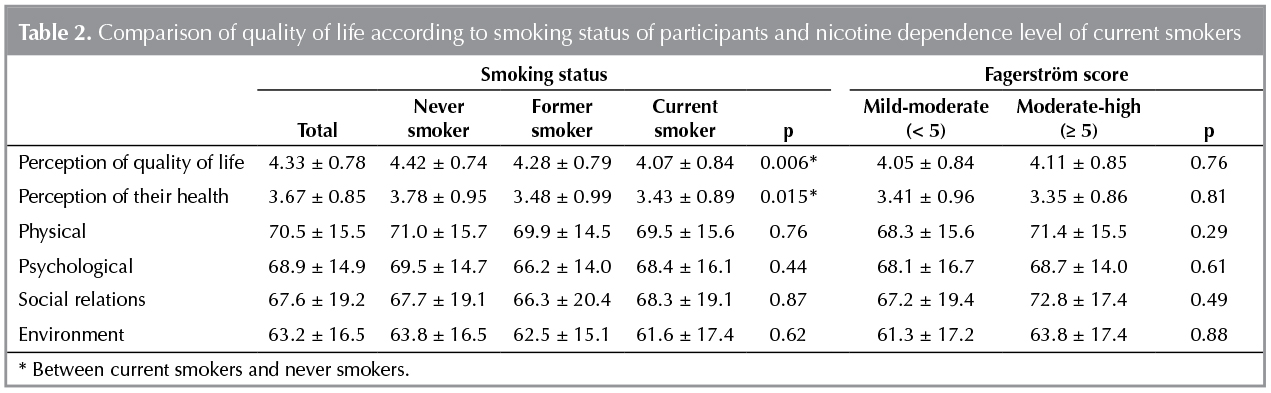
Table 2 shows the comparison of quality of life according to smoking status and nicotine dependence levels of current smokers. Perception of quality of life and perception of health status scores were lower in the current smoker group as compared to never smokers (p values were 0.006 and 0.015, respectively). The other quality of life domains were not significantly different among smoking groups. The mean Fagerstr?m score of current smokers was 4.1 ? 1.96 (min 1, max 10). None of the quality of life domains differed significantly according to current smokers' nicotine dependence level.
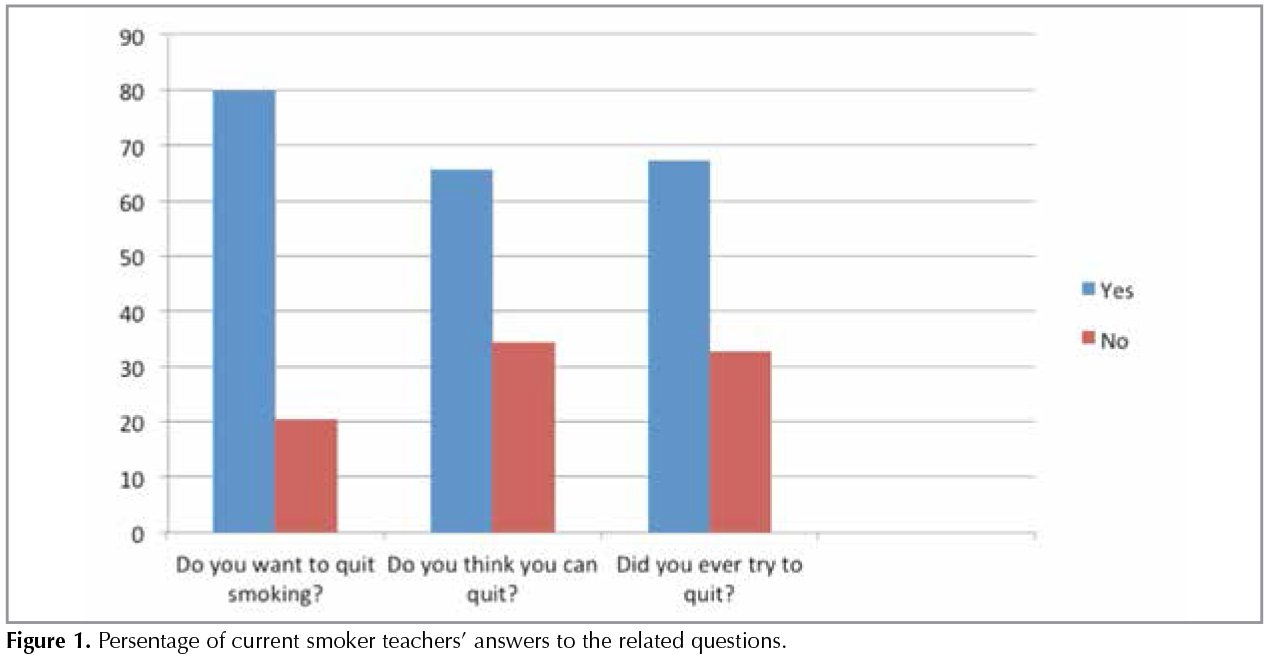
Among current smokers 77.2% (51 teachers) want to quit smoking, 63.6% (42 teachers) think that they can quit, and 65.1% (43 teachers) have tried to quit at least once (Figure 1).
DISCUSSION
In this cross-sectional study we evaluated the sociodemographic characteristics and quality of life of teachers according to their cigarette smoking status. We found the overall prevalence of current smoking among teachers to be 20.1%; a lower rate than previous Turkish studies evaluating teachers' smoking status. A study from Turkey conducted in 2002 found the percentage of current smokers among school teachers to be 52.4; in another study in 2005 the prevalence of current smokers was 32.5% (13,14). A 2006 study found 42.7% of teachers in Turkey were current smokers-an increase from the previous year but still lower than the amount of smoking school teachers in 2002, which was over half of the population (15). The decreasing smoking ratio has been recorded not only in teachers but also in the whole population of the country (16). This decrease is likely related to Turkey's signature on the Framework Convention on Tobacco Control with the World Health Organization (WHO FCTC) in 2004, which initialized effective tobacco control programs nationwide. Due to the tobacco control programs, smoking has newly been forbidden in closed areas, schools, or school gardens. In our study, among current smokers, most wanted to quit or have attempted to quit at least once. To further lower smoking rates teachers should be informed not only about the harmful effects of smoking but also about the available smoking cessation interventions. They should also be encouraged to apply for smoking cessation programs or outpatient clinics, which are currently free of charge and provided by the government.
Of the demographic characteristics, only the male gender was associated with current smoking, as found in previous studies (17,18). Because smoking is a behavior associated with? the male gender, gender roles plays a key role on this effect.
Quality of life (QL) is a common metric to assess the clinical status of smokers. It has been pointed out that these self-rated measures of QL may be a marker of poor health (9). It has also been shown that self-perception of "poor" health status has been associated with two-fold higher mortality risk, compared to those who perceive they are in "excellent" health (19). In previous studies, QL of smokers has been measured by both generic instruments and smoking-specific scales (9). In our study, we preferred the WHOQL?bref questionnaire, because our study group consisted of healthy individuals. Furthermore, that questionnaire has been adapted and validated for use in Turkey (12). From our results we found that the perception of quality of life and perception of health status scores were lower in the current smoker group compared to never smokers (p values were 0.006 and 0.015, respectively). None of the other quality of life domains were significantly different between smoking groups.
Previous studies have shown similar results, for the most part. In the Finish adult population, daily smokers had both lower HRQL and overall QL than never smokers (2). But in a Japanese population, the SF-36 scores of non-smokers and smokers showed no significant differences (4). An Iranian study using the WHOQL?bref found lower QL scores among current smokers compared to non-smokers (20).
It is difficult to compare our results with these studies; one reason is that many of the? previous studies used different QL questionnaires than we used in our study. Another reason is that our study population's mean age was younger than that of previous studies. The Japanese study's population mean age was 52.2 among males, 55.9 among females. In the Finish study the mean age was 51.3 among men, and 54.4 among women. Our study population's mean age was 36.6 ? 9.65 among males, 31.9 ? 7.78 among females. This could be the reason for the low perception scores of questionnaire, which has not affected the individual clinically, accordingly no difference measured in the other domains. Because it is known that smoking-related diseases and discomforts start after long-term use, at this younger age the individuals may not feel the adverse effects of smoking. Another factor may be the low nicotine dependence level of our study population. The mean Fagerstr?m score of current smokers was 4.1 ? 1.96 in our study. Previous studies have shown a link between smoking dependence level and QL. Higher Fagerstr?m scores have been associated with worse QL (21,22). A final reason that this study differs from others may be the cultural differences; for example, in the Japanese study the absence of difference in QL between smoking groups has been explained by the possibility of the Japanese population's lower sensitivity to and disclosure of the minor subclinical adverse health effects from smoking (4). Our study participants may be less aware of the minor subclinical adverse effects of smoking in their lives, however, low scores of perception of quality of life and perception of health status can indicate upcoming adverse subclinical effects, which is why we chose to evaluate perceptions in a population of this age.
Strengths and Limitations
This study had several criteria that both validate its results and distinguish it from similar studies in the literature. The study population was in the same sociodemographic class; all of them were school teachers. Therefore this eliminates the possibility of selection bias. The data form and questionnaire were self-administrative, eliminating potential pressure to give a "right" answer to a researcher. We ensure that our study population's education level was high enough to correctly understand and complete the forms.
The study's limitations stem from its design. The study design is cross-sectional; this limits our ability to detect the exact effect of smoking on health quality.
Conclusion
This study reflected a decrease in current smoking prevalence among school teachers, and a common desire to quit. For a more decreased rate, they should be incentivized to quit smoking and informed about smoking cessation interventions. We also found that current smokers have a lower overall perception of quality of life and health status compared to never smokers. Perception is referred to as the beginning of knowledge in philosophy. In our point of view, this study demonstrates that before directly encountering subclinical smoking-related adverse effects, individuals are realizing their ongoing worse health status and health quality. At younger ages-before subclinical or clinical health worsening due to smoking-perception scores could be a good determinant to show the current effects of smoking. Ideally, these results can be used to motivate smokers in their attempts at cessation.
REFERENCES
- Ekpu VU, Brown AK. The economic impact of smoking and of reducing smoking prevalence: review of evidence. Tob Use Insights 2015;8:1-35. doi: 10.4137/TUI.S15628. eCollection 2015.
- Heikkinen H, Jallinoja P, Saarni SI, Patja K. The impact of smoking on health-related and overall quality of life: a general population survey in Finland. Nicotine Tob Res? 2008;10:1199-207. doi: 10.1080/14622200802163142.
- Huang IC, Wu AW, Frangakis C. Do the SF-36 and WHOQOL-BREF measure the same constructs? Evidence from the Taiwan population. Qual Life Res 2006;15:15-24.
- Funahashi K, Takahashi I, Danjo K, Matsuzaka M, Umeda T, Nakaji S. Smoking habits and health-related quality of life in a rural Japanese population. Qual Life Res 2011;20:199-204. doi: 10.1007/s11136-010-9748-8.
- Şen N, Arslan GG, ?oban A, G?ng?r N, Kulbakan S, Solar M. Study on the effects of situation of cigarette smoking on university students' quality of life. Turk Thoracic J 2008;9: 68-73.
- Kartal M, Mıdık ?, B?y?kakkuş A. Tobacco smoking and its effect on quality of life of medical students in Ondokuz Mayıs University. Turk Thoracic J 2012;13:11-7.
- Unsal A, Ayranci U, Tozun M. Frequency of smoking among males and its impact on the quality of life. Pak J Med Sci 2010;26;163-7.
- Taspinar B, Taspinar F, Aksoy CC, Afsar A. Investigation of the effects of nicotine dependence levels on quality of life and depressive symptoms. J Addict Res Ther 2014; 5:196. doi:10.4172/2155-6105.1000196.
- Goldenberg M, Danovitch I, IsHak WW. Quality of life and smoking. Am J Addict 2014;23:540-62. doi: 10.1111/j.1521-0391.2014.12148.x.
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerstr?m KO. The fagerstr?m test for nicotine dependence: a revision of the fagerstr?m tolerance questionnaire. Br J Addict 1991;86:1119-27.
- Orley J. WHOQ OL-BREF: Introduction, administration, scoring and generic version of the assessment. Geneva: Program on Mental Health, 1996.
- Fidaner F, Fidaner C, Eser SY. Psychometric characteristics of WHOQOL-100 and WHOQOL-BREF. WHOQOL-100 ve WHOQOL-BREF in psikometrik ?zellikleri. Psikiyatri Psikoloji Psikofarmakoloji Dergisi 1999;7(Suppl 2):S23-40.
- Demirel Y, Toktamış A, Nur N, Sezer E. Smoking among the primary school teachers. T?rkiye Klinikleri J Med Sci 2004;24:492-7.
- Fidan F, Sezer M, Demirel R, Kara Z, ?nl? M. Smoking status of teachers and their attitudes about smoking restriction. Turk Thoracic J 2006;7:196-9.
- Kutlu R, ?ivi S. The Frequency and affecting factors of smoking among the high school teachers in Konya. TAF Prev Med Bull 2007;6:273-8.
- Public Health Institution of Turkey. Global Adult Tobacco Survey 2012. Available from: http://www.who.int/tobacco/surveillance/survey/gats/report_tur_2012.pdf?ua=1.
- Gencer M, Ceylan E, Yengil E, Ethemoğlu G. The results of the cigarette questionnaire applied to the teachers of primary school in Şanlıurfa. Turkiye Klinikleri Arch Lung 2007;8:5-9.
- Coşkun F, Karadağ M, Ursavaş A, Ege E. Smoking habits of the teachers and their opinion about the new law. Eurasian J Pulmonol 2010;12:119-24.
- DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. A meta-analysis. J Gen Intern Med 2006;21:267-75.
- Toghianifar N, Najafian J, Pooya A, Rabiei K, Eshrati B, Anaraki J, et al. Association of smoking status with quality of life in a cross-sectional population-based sample of Iranian adults: Isfahan Healthy Heart Program. Asia Pac J Public Health 2012;24:786-94. doi: 10.1177/1010539511403800.
- Wilson D, Parsons J, Wakefield M. The health-related quality-of-life of never smokers, ex-smokers, and light, moderate, and heavy smokers. Prev Med 1999;29:139-44.
- Schmitz N, Kruse J, Kugler J. Disabilities, quality of life, and mental disorders associated with smoking and nicotine dependence. Am J Psychiatry 2003;160:1670-6.
Yazışma Adresi (Address for Correspondence)
Dr. Dilek ?AKMAK?I KARADOĞAN
Hopa Devlet Hastanesi,
G?ğ?s Hastalıkları Polikliniği,
Hopa, ARTVİN - TURKEY
e-mail: cakmakcidilek@yahoo.com