RESEARCH ARTICLE
Doi: 10.5578/tt.9411
Tuberk Toraks 2016;64(2):171-174

Mantar allerjisi olan bir olgu; Kounis sendromuna neden olan yeni bir etyolojik ajan
Fatma Merve TEPETAM1, Bahadır DAĞDEVİREN2, İsmet BULUT1, Can Y?cel KARABAY3, Safa BARIŞ4,
Elif AYDINER KARAKO?4
1 S?reyyapaşa G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, İmm?noloji ve Allerji Kliniği,
İstanbul, T?rkiye
1 Clinic of Immunology and Allergy, Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital,
Istanbul, Turkey
2 Medical Park G?ztepe Hastanesi, Kardiyoloji Kliniği, İstanbul, T?rkiye
2 Clinic of Cardiology, Medical Park Goztepe Hospital, Istanbul, Turkey
3 S?reyyapaşa G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, Kardiyoloji Kliniği, İstanbul, T?rkiye
3 Clinic of Cardiology, Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey
4 Marmara ?niversitesi Tıp Fak?ltesi, Pediatrik İmm?noloji ve Allerji Bilim dalı, İstanbul, T?rkiye
4 Department of Pediatric Immunology and Allergy, Faculty of Medicine, Marmara University, Istanbul, Turkey
?ZET
Mantar allerjisi olan bir olgu; Kounis sendromuna neden olan yeni bir etyolojik ajan
Kounis sendromu, anafilaktik reaksiyon bağlamında, akut miyokart infarkt?s? (AMİ) olduğunda, her zaman akılda tutulması gereken, nadiren tanı konulan bir durumdur. Bizim rapor ettiğimiz olgu; 31 yaşında kadın hasta, mantar (Pleurotus Ostreatus) yedikten iki saat sonra bulantı, karın ağrısı, kusma, nefes darlığı ve g?ğ?s ağrısı tarif ediyordu. EKG'de D1, AVL, prekordial V1-V4'e kadar uzanan ST segment elevasyonu vardı. Kan analizinde CK-MB ve troponin T d?zeylerinde y?kseklik mevcuttu. Laboratuvar kateterizasyonunda intrakoroner nitrat tedavisi sonrası elektrokardiyografik değişikliklerle beraber anjinanın tamamen kaybolması ve mantarla prick to prick testin pozitif ?ıkmasıyla Kounis tanısı konuldu. Bizim bildiğimiz kadarıyla bu olgu Pleurotus Ostreatus allerjisi nedeniyle gelişen rapor edilmiş ilk tip 1 varyant Kounis sendromu olgusudur.
Anahtar kelimeler: Anafilaksi, koroner hipersensitivite bozukluğu, Kounis sendromu, mantar allerjisi, miyokart infarkt?s?
SUMMARY
A patient with mushroom allergy; a new etiological agent of Kounis syndrome
Kounis syndrome (KS) is a rarely diagnosed condition which should always be kept in mind when an acute myocardial infarction (AMI) happens in the context of anaphylactic reactions. We report a case of a 31-year old female; 2 hours after the ingestion of the mushroom (Pleurotus ostreatus); she experienced nausea, stomachache, vomiting, dyspnea and chest pain. Electrocardiogram (ECG) showed an ST segment elevation in D1, AVL, precordial leads V1-V4. The blood analysis revealed high levels of CK-MB fraction and troponin T values. The diagnosis of Kounis syndrome was made in the catheterization laboratory via the complete resolution of angina, along with electrocardiographic changes that took place after intracoronary nitrate therapy and skin prick to prick test positivism with the mushroom. To the best of our knowledge, this is the first case of a type I variant of Kounis syndrome due to Pleurotus ostreatus allergy reported so far.
Key words: Anaphylaxis, coronary hypersensitivity disorder, kounis syndrome, mushroom allergy, myocardial ischaemia/infarction.
Introduction
Pleurotus ostreatus, the oyster mushroom, is a common edible mushroom. It was first cultivated in Germany as a subsistence measure during World War and is now grown commercially around the world for food (1). It contains statins such as lovastatin which work to reduce cholesterol and benzaldehyde which is an aromatic aldehyde used in cosmetics as a denaturant (2,3). Moreover a fibrinolytic enzyme was produced by the mushroom applied as a natural agent for oral fibrinolytic therapy or prevention of thorombosis (4). Kounis syndrome (KS) is a rarely diagnosed condition which should always be kept in mind when an acute myocardial infarction (AMI) happens in the context of anaphylactic reactions, with or without clinical history of atopy or allergy (5).
Several causes have been described to induce Kounis syndrome, and their number is increasing rapidly. These causes include various drugs, chemicals, foreign bodies, environmental exposures or some other conditions that give rise to inflammatory mediator release (6,7,8,9,10,11). Pleurotus Ostreatus spores are known as inhalation allergens and contact allergens that cause allergic reactions like bronchial asthma, and contact dermatitis (12,13). There has been no report describing food anaphylaxis or anaphylactoid reaction caused by the Pleurotus ostreatus, but a small number of reports suggest that matsutake mushroom can induce anaphylaxis on rare occasions (14,15). However there is not any report with kounis syndrome due to any mushroom allergy.
Case Report
Herein, we report a case of a 31-year old female wih history of giving birth a child before 1 mounth ago, with? no cardiovascular risk factors (smoker, diabetes mellitus, and dyslipidemia), and no medical history of atopic diseases (Asthma, allergic rhinitis, athopic dermatitis, urticaria).? She ate a mushroom (Pleurotus ostreatus) and 2 hours after the ingestion of the mushroom she experienced, nausea, stomachache, vomiting. She told us an episode of the same mushroom-induced anaphylaxis (nausea, stomachache, vomiting and dyspnea) that had occurred approximately 15 years before. She said that other mushrooms had never induced allergic reactions. She was transferred to the emergency room in 15 min, where dyspnea and chest pain appeared together with the former symptoms. Blood pressure and heart rate were 100/70 mmHg and 107 beats/min respectively. Physical examination was completely normal. Electrocardiogram (ECG) showed an ST segment elevation in D1, AVL, precordial leads V1-V4. The blood analysis revealed CK-MB fraction of 291.6 ng/mL (normal= 0-5), and troponin T value of 5042.0 pg/mL (normal= 0-14). The serum tryptase level was not determined at the time. The transthoracic echocardiography revealed left ventricul segmental wall motion abnormality, as well as, a moderate global systolic dysfunction, she was immediately transferred for coronary angiography revealed that the right and circumflex coronary arteries were normal, but there was a diffuse narrowing in the proximal segment of the LAD (Figure 1). The diagnosis of Kounis syndrome was made in the catheterization laboratory via the complete resolution of the angina along with electrocardiographic changes that took place after intracoronary nitrate therapy. Calcium channel blockers and intravenous glycerol trinitrate were administered when she was hospitalized in the coronary care unit.

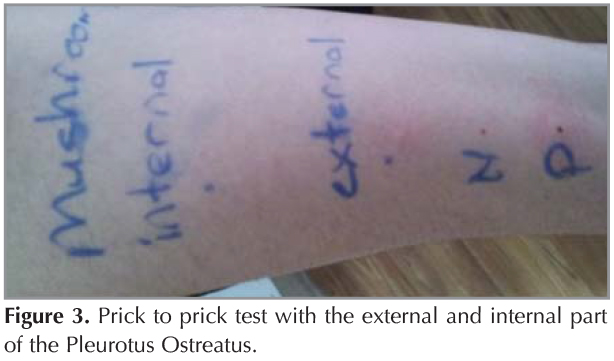
The patient was followed up for three mounths after discharge and the treatment of isosorbide dinitrate 60 mg and perindopril 10 mg were given to the patient.? She did not complain any symptoms of angina pectoris or heart failure. She was admitted to the endokrinology, rhomatology, hematology and coronary care unit for further tests because history of giving birth child before 1 mounth ago. Hormon analyzes; T3, T4, TSH, FSH, LH, Estradiol, prolactin, progesteron, total testesteron were normal, prothrombotic risk factors; natural coagulation inhibitors (antithrombin, protein C, protein S), blood coagulation factors (FV Leiden and FII 20210), homocysteine, lipid and lipoprotein profile (lipoprotein (a), triglycerides, total, high- and low-density lipoprotein), and antiphospholipid antibodies (lupus anticoagulant, anticardiolipin IgG, IgM, ,anti beta2 glikoprotein IgG) were normal, Influenza, adenovirus, RSV virus antigen, HBs Ag, anti HCV, C3, C4? were normal too. Three months later, she visited our allergy outpatient-clinic, allergic etiology of the cardiac event was considered in view of the detailed clinical history and relationship with ingestion the mushroom Pleurotus.ostreatus (Figure 2). A skin-prick-testing battery of indoor, outdoor and food allergens; not including mushroom; was performed. All the test results were negative but Pleurotus ostreatus (external part) prick to prick test was positive which produced a wheal of 5 mm after 20 min and increased wheal of 15 mm after 8 hour but matsutake mushroom produced no reaction, thus confirming Pleurotus ostreatus hypersensitivity (Figure 3). The analytical data showed a serum total IgE of 52.9 IU/mL (normal: < 100 IU/mL), baseline serum tryptase of 3.8 ?g/L (normal: < 11.4 ?g/L). Control electrocardiography demonstrated the complete resolution of the ST elevation. The troponin-T levels were 18.33 ng/mL? (normal: 0-14 ng/mL). CK-MB levels were 1.90 ng/mL (normal: 0-5). Echocardiography was performed and showed mild mitral regurgitation and grade I diastolic dysfunction without segmental wall motion abnormality. These findings confirmed the diagnosis of acute myocardial infarction associated with vasospastic angina in connection with Kounis syndrome.

Kounis syndrome has been reported in association with a mutation in E148q, the gene of familial Mediterranean fever (MEFV) (16). When we investigate our patients famial history, her mother was died because of possibly MI when she was 45 years old; so we analized the gen mutation; The result was V726A heterozigot mutation.
Discussion
According to recent data, two variants of Kounis syndrome have been described by Nikolaidis et al (17). The type I variant pertains to normal coronary arteries without predisposing factors, and their underlying mechanism is endothelial dysfunction. The type II variant is associated with patients with preexisting atheromatous disease for whom the acute release of inflammatory mediators can cause coronary artery spasms. In light of recently published papers, Biteker has also proposed a type III variant that includes patients with stent thrombosis (18). Our patient was diagnosed as type I Kounis syndrome in which myocardial ischemia or infarction occurs in normal coronary arteries due to coronary artery spasm.
Main pathophysiological mechanism is vasospasm of epicardial coronary arteries due to increased inflammatory mediators such as histamine, neutral proteases, arachidonic acid products, platelet-activating factor (PAF), and a variety of cytokines and chemokines that are released during a hypersensitivity and anaphylactic or anaphylactoid reaction (19,20,21). Clinical and experimental findings show that there is a common pathway between allergic and non allergic coronary events, because the same mediators from the same cells are present in both hypersensitivity episodes and acute coronary syndromes (22).
To the best of our knowledge, this is the first case of a type I variant of Kounis syndrome due to Pleurotus ostreatus allergy reported so far. The pathogenesis of the resulting coronary artery spasm is unclear. We considered a positive reaction against P. Ostreatus but not matsutake mushroom in skin prick to prick test, this case as anaphylaxis to Pleurotus ostreatus. But the specific IgE antibody was not detected however a few groups have extracted and purified the antigens from Pleurotus and detected the specific IgE or IgG antibodies in sera from patients with extrinsic allergic alveolitis although it is too complicated and time-consuming (12). The detected V726A heterozigot mutation support the report of Kounis syndrome association with a mutation in E148q the gene of familial Mediterranean fever (MEFV) (16).
We remark the importance of keeping? accompanied by preceding allergic or anaphylactic symptoms along with the ingestion of the mushroom, it is important to note that allergy to mushroom can be induced several hours after its ingestion. Because of the potentially atypical clinical presentations of acute coronary syndromes, either the ECG or serum tryptase assay is a mandatory diagnostic tool in any anaphylactic reaction. Physicians should be aware of this complication of anaphylaxis in order to diagnose it early and treat it properly.
REFERENCES
- Eger G, Eden G, Wissig E. Pleurotus ostreatus breeding potential of a new cultivated mushroom. Theor Appl Genet 1976;47:155-63.
- Gunde-Cimerman N, Cimerman A. Pleurotus fruiting bodies contain the inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A reductase-lovastatin. Exp Mycol 1995;19:1-6.
- Beltran-Garcia MJ, Estarron-Espinosa M, Ogura T. Volatile compounds secreted by the oyster mushroom (Pleurotus Ostreatus) and their antibacterial activites. J Agric Food Chem 1997;45:4049.
- Liu XL, Zheng XQ, Qian PZ, Kopparapu NK, Deng YP, Nonaka M, et al. Purification and characterization of a novel fibrinolytic enzyme from culture supernatant of Pleurotus ostreatus. J Microbiol Biotechnol 2014;24:245-53.
- Molina P, Presentaci?n C, Beltr?n P, Zorio E. Kounis syndrome: a possibility to be considered as a cause of sudden cardiac death. Cuad Med Forense 2012;18:35-8.
- Ilhan E, G?ven? TS, Poyraz E, Ayhan E, Soylu O. Kounis syndrome secondary to cefuroxime axetil use in an asthmatic patient. Int J Cardiol 2009;137:67-9.
- Aykan AC, Zehir R, Karabay CY, Ozkan M. A case of Kounis syndrome presented with sudden cardiac death? Anadolu Kardiyol Derg 2012;12:599-600.
- Kogias JS, Papadakis EX, Tsatiris CG, Hahalis G, Kounis GN, Mazarakis A, et al. Kounis syndrome: a manifestation of drug-eluting stent thrombosis associated with allergic reaction to contrast material. Int J Cardiol 2010;4:139:206-9.
- Venturini E, Magni L, Kounis NG. Drug eluting stent-induced Kounis syndrome. Int J Cardiol 2011:7;146:16-9.
- Kogias JS, Sideris SK, Anifadis SK. Kounis syndrome associated with hypersensitivity to hymenoptera stings. Int J Cardiol 2007;114:252-5.
- Nikolaidis LA, Kounis NG, Gradman AH. Allergic angina and allergic myocardial infarction: a new twist on an old syndrome. Can J Cardiol 2002;18:508-11.
- Cox A, Folgering HTM, Van Griensven LJLD. Extrinsic allergic alveolitis caused by spores of the oyster mushroom Pleurotus osteatus. Eur Respir J 1988;1:466-8.
- Rosina P, Chieregato C, Schena D. Allergic contact dermatitis from Pleurotus mushroom. Contact Dermatitis 1995;33:277-8.
- Toda T, Yamaguchi M, Nakase Y, Sugimoto N, Suzukawa M, Nagase H, et al. A case of anaphylactic reaction following matsutake mushroom ingestion: Demostration of histamine release reaction of basophils. Allergol Int 2010;59:417-9.
- Ichikawa K, Ito R, Kobayashi Y, Aihara M, Osuna H, Aihara Y. A pediatric case of anaphylaxis caused by matsutake mushroom (Tricholoma matsutake) ingestion. Allergol Int 2006;55:85-8.
- Nicholas NG. Coronary hypersensitivity disorder: the Kounis syndrome. Clin Ther 2013;35:563-71.
- Nikolaidis LA, Kounis NG, Gradman AH. Allergic angina and allergic myocardial infarction: a new twist on an old syndrome. Can J Cardiol 2002;18:508-11.
- Biteker M. A new classification of Kounis syndrome. Int J Cardiol 2010;145:553.
- Karabay CY, Can MM, Tanboga IH, Ahmet G, Bitigen A, Serebruany V. Recurrent acute stent thrombosis due to allergic reaction secondary to clopidogrel therapy. Am J Ther 2011;18:e119-22.
- Kounis NG, Mazarakis A, Tsigkas G, Giannopoulos S, Goudevenos J. Kounis syndrome: a new twist on an old disease. Future Cardiol 2011;7:805-24.
- Kounis NG, Giannopoulos S, Tsigkas GG, Goudevenos J. Eosinophilic responses to stent implantation and the risk of Kounis hypersensitivity associated coronary syndrome. Int J Cardiol 2012;19:156:125-32.
- Kounis NG, Hahalis G, Manola A, Kourelis T, Theoharides TC. Kounis Syndrome (Allergic angina and allergic myocardial infarction) In: Gallo AP, Jones ML (eds). Angina pectoris: etiology, pathogenesis and treatment. Nova Science Publishers, 2008;77-150.
Yazışma Adresi (Address for Correspondence)
Dr. Fatma Merve TEPETAM
S?reyyapaşa G?ğ?s Hastalıkları ve
G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi,
İmm?noloji ve Allerji Kliniği,
İSTANBUL - TURKEY
e-mail: fatmamervealan@hotmail.com