RESEARCH ARTICLE
Doi: 10.5578/tt.10916
Tuberk Toraks 2016;64(2):127-136

Ankara ili diş teknisyenlerinde pn?mokonyozlu olgularda hastalığın
radyolojik yaygınlığı ve solunum fonksiyonları arasındaki ilişki
Dilek ERG?N1, Recai ERG?N2, Ender EVCİK3, T?rkan NADİR ?ZİŞ1, İbrahim AKKURT4
1 Ankara Meslek Hastalıkları Hastanesi, G?ğ?s Hastalıkları Kliniği, Ankara, T?rkiye
1 Clinic of Chest Diseases, Ankara Occupational Diseases Hospital, Ankara, Turkey
2 Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği, Ankara, T?rkiye
2 Clinic of Chest Diseases Diskapi Yildirim Beyazit Training and Research Hospital, Ankara, Turkey
3 Ankara Meslek Hastalıkları Hastanesi, Radyoloji Kliniği, Ankara, T?rkiye
3 Clinic of Radiology, Ankara Occupational Diseases Hospital, Ankara, Turkey
4 ?zel Akay Hastanesi, G?ğ?s Hastalıkları ve Meslek Hastalıkları Kliniği, Ankara, T?rkiye
4 Clinic of Chest Diseases and Occupational Diseases, Special Akay Hospital, Ankara, Turkey
?ZET
Ankara ili diş teknisyenlerinde pn?mokonyozlu olgularda hastalığın radyolojik yaygınlığı ve solunum fonksiyonları arasındaki ilişki
Giriş: Diş teknisyenlerinde tozun neden olduğu parankimal değişiklikler pulmoner fonksiyonları etkiler. Diş teknisyenlerinde pulmoner tutulumun derecesini g?steren radyolojik skorlar (Akciğer grafiği/YRBT) ile fonksiyonel bulguların etkilenme derecesi arasındaki ilişkiyi değerlendirmek.
Materyal ve Metod: 440 diş teknisyeni akciğer grafiği, solunum fonksiyon testleri, y?ksek ??z?n?rl?kl? bilgisayarlı tomografi (YRBT) ile değerlendirildi. Radyolojik g?r?nt?lerdeki pulmoner tutulum derecesi; opasitelerin yoğunluğu, amfizem, buzlu cam, bal peteği, plevral anormalliklerin genişliği temel alınarak kategorize edildi.
Bulgular: ?alışma pop?lasyonunun ortalama yaşı 34.7 ? 8.5 idi ve ortalama ?alışma s?resi 16.5 ? 7.9 yıl idi. Diş teknisyeni pn?mokonyozu (DTP) prevalansı %11.1 idi. YRBT'de en yaygın opasite %89.7 ile round opasite idi. B?y?k opasite oranı ise %14.3 idi. ILO (International Labor Organization) skoru ve YRBT skoru arasında pozitif korelasyon vardı. ILO ve YRBT skorları ile t?m pulmoner foksiyon testleri (FEV1/FVC dışında) arasında negatif korelasyon saptanırken, yaş, total maruziyet s?resi, sigara, işe başlama yaşı arasında bir ilişki saptanmadı. Multiple regresyon analizinde; pulmoner tutulumun derecesi (YRBT skor) fonksiyonel bozukluğun bağımsız belirleyicisi olmuştur. Pulmoner tutulumun derecesini en iyi yansıtan fonksiyonel parametre ise %FEV1 idi.
Sonu?: Biz diş teknisyenlerinde miks toz maruziyeti ile ilişkili fonksiyonel bozuklukların g?sterilmesinde radyolojik ve fonksiyonel ?l??mlerin birlikte kullanılması gerektiğini d?ş?n?yoruz.
Anahtar kelimeler: Pn?mokonyoz, diş teknisyeni, mesleki akciğer hastalığı
SUMMARY
The relation between the extent of radiological findings and respiratory functions in pneumoconiosis cases of dental technicians who are working in Ankara
Introduction: In dental technicians, parenchymal changes caused by dust affect pulmonary functions. The evaluation of the relation between radiological scores (chest X-Ray/HRCT) indicating the extent of pulmonary involvement and the severity of functional findings in dental technicians.
Materials and Methods: 440 dental technicians were evaluated with chest X-Ray, pulmonary function tests (PFTs) and high resolution computed tomography (HRCT). The degree of pulmonary involvement in radiological images was categorized based upon emphysema, the profusion of opacities, ground-glass opacity, honey combing and extent of pleural abnormalities.
Results: Mean age of the study population was 34.7 ? 8.5 and mean duration of work was 16.5 ? 7.9 years. The prevalance of Dental technicians' pneumoconiosis (DTP) was 11.1%. The most common opacity in HRCT was round opacity with a rate of 89.7%. The rate of large opacity was %14.3. There was positive correlation between ILO score and HRCT score. Negative correlation was found between ILO and HRCT scores and all pulmonary function tests (except for FEV1/FVC), while no relation was found with age, overall duration of exposure, smoking and the age ofwork onset. In Multiple regression analysis, the extent of pulmonary involvement (HRCT scores) was found to be an independent predictor of functional impairment. Functional parameter reflecting the extent of pulmonary involvement most accurately was (FEV1%).
Conclusion: It is our suggestion that radiological measurement should be used along with functional measurements in the evaluation of functional impairment in mixed dust exposed dental technicians.
Key words: Pneumoconiosis, dental technicians, occupational lung diseases
INTRODUCTION
Dental laboratories harbor many dangers for dental technicians including physical, chemical, radioactive, ergonomic, psychological and biological ones. Dental technicians are constantly exposed to the vapor of different solvents and non organic acids, toxic gases formed during material use and to deleterious effects of dust formed during finishing, grinding and sandblasting of ceramic, acrylate and metal alloys (1,2,3). Pneumoconiosis, hypersensitivity pneumonia, occupational asthma and lung cancer may occur in dental technicians depending upon the duration of exposure (4).
Dental technicians' pneumoconiosis (DTP), is a disease presenting with interstitial inflammation and fibrosis occurring due to exposure to complex substances (5). Although clinical functional parameters are influenced minimally in the early period of the disease, impairment in clinical functional parameters becomes more marked with radiological progression (6). In the evaluation of the severity of the disease, the employment of radiological and functional indices becomes more important (7).
High resolution computerised tomography (HRCT) has an increasingly important role in the evaluation of occupational lung disease. HRCT is more sensitive than lung radiography in the detection of asbestosis, silicosis, pneumoconiosis and other parenchymal abnormalities in early period (8).
In the literature, there are studies demonstrating the relation between the degree of involvement detected with lung radiography or HRCT and functional loss in various occupational groups (9,10). Although there are many studies showing the clinical findings, radiological involvement and functional impairment in dental technicians; relation between the degree of radiological involvement and functional impairment has not been clarified (11,12,13). In the present study with a large case series, the presence of a relation between radiological findings (chest X-Ray/HRCT) and functional findings in all dental technicians residing in Ankara, Turkey was evaluated. As far as we know, there is no previous study in the literature evaluating the relation between the extent of pulmonary involvement in lung graphies and functional findings and comparing lung radiographies with HRCT in this respect. Therefore, we believe that this article will contribute to the literature on the issue.
MATERIALS and METHODS
In order to determine the effect of occupational exposure on dental technicians, overall 440 dental technicians employed in 175 dental prosthesis laboratories registered in Ankara Health Province directorate of health were examined in our hospital between January 2009-January 2010. Their data were evaluated retrospectively. None of the dental technicians had a history of exposure to dust in their previous occupations. Those with any pulmonary disease were excluded from the study. The present study was approved by ethics committee of Dışkapı Yıldırım Beyazıt Training and Investigation Hospital.
Demographic information, respiratory symptoms, smoking status, overall duration of work, physical examination findings, chest X-Ray, HRCT, and pulmonary function tests (PFTs) results were recorded in evaluation form.
Those who have not smoked for one year or longer were considered as ex smoker, those who smoke one or more cigarettes per day for at least one year as smoker and those who smoke less or never as nonsmoker.
Radiological Examination
Chest X-Rays were taken in the US X-Ray (500 milliAmpers) conventional radiography device, posteroanterior position with a short exposure time (0.1 second). To obtain the images computerised radiography (CR) technique was used in the Kodak Direct View Elite CR system and then the the images were printed in Kodak DryView 8900 Laser Imager. The hard copies were in 35 x 43 cm dimension.
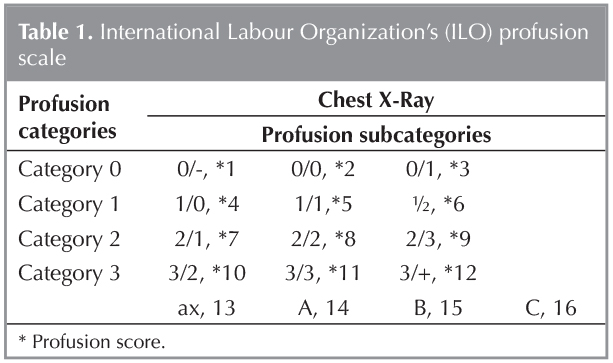
Chest X-Rays were evaluated by 2 respiratory diseases consultant and 1 radiologist (2 of them ILO B readers) according to International Labor Organization (ILO) 2000 criteria (14). When there was disagreement, lung radiographies were evaluated together by three readers. Those at ILO category 1/0 and over were evaluated as pneumoconiosis (15). Small opacities up to 1.5 mm were coded as "p", those between 1.5-3 mm as "q" and those between 3-10 mm as "r". Irregular opacities up to 1.5 mm thickness were coded as "s", those between 1.5-3 mm as "t", and those between 3-10 mm as "u". Large opacities were classified according to their largest dimension. Opacities with largest dimensions over 1 cm were classified as large opacity. If the number of these opacities was over one, the sum of largest dimensions of all was calculated. A opacity was: 1 cm-5 cm; B opacity: overall dimensions over 5 cm, but overall area occupied by one large opacity or multiple large opacities does not exceed overall right upper zone area. C opacity: overall area occupied by one large opacity or multiple large opacities exceeding right upper zone area. In order to evaluate small and large opacity profusion, 16 score ILO scale was used (Table 1) (16).
104 dental technicians with Chest X-Ray results suspicious for DTP underwent HRCT examination. HRCT images were interpreted in a randomized manner by a radiologist in a different session retrospectively (without seeing chest X-Rays). The HRCT scans were acquired using GE HiSpeed scanner (General Electric Medical Systems). Slices were obtained in 1 mm thickness, at 10 mm intervals from apex to the base of the lung. Image reconstruction technique was 512 x 512 pixel matrix with the use of a high resolution algorithm. The HRCT images were evaluated according to International Classification of HRCT for Occupational And Enviromental Respiratory Diseases Guidelines (17).
First of all, each lung (right and left) was divided into three zones. Upper zone was from apex to arch of aorta level. Middle zone was from arch of aorta to the inferior pulmonary veins. The scans caudal to the inferior pulmonary veins were considered as lower zone. Each zone was evaluated for the presence of small opacities, according to their shape as regular (round) and irregular (linear). Opacities were considered as small opacity if they had a diameter (for round opacity) or thickness (for linear opacity) less than 1 cm. If there was no opacity the point score was "0".
The point score of round opacities was noted as "1" if there were few micronodules and no erasing of vascular markings. Point score was "2" when there were many micronodules, with or without erasing of vascular markings, but there was no confluence of the nodules. The score was "3" when there was confluence of nodules as well the erasing of the vascular markings. Score 1 was evaluated as "mild", score 2 as "moderate" and score 3 as "severe".
The linear (irregular) opacities point scoring was made according to the number of opacities. Few numbers of linear opacity was scored as "1", moderate number was "2", many diffuse many linear opacities was "3" (severe). Normal anatomical lung structure was poorly visible in severe form.
Honeycomb pattern is the presence of small cysts which are surrounded by septations. This kind of pattern is seen at the periphery of the lung and signifies the end stage fibrosis. Honeycomb pattern scoring was made for each zone as; 1 (mild), if the thickness of lung parenchyma where this pattern is seen is up to 10 mm, 2 (moderate) if the thickness is between 10 mm and 30 mm, and 3 (severe) if the thickness of honeycomb pattern is more than 30 mm.
Ground glass opacity scoring was made according to pattern as focal (score 1), patchy (score 2), and diffuse (score 3).
Emphysema scoring was made for each zone. The score was "1" when the total area of the emphysema and the bullae of that zone occupies up to 15 % of the zone. When the total area of emphysematous region is between 15% and 30% of that zone, the score is "2". When it is more than 30%, the score is "3". Grading of scores are mild "point 1", moderate"point 2", and severe "point 3".
For the grading of large opacities; the opacities with the largest dimension more than 1 cm are considered and the HRCT slice of right lung at the carina level was evaluated. Large opacities; A: The sum of the opacities having the largest dimension(s) more than 1cm is up to 1/4 of the area (quadrant)of the right lung at the carina level. B: When the total area of opacities is between ? and ? of right lung at carina level. C: when the total area of opacity(s) exceeds ? of right lung. The scores were "1" for Large opacity A; "2" for Large opacity B, and "3" for Large opacity C.
For pleural scoring, again the right lung at the carina level was taken in consideration. All pleural thickening and calcifications of both lungs were added. But the diaphragmatic pleural thickenings were not measured. Extent was measured in terms of degrees of the circumference of 360?. If the total sum of the pleural thickening is up to 90? (< ?) the score is considered as "1"; when the total sum is between 90? and l80? (? - ?) the score is "2". Score "3" is when the sum exceeds 180? (> ?).
The sum of the whole scores obtained from each zone (round opacity, linear opacity, emphysema, honeycomb pattern, ground glass opacity; large opacity, pleural findings) was evaluated as total profusion score of HRCT.
Pulmonary Function Tests (PFTs)
Spirometer tests were carried out by spirometer technician by dry-seal-spirometer (Zan 100, nSpire Health Inc., Germany) according to American Thoracic Society (ATS) guidelines (18). Diffusing capacity of lung for carbon monoxide (DLCO) was measured by using the single-breath DLCO procedure (Zan 100, nSpire Health Inc., Oberthulba, Germany). In 38 patients in whom DTP was detected, DLCO was measured. 11 patients were not able to cooperate with the test.
Statistical Analysis
In the analysis of data, SPSS 21.0 for Windows program was used. Categorical variables were expressed in cross-tables and numerical variables in mean, median, standard deviation, minimum and maximum. In the comparison of independent categorical variables, Chi-square test was used. In multiple comparisons when the conditions of Chi-square were not met, Monte Carlo Simulation, in comparion of groups two by two Fisher's Exact test, in groups comparion of numerical variables, when the data were not distributed normally Mann-Whitney U test and in multiple groups comparisons in which the data were not distributed normally Kruskal-Wallis test was used. In the comparison of subgroups, Mann-Whitney U test with Bonferroni correction was used. Pearson's coefficient of correlation was used in order to evaluate the relation between functional parameters and radiological scores. In the investigation of the factors influencing respiratory functions, linear regression stepwise method was used. P value of < 0.05 was considered statisticallly significant.
RESULT
Overall 440 dental technicians (349 male, 91 female) at the mean age of 34.7 ? 8.5 were included in the study. Mean age of onset of work was 18.8 ? 5.2 and mean duration of work was 16.5 ? 7.9 years.
In Chest X-Rays, pneumoconiosis was detected in 49 out of 440 dental technicians (11.1%) according to ILO classification. The characteristics of dental technicians with pneumoconiosis and those without pneumoconiosis are shown in Table 2.
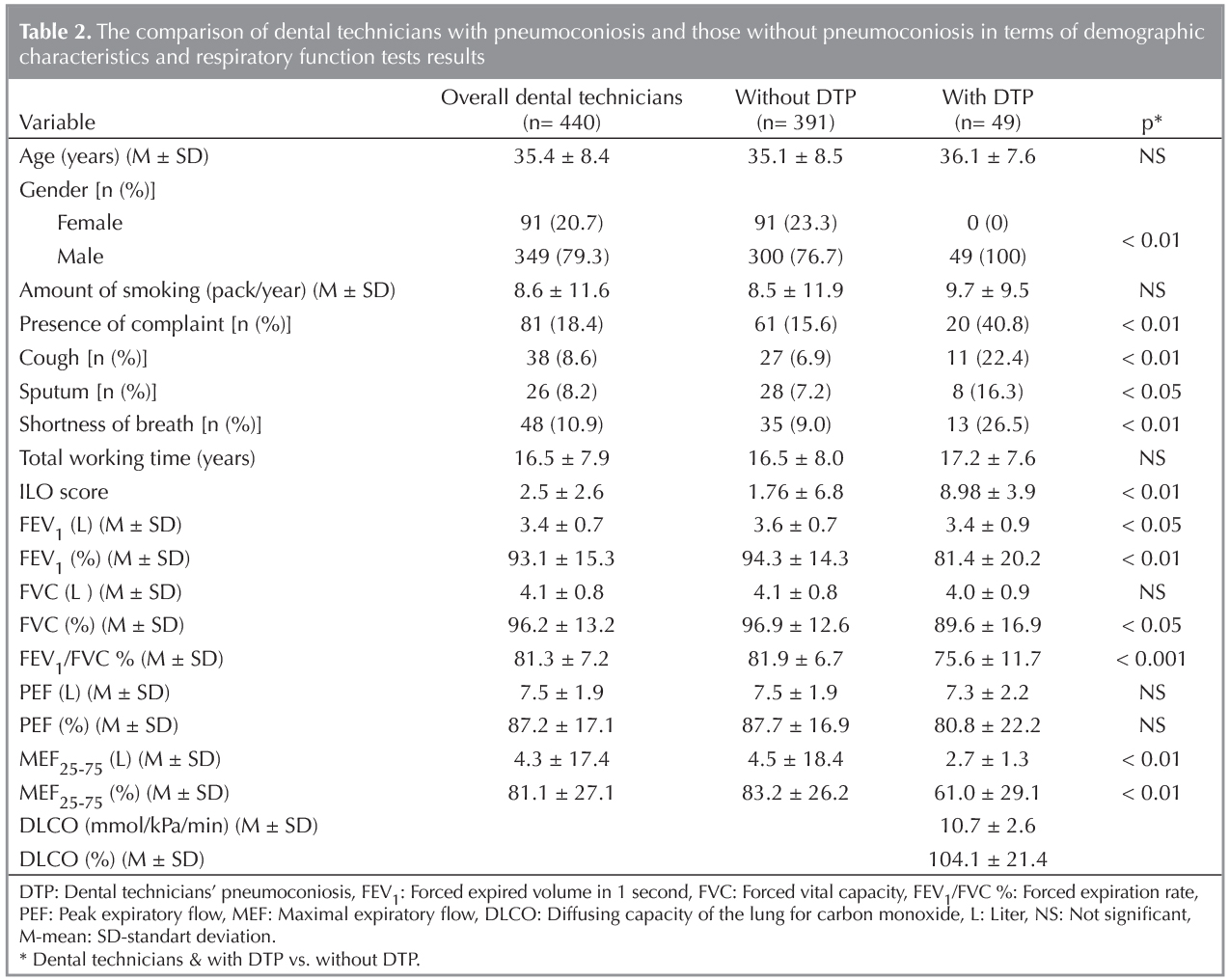
The rate of DTP was higher in males than that in females. There was no significant difference between dental technicians with DTP and those without it in terms of the rate of smoking, the amount of cigarettes consumed and overall duration of work. In those with DTP, respiratory complaints were more marked, with higher ILO scores.
In those with DTP, all PFTs other than FVC (L) and PEF (L, %) were significantly lower (Table 2).
There was positive correlation between ILO score and HRCT score. ILO and HRCT scores had negative correlation with all functional parameters ( except FEV1/FVC), while HRCT score was more closely correlated with functional impairment. No relation was found between ILO and HRCT scores and age, duration of work, age of onset of work and smoking status (Table 3).

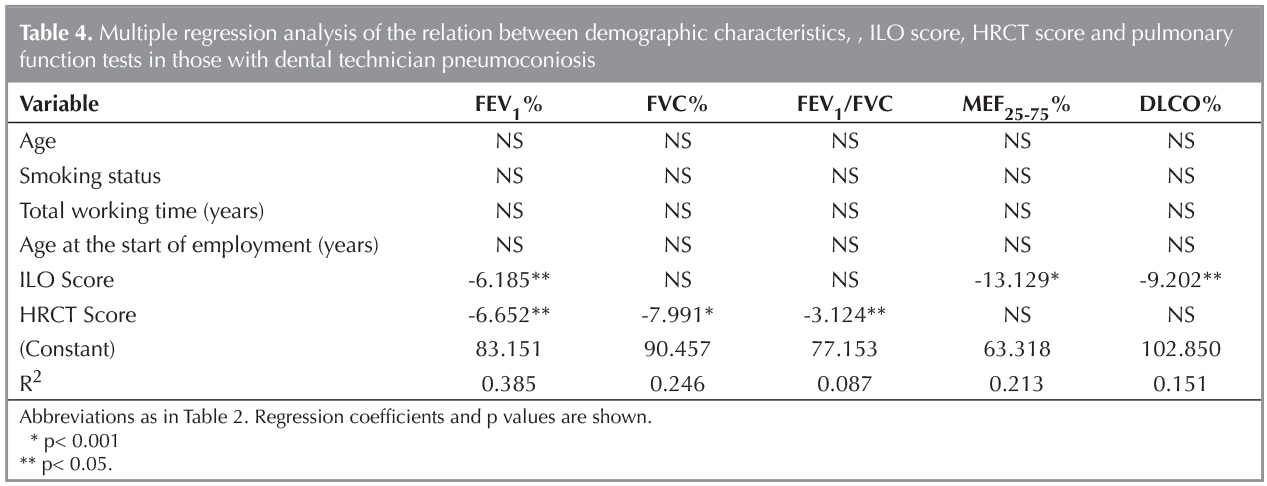
The effects of age, smoking status (non smokers versus smokers and ex smokers), overall duration of work, age of onset of work, and, ILO and HRCT scores on pulmonary function tests was investigated using multiple linear regression test. HRCT score was an independent predictor of FEV1%, FVC% and FEV1/FVC while ILO score was an independent predictor of FEV1%, MEF25-75% and DLCO%. Both HRCT score and ILO score were the best independent predictors of FEV1. The effect of age, overall duration of work, the age of onset of work on respiratory functions were not independent (Table 4).
Profusion category, shape and size of small opacities in lung graphies and ILO classification of large opacities is demonstrated in Table 5.
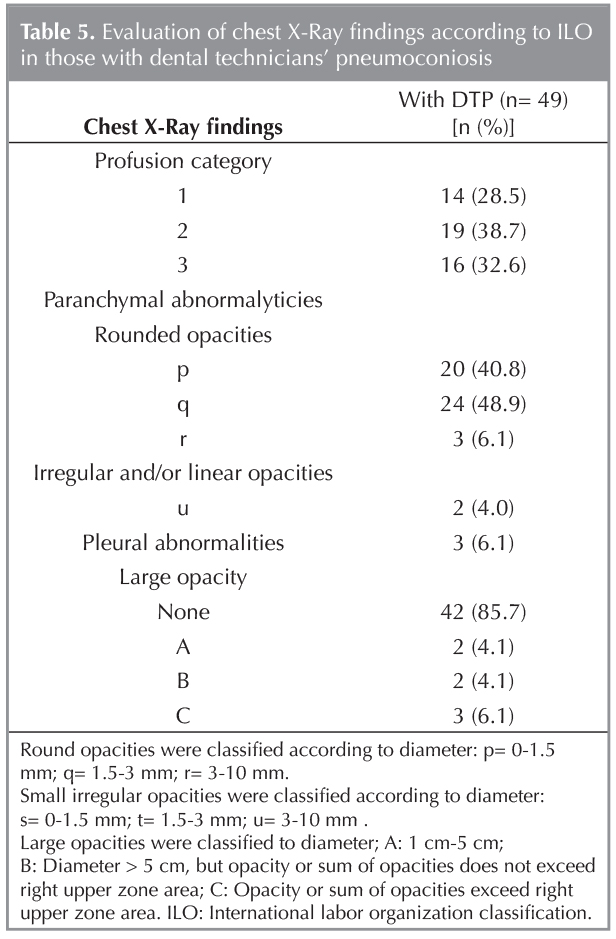
In HRCT, the most commonly detected opacities (89.7%) were round opacities and the rate of large opacity was 14.3%. HRCT according to ILO classification revealed pleural abnormality in 13 of 49 patients with DTP in lung radiography (26.5%), emphysema in 16 (32.7%), hilar enlargement in 14 (28.6%) dependent opacity in, 10 (20.4%), 9 (18.4%) coalesence of small opacities in, and additional pathologies such as eggshell calcification and honey combing in 2 (4.1%) (Table 6).

Discussion
Dental technician pneumoconiosis is a form interstitial lung disease developing as a result of occupational exposure. The prevalence of pneumoconiosis has been reported to vary between 4.5% and 43% in dental technicians (2,19,20). Such a wide range of variation in rates of pneumoconiosis may be due to differences in work conditions and environments of dental technicians, size of study population and methodology used in studies. In the study of Choudat et al on 105 freelance dental technicians at the ages of 43-66 in Paris, the prevalance of small opacity over 1/0 according to ILO classification was found to be 11.8%. The prevalence of pneumoconiosis was found to be 3.5% in technicians working less than 30 years, while it was 22.2% in those working for more than 30 years (2). In the study of Sherson et al. in which 31 dental technicians with a mean duration of exposure around 20 years, the rate of DTP was found to be 12.9% (39-61 years age range; mean age 42) (20). In our large series consisting of young dental technicians with low overall duration of work (mean duration, 16.5 years) (mean age, 35.4 years) (n= 49/440), the rate of pneumoconiosis prevalence was 11.1%.
Different results have been reported in the literature regarding the factors influencing the development of pneumoconiosis. In a study in Iran evaluating 42 dental technicians, significant relation was found between duration of work and interstitial opacity (21). In studies by Sherson et al. and Froudarakis et al. , in subjects with mean duration of work around 19-20 years the prevalence of pneumoconiosis were found to be respectively 12.9% and 9.8% (20,22). In the study of Berk et al with 32 dental technicians, positive correlation was found between age, duration of work, smoking status and profusion scores (23). In the study of Ooi et al on 76 silicosis cases, neither duration of exposure to silica nor smoking was associated with ILO and HRCT scores (24). In the present study, no significant relation was found between overall duration of work and smoking and radiological scores (both ILO score and, HRCT total score).
Many studies have been carried out concerning the presence of respiratory system complaints in dental technicians (2,19,20,22). In the study of Radi et al., it was stated that cough and sputum is an important risk in dental technicians (19). In the study of Frodorakis, significant difference was found in respiratory symptoms between dental technicians and control group, while in the study of Sherson et al., no significant difference was found in terms of symptoms, although the rate of dyspnea was higher in the group of dental technicians (20,22). In the study of Choudat et al. no difference was found between dental technicians and control group with regard to respiratory symptoms (2). However, Dogan et al. found the rate of dyspnea to be higher in dental technicians with pneumoconiosis (23). In the present study, respiratory complaints were present in 18.4% of dental technicians while in those diagnosed radiologically with DTP, this figure was 40.8%, being 15.6% in cases not so diagnosed. Respiratory system symptoms (cough sputum, shortness of breath ) were significantly higher in those with DTP than those without it. Symptoms were found in 34 (21%) of non smokers.
In early stage pneumoconiosis, PFTs may not display any abnormality. With radiological progression, obstructive, restrictive or mixed abnormalities may develop (25). Although there are studies showing that lung functions are slightly lower among dental technicians than the control group, there are also studies demonstrating no statistically significant difference in spirometric values (2,5,20,22). In the present study, there was significant difference between those diagnosed with DTP radiologically and those who were not diagnosed with it, with regard to all respiratory function test parameters (except FVCL, PEFL, PEF%).
HRCT contributes significantly to lung radiography in demonstrating early parenchymal changes and the extent of these changes in the diagnostic process of pneumoconiosis (26). To the best of our knowledge, there are few studies in the involving large case series utilizing HRCT in the diagnosis of pneumoconiosis in this specific group (11,26). In a study evaluating 76 dental technicians with HRCT, the most common finding was round opacity with a rate of 38% followed by pleural abnormalities (11%) and linear opacities (9%) (11). In another study in which 32 dental technicians were evaluated, rounded opacities were seen in 56% (47% p, 9% q) and linear opacities in 50%. In addition, findings such as pleural abnormalities, bronchiectasia, ground glass opacities, dependent opacities, hilar enlargement and bronchial wall thickening were also reported (23). In the study where the dental technicians were evaluated according to clinical and radiological findings, HRCT scans have been obtained in 58 patients having a suspicious pneumoconiosis radiographically and in 10 patients (%6) pneumoconiosis have been found (13). However, large opacity was not found in either of these studies. In the present study, the most common finding in those having DTP detected with HRCT was round opacity with a rate of 89.8%. The rate of large opacity was 14.3%. The detection of large opacities at a higher rate may suggest that our cases were exposed to silica or other dusts more intensively. In addition, in 49 patients with DTP in lung radiography according to ILO classification, it was established with HRCT that 13 (26.5%) had pleural abnormality, 16 (32.7%) emphysema, 14 (28.6%) hilar enlargement, 10 (20.4%) dependent opacity, 9 (18.4%) coalescence of small opacities, and 2 (4.1%) additional pathologies such as eggshell calcification and honeycombing.
There are no studies demonstrating radiological and functional correlation in dental technicians except for small case series. ILO scoring system is a valid method for detection of parenchymal involvement in pneumoconiosis in plain lung graphies and is used frequently for clinical and epidemiological studies (16). In previous studies, correlation between ILO score and pulmonary function abnormalities was demonstrated in those exposed to asbestos (9,27,28). Restrictive pulmonary changes (reduced TLC, FVC, and DLCO) correlated positively with the degree of parenchymal involvement shown in CXR (28). In 5003 workers exposed to asbestos, the severity of radiography was evaluated with ILO scores and relation was found beeen ILO scores and both independent functional parameters (FVC and DLCO). Both measurements decreased more markedly in high scores compared to low scores, indicating the consistency between radiographic and functional evaluation (9).
In a study evaluating 68 patients with cryptogenic fibrosing alveolitis using HRCT, close correlation was found between the extent of pulmonary involvement in tomography and pulmonary functions. It was also reported that especially additional pathologies such as emphysema contributed significantly to functional impairment and that the disease severity detected with HRCT was closely related to DLCO (7). In another study in which only radiological opacity of 32 dental technicians was evaluated, negative correlation was found between ILO and HRCT scores and spirometry findings, and close correlation between ILO and HRCT scores was demonstrated (23). In a study in which 76 male patients with silicosis were evaluated with lung graphy and HRCT, linear relationship was demonstrated between HRCT and lung functions. It was also established that nodules, large opacity and emphysema extent detected by HRCT, had a considerable contribution to impairment in pulmonary functions. In addition, HRCT scores had a more significant correlation with functional parameters than did ILO scores (24).
In the study of Lopes et al., correlation between tomographic parameters and functional parameters were investigated in 44 silicosis cases without history of tuberculosis. Negative correlation was found between total HRCT score including parenchymal opacity, emphysema, large opacity and other parenchymal changes and FEV1, FVC, FEV1/ FVC, DLCO. It was established that there was correlation between increase in damage detected with HRCT and decrease in air flow. Therefore, it was stressed that the degree of parenhymal involvement is an important indicator of the severity of functional impairment (26).
In the present study, there was close correlation between lung radiography (ILO score ) and extent of parenchymal involvement in HRCT (HRCT score) and functional parameters. This relation was more marked in HRCT. HRCT score reflected present functional impairment more accurately as it also demonstrated additional parenchymal pathologies such as emphysema, ground-glass opacity, honey combing and pleural abnormalities in addition to parenchymal opacity. Functional loss increased with radiological progression. The functional parameter mirroring the degree of pulmonary involvement most accurately was (FEV1%). In view of these data, it is our belief that HRCT has increasingly become more important in the evaluation of functional impairment caused by mixed dust exposure in dental technicians.
The present study has some limitations. HRCT was carried out only in dental technicians with suspicious lung graphies. If all dental technicians underwent HRCT, evaluations could be made in more detail. Another limitation was that agreement between readers could not be evaluated since all HRCT were evaluated by a single radiologist. The other limitations of our study was that there was no pneumoconiosis cases among the women patients. As we had informed in our previous study, especially being a male and sandblasting increase pneumoconiosis risk. Because there were few women who were sandblasting in this study, there were no pneumoconiosis observed among women technicians.? However, as far as we know, the present study is the first one comparing the relation between functional impairment and degree of involvement both in lung radiography and HRCT in a specific group such as dental technicians.
In conclusion, in the present study having a large case series, the prevalance of DTP in our region was found to be 11.1%. There is positive correlation between the degree of radiological involvement and functional loss in dental technician pneumoconiosis. The extent of involvement and its functional effects are demonstrated more clearly by HRCT. The functional parameter reflecting the degree of pulmonary involvement best was (FEV1%) . It is our suggestion that radiological (chest X-Ray/HRCT) and functional (PFTs) findings should be used in combination in the evaluation of occupational exposure in dental technicians.
REFERENCES
- Sivakumar I, Arunachalam KS, Solomon EGR. Occupational heallth hazards in prosthodontic practice: review of risk factors and management strategies. J Adv Prosthodont 2012;4:259-65.
- Choudat D. Occupational lung disease among dental technicians. Tuber Lung Dis 1994;75:99-104.
- Selden AI, Persson B, Bornberger-Dankvardt SI, Winstr?m LE, Bodin LS. Exposure to cobalt chromium dust and lung disorders in dental technicians. Thorax 1995;50:769-72.
- Thorette C, Grigoriu B, Canut E, Sobaszek A, Tonnel AB, Tillie-Leblond I. Pulmonary disease in dental laboratory technicians. Rev Mal Respir 2006;23(Suppl 2):4S7-4S16.
- Torbica N, Krstev S. World at work: Dental laboratory technicians. Occup Environ Med 2006;63:145-8.
- Rom WN. Role of oxidants in interstitial lung diseases: pneumoconioses, constrictive bronchiolitis, and chronic tropical pulmonary eosinophilia. Mediators In?amm 2011;2011:407657.
- Wells AU, King AD, Rubens MB, Cramer D, du Bois RM, Hansell DM. Lone cryptogenic fibrosing alveolitis: a functional-morphologic correlation based on extent of disease on thin-section computed tomography. Am J Respir Crit Care Med 1997;155:1367-75.
- Akira M. High-resolution CT in the evaluation of occupational and environmental disease Radiol Clin North Am 2002;40: 43-59.
- Miller A, Warshaw R, Nezamis J. Diffusing capacity and forced vital capacity in 5.003 asbestos-exposed workers: relationships to interstitial fibrosis (ILO profusion score) and pleural thickening. Am J Ind Med. 2013;56:1383-93.
- Wells AU, Hansell DM, Rubens MB, King AD, Cramer D, Black CM, et al. Fibrosing alveolitis in systemic sclerosis: indices of lung function in relation to extent of disease on computed tomography. Arthritis Rheum 1997;40:1229-36.
- Kahraman H, Koksal N, Cinkara M, Ozkan F, Sucakli MH, Ekerbicer H. Pneumoconiosis in dental technicians: HRCT and pulmonary function findings. Occup Med (Lond) 2014;64:442-7.
- Erg?n D, Erg?n R, Ozdemir C, Oziş TN, Yilmaz H, Akkurt I. Pneumoconiosis and respiratory problems in dental laboratory technicians: analysis of 893 dental technicians. Int J Occup Med Environ Health 2014;27:785-96.
- Yurdasal B, Bozkurt N, Bozkurt Aİ, Yilmaz ?. The evaluation of the dust-related occupational respiratory disorders of dental laboratory technicians working in Denizli Province. Ann Thorac Med 2015;10:249-55.
- International Labour Office (ILO): Guidelines for the use of the ILO International Classification of Radiographs of Pneumoconioses. Occupational Safety and Health Series No. 22 (Rev 2000) Geneva: p.1-38.
- Muir DC, Bernholz CD, Morgan WK, Roos JO, Chan J, Maehle W, et al. Classification of chest radiographs for pneumoconiosis: a comparison of two methods of reading. Br J Ind Med 1992;49:869-71.
- Guidelines for the use of the ILO International Classification of Radiographs of Pneumoconioses. Revised Edition. ILO occupational safety and health series. No. 22 (rev 80). Geneva 1980.
- Hering K, Kraus T. Coding CT-classification in occupational and environmental respiratory disease. In: Kusaka Y, Hering K, Parker J (eds). International classification of HRCT for occupational and environmental respiratory diseases. Tokyo, Japan, Springer 2005:15-23.
- Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J 2005;26:319-38.
- Radi S, Dalphin JC, Manzoni P, Pernet D, Leboube MP, Viel JF. Respiratory morbidity in a population of French dental technicians. Occup Environ Med 2002;59:398-404.
- Sherson D, Maltbaek N, Olsen O. Small opacities among dental laboratory technicians in Copenhagen. Br J Ind Med 1988;45:320-4.
- Alavi A, Shakiba M, Nejad AT, Massahnia S, Shiari A. Respiratory findings in dental laboratory technicians in Rasht (North of Iran). Tanaffos 2011;10:44-9.
- Froudarakis ME, Voloudaki A, Bouros D, Drakonakis G, Hatzakis K, Siafakas NM. Pneumoconiosis among cretan dental technicians. Respiration 1999;66:338-42.
- Berk S, Dogan DO, Gumus C, Akkurt I. Relationship between radiological (X-ray/HRCT), spirometric and clinical findings in dental technicians' pneumoconiosis. Clin Respir J 2016;10:67-73.
- Ooi GC, Tsang KW, Cheung TF, Khong PL, Ho IW, Ip MS, et al. Silicosis in 76 men: qualitative and quantitative CT evaluation-clinical-radiologic correlation study. Radiology 2003;228:816-25.
- Hertzberg VS, Rosenman KD, Reilly MJ, Rice CH. Effect of occupational silica exposure on pulmonary function. Chest 2002;122:721-28.
- Lopes AJ, Mogami R, Capone D, Tessarollo B, de Melo PL, Jansen JM. High-resolution computed tomography in silicosis: correlation with chest radiography and pulmonary function tests. J Bras Pneumol 2008;34:264-72.
- Rosenstock L, Barnhart S, Heyer NJ, Pierson DJ, Hudson LD. The relation among pulmonary function, chest roentgenographic abnormalities and smoking status in an asbestos-exposed cohort. Am Rev Respir Dis 1988;138:272-7.
- Lee YC, Singh B, Pang SC, de Klerk NH, Hillman DR, Musk AW. Radiographic (ILO) readings predict arterial oxygen desaturation during exercise in subjects with asbestosis Occup Environ Med 2003;60:201-6.
Yazışma Adresi (Address for Correspondence)
Dr. Recai ERG?N
Dışkapı Yıldırım Beyazıt Eğitim ve
Araştırma Hastanesi,
G?ğ?s Hastalıkları Kliniği,
ANKARA - TURKEY
e-mail: recaiergun@gmail.com