LETTER TO THE EDITOR
Doi: 10.5578/tt.8892
Tuberk Toraks 2016;64(1):87-90

İntratorasik dev fibrolipomanin radyolojik g?r?n?m?
Emine DAĞISTAN1, Abdullah Y?ksel BARUT2, Yeşim KARAG?Z3, Neslihan FENER4, Arzu CANAN5, Bet?l KIZILDAĞ1
1 Abant İzzet Baysal ?niversitesi Tıp Fak?ltesi, Radyoloji Anabilim Dalı, Bolu, T?rkiye
1 Department of Radiology, Faculty of Medicine, Abant Izzet Baysal University, Bolu, Turkey
2 İstanbul Gelişim ?niversitesi, Sağlık Bilimleri Enstit?s?, İstanbul, T?rkiye
2 Health Sciences Institude, Istanbul Gelisim University, Istanbul, Turkey
3 İstanbul Eğitim ve Araştırma Hastanesi, Radyoloji Kliniği, İstanbul, T?rkiye
3 Clinic of Radiology, Istanbul Training and Research Hospital, Istanbul, Turkey
4 Yedikule G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, Patoloji Kliniği, İstanbul, T?rkiye
4 Clinic of Pathology, Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey
5 Antalya Atat?rk Devlet Hastanesi, Radyoloji Kliniği, Antalya, T?rkiye
5 Clinic of Radiology, Antalya Ataturk State Hospital, Antalya, Turkey
Fibrolipomas are benign variants of lipomas. Although, lipomas are common benign tumors of soft tissue, intrathoracic lipomas especially fibrolipomas are very rare. They usually presents as a sharply delineated mass with a thin capsule/septation. The patients are commonly asymptomatic. Fibrolipomas are determined on chest radiograph incidentally. A radiography only showed the mass and location. Computed tomography (CT), magnetic resonance imaging (MRI) usually reveal characteristic findings of lipomatous mass, that is helpful for diagnosis (1).
We report an asymptomatic patient with a pedunculated huge intrathoracic fibrolipoma and its radiological findings.
A 45-year-old woman presented to clinic of Chest Disease with desire of check-up because of her age. The patient had no complaints. Her medical history was unremarkable. She was non-smoker, was not on medication. Physical examination revealed a normal blood pressure and pulse. The expansion of the thorax was symmetric. But, breath sounds were absent on the base of right hemithorax and there was dullness on percussion. The results of routine laboratory tests including arterial blood gas analysis were normal.
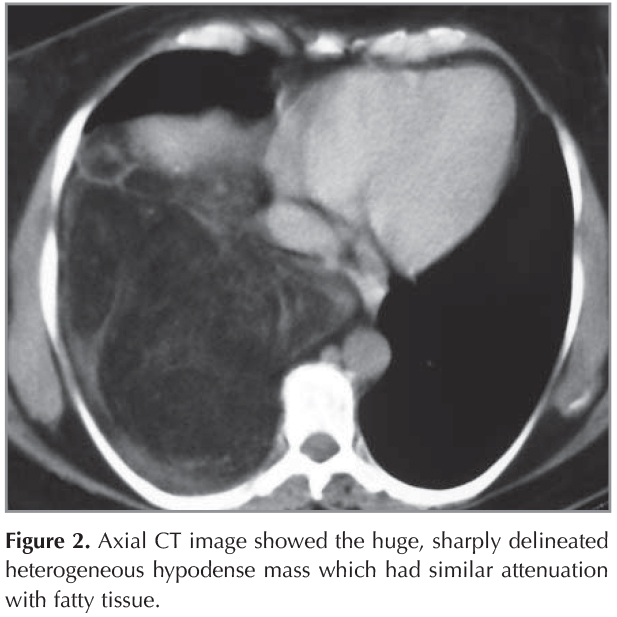
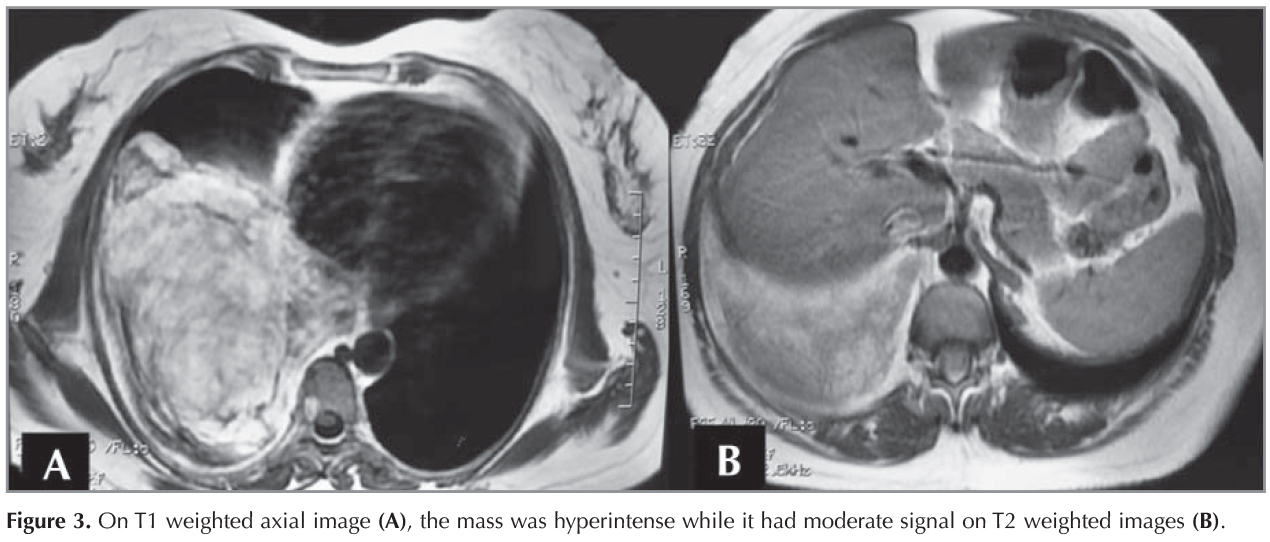
A chest radiograph revealed opacification of the lower part of the right hemithorax because of a well defined enormous mass (Figure 1). Thorax CT was performed to examine the origin of the mass (Figure 2). CT demonstrated a huge, sharply delineated heterogeneous hypodense mass lying between mediastinum and chest wall at the lower part of the right lung. The CT attenuation of the mass was -107 Hounsfield unit (HU) that was consistent with fatty tissue. The right hilar structures showed displacement to the anterior according to the mass, but there were no signs of infiltration. Only a small part of the right upper lobe appeared to be normal. No abnormalities were seen on the left side. Because of its higher soft tissue resolution, MRI was performed to determine the relationship of the mass with surrounding structures. MRI revealed a posteriorly located heterogeneous mass which filled the middle and lower part of the right hemithorax. On fast spin echo (FSE) T1 weighted images, the signal of the mass was hyperintense while it had moderate signal on FSE T2 weighted images (Figure 3). In addition, the mass was hypointense on the images with fat saturation. Short T1 inversion recovery (STIR) sequences demonstrated that the mass had similar signal intensity with fat tissue (Figure 4). After gadolinium injection, the mass showed no enhancement. Despite the performance of many tests, we did not exclude the possibility of malignancy such as liposarcoma. The patient denied operation. She wanted to have operation only the condition that the lesion was proved to be malignant. Hence, CT-guided percutaneous coaxial cutting needle biopsy was performed to investigate nature of lesion. The results of histologic examination of tumor was fibrolipomatous tissue with mononuclear cell infiltration but could not exclude possibility of malignancy. Thus, the patient was convinced to have operation.


After that, a right thoracotomy was performed, using a standard posterolateral incision. A large capsulated and pedunculated mass that originated from the parietal pleura was found. There were no attachments of the tumor to the lung and mediastinal structures. The mass measuring 21 x 17 x 5 cm with a stalk 2 cm in diameter was successfully excised. The patient made a normal recovery. She has been followed up with a chest radiography at 3, 6, 9 months after resection. At first year, CT was performed and after that she was followed up with CT every year for 5 years until she has migrated to another city. During the follow-up, she remained in good health without any signs of recurrence. The diagnosis of mass was a fibrolipoma.
Fibrolipoma is a variant of lipoma that consists of fibrous and lipomatous elements. Clinically, they have similar characteristics. Most patients with fibrolipomas are asymptomatic until incidental detection of the lesions at a radiography. The lesions grow slowly, therefore, the presenting symptoms are often secondary to mass effect including breathless, dysphagia due to compression of the adjacent structures such as esophagus, bronchus or nerves (1). Our patient had no symptoms.
Histologically, several histologic variants of lipomas were described including fibrolipoma, chondroid lipoma, angiolipoma, spindle cell and pleomorphic lipoma, myolipoma, and hibernoma. Fibrolipomas are an uncommon type with a mixture of fibrous connective tissue, arise from the maturation of lipoblastomatosis. The fibers of collagen separates fat cells into lobules, that is the characteristic sign of a fibrolipoma due to the maturation of both adipose and fibrous tissue (1,2).
Fibrolipomas are found usually on chest radiography incidentally and appear as a well-delineated opacity with variable size. CT was reliable imaging method for the lipomatous lesions, because it reveal their characteristic fat attenuation (approximately -100 HU) and often allow the diagnosis (3). MRI, especially images with fat saturation, also be helpful in demonstrating its lipomatous nature. The lesions have similar signal intensity with fat tissue (4). In our case, the CT attenuation of mass is suggested its lipomatous nature. MRI revealed a huge mass containing fat. In addition, T2 weighted images demonstrated with low-intensity in the mass showing a fibrous component. The differentiation lipoma and lipoma variants from liposarcomas are frequently a handicap for the radiologist. Because of its malign nature, the distinction of liposarcoma is very important. Liposarcomas show contrast enhancement on both CT and MRI, hence these findings may help to distinguish liposarcoma from benign lesions (5). However, the mass did not demonstrate any enhancement on any radiologic techniques in our case; we could not exclude the possibility of liposarcoma exactly without surgery. It is extremely diffcult to accurately differentiate lipoma from liposarcoma by preoperative diagnostic imaging. Hence, the gold standart for diagnosis is surgery in such cases.
Surgical excision is the curative treatment for many intrathoracic lipomatous tumors of any histologic type. However, fibrolipomas are benign tumors histologically, in clinical practise they are often accepted to be malignant because fibrolipomas have a higher risk of recurrence (3). Our patient had total excision of the mass and she had normal recovery without any complications. Also, during the follow-up she had no recurrence of the mass.
In conclusion, lipomas and its variants may reach huge size without any symptom. In such cases, radiological examination especially CT is helpful for showing its lipomatous nature. MRI can demonstrate the other components such as fibrous and is useful for differentiating from liposarcomas.
CONFLICT of INTEREST
None declared.
REFERENCES
- Gaerte SC, Meyer CA, Winer-Muram HT, Tarver RD, Conces DJ Jr. Fat-containing Lesions of the Chest RadioGraphics 2002;22:61-78.
- Hsu JS, Kang WY, Liu GC, Kao EL, Chuang MT, Chou SH. Giant fibrolipoma in the mediastinum: An unusual case. Ann Thorac Surg 2005;80:10-2.
- Kato M, Saji S, Kunieda K, Yasue T, Nishio K, Adachi M. Mediastinal lipoma: report of a case. Surg Today 1997;27:766-8.
- Sato S, Maekawa T, Sato K, Maekawa H, Ouchi K, Sakurada M, et al. Pedunculated giant fibrolipoma of the esophagus: a case report. Esophagus 2005;2:199-203.
- Garcia M, Buitrago E, Bejarano PA, Casillas J. Large esophageal liposarcoma: a case report and review of the literature. Arch Pathol Lab Med 2004;128:922-5.
Yazışma Adresi (Address for Correspondence)
Dr. Emine DAĞISTAN
Abant İzzet Baysal ?niversitesi Tıp Fak?ltesi,
Radyoloji Anabilim Dalı,
BOLU - TURKEY
e-mail: yemined@gmail.com