CASE REPORT
Doi: 10.5578/tt.8936
Tuberk Toraks 2016;64(1):69-72

β-HCG sektere eden k???k h?cre dışı akciğer kanseri
Burcu CİRİT KO?ER1, Yurdanur ERDOĞAN1, Berna AKINCI ?ZY?REK1, Serta? B?Y?KYAYLACI ?ZDEN1,
Funda DEMİRAĞ2
1 Ankara Atat?rk G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği,
Ankara, T?rkiye
1 Clinic of Chest Diseases, Ankara Ataturk Chest Diseases and Chest Surgery Training and Research Hospital,
Ankara, Turkey
2 Ankara Atat?rk G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, Patoloji Kliniği, Ankara, T?rkiye
2 Clinic of Pathology, Ankara Ataturk Chest Diseases and Chest Surgery Training and Research Hospital, Ankara, Turkey
?ZET
β-HCG sektere eden k???k h?cre dışı akciğer kanseri
K???k h?cre dışı karsinomlarında paraneoplastik B-HCG salınımı nadiren bildirilmiştir. 43 yaşında erkek hasta nefes darlığı ve g?ğ?s ağrısı şikayeti ile başvurdu. Toraks bilgisayarlı tomografisinde bilateral multipl kitleler ve sağda plevral ef?zyon saptandı. Pozitron emisyon tomografisinde kitle lezyonlarda ve mediastinal lenf nodlarında artmış FDG18 tutulumu g?r?ld?. Serum β-HCG değeri y?ksek olarak bulundu. Yapılan bronkoskopide endobronşiyal lezyon saptandı. Lezyondan alınan biyopsi ?rneğinin patolojik incelemesinde tanı ayrımı yapılamaması ?zerine hastaya ikinci kez bronkoskopi yapıldı ve kriyobiyopsi alındı. Alınan ?rneğin patolojik incelemesi k???k h?creli dışı akciğer kanseri ile uyumlu geldi. Sonu? olarak olgu β-HCG sekrete eden k???k h?cre dışı akciğer kanserlerinin nadir olması nedeni ile sunuldu.
Anahtar kelimeler: β-HCG, k???k h?cre dışı akciğer kanseri, jinekomasti.
SUMMARY
β-HCG secretion by a non-small cell lung cancer: a case report
Paraneoplastic secretion of beta human chorionic gonadotropin (β-HCG) in non-small cell lung cancer (NSCLC) has been rarely reported. A 43-year old male patient was admitted with dyspnea and chest pain. Thorax computed tomography (CT) revealed bilateral multiple masses and pleural effusion at right hemithorax. Positron emission tomography (PET)-CT showed pathologic 18 FDG uptake at mass lesions and mediastinal lymph nodes. The serum β-HCG level was elevated. A bronchoscopy was performed and endobronchial lesion was observed. Since a definitive diagnosis was not achieved by pathologic examination of biopsy specimen, bronchoscopy was repeated and a sample was taken by cryobiopsy. The pathologic examination revealed non-small cell lung cancer.In conclusion, the case was presented because of extremely rare occurence of NSCLC secreting β-HCG.
Key words: β-HCG, non-small cell lung cancer, gynaecomastia
Geliş Tarihi/Received: 13.01.2015 • Kabul Ediliş Tarihi/Accepted: 04.02.2015
INTRODUCTION
Paraneoplastic syndromes occur in approximately 10% of patients with lung cancer and may be the initial presenting complaint, however, they also may develop late in the course of disease. The awareness of paraneoplastic syndromes associated with lung cancer may lead to earlier diagnosis of malignancy.
Human chorionic gonadotropin (HCG) is a hormone secreted by placental syncytiotrophoblasts and measurable serum β-human chorionic gonadotropin (β-HCG) is usually consistent with a pregnancy or pregnancy-related conditions such as gestational trophoblastic tumors. However, β-HCG can also be detected in conditions not associated with pregnancy. Paraneoplastic syndromes involving β-HCG production have been reported arising from tumors of multiple tissues, including bone, breast and stomach (1). Lung cancer also can secrete β-HCG as an ectopic hormone.
?We report here a rare case of non-small cell lung cancer (NSCLC) secreting β-HCG in a male patient.
CASE REPORT
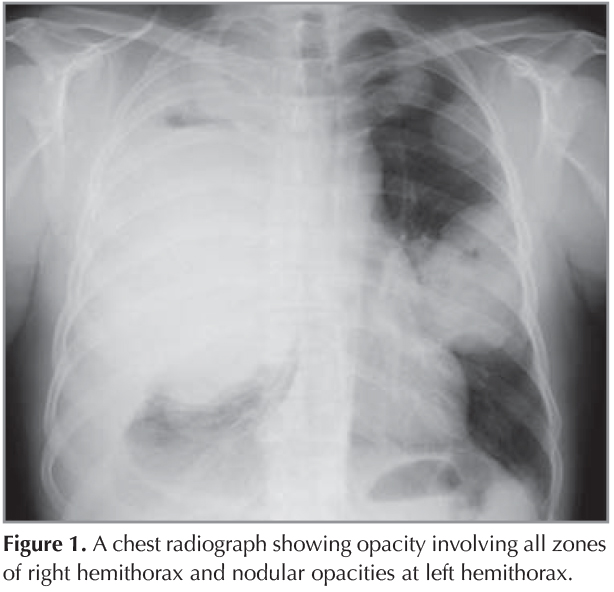
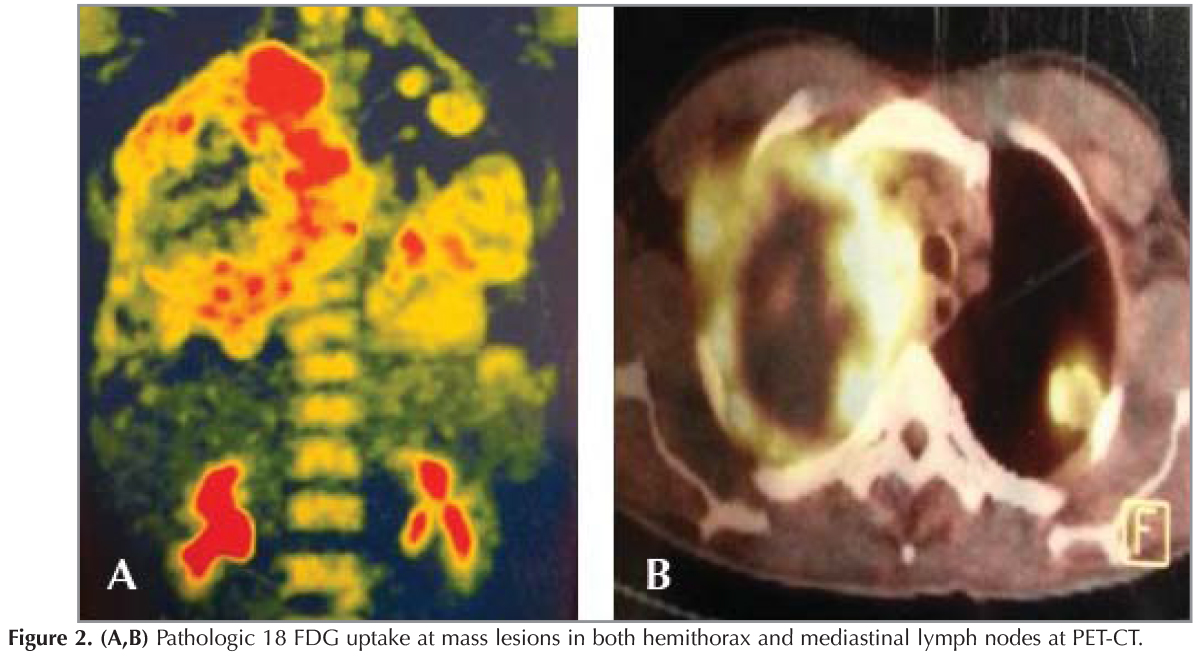
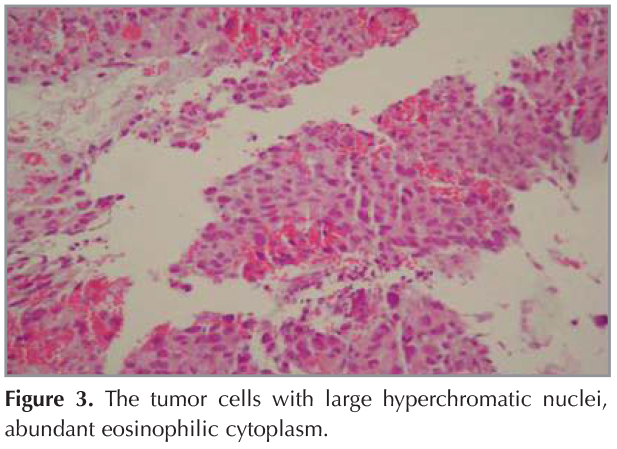
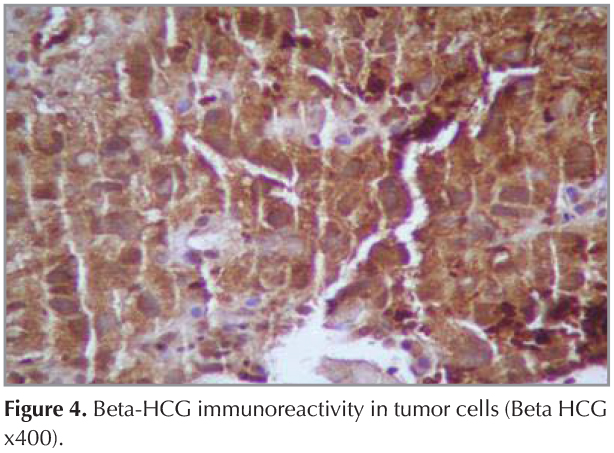
?A 43-year old male patient was admitted with dyspnea and chest pain. On physical examination the breath sounds were markedly diminished at right hemithorax and he had bilateral gynaecomastia. He was a smoker and his smoking history was 22 pack years. A chest radiograph showed opacity involving all zones of right hemithorax and nodular opacities at left hemithorax (Figure 1). A thorax computed tomography (CT) revealed a mass lesion occupying almost all right hemithorax and multiple masses in the left hemithorax. There was also pleural effusion and compression atelectasis at right hemithorax. Laboratory studies revealed a normal complete blood count and serum biochemistry. The erythrocyte sedimentation rate was elevated. Since he was a young patient, had bilateral multiple masses at thorax CT and also had gynaecomastia, a germ cell tumor was suspected and serum β-HCG level was analyzed. The serum β-HCG level was found as elevated: 4261 mIU/mL (normal less then 2.0). Positron emission tomography (PET)-CT revealed pathologic 18 FDG uptake at mass lesions in both hemithorax and mediastinal lymph nodes (Figure 2). Positron emission tomography and ultrasonography showed no gonadal involvement. A bronchoscopy was performed and an endobronchial lesion at the apical segment of right upper lobe was observed. A definitive diagnosis was not achieved by pathologic examination of biopsy specimen, bronchoscopy was repeated and samples were taken by cryobiopsy. Tumor consisted of solid sheets of uniform large tumor cells (Figure 3). Tumor cells were positive with P63 and β-HCG (Figure 4). Keratin 5/6, TTF-1, PLAP and AFP were negative in tumor cells. Mucine carmin staining was negative. We didn't observe syncytiotrophoblast and cytotrophoblast. Our case was β-HCG secreting nonsmall cell lung carcinoma. Since the patient was inoperable, a chemotherapy protocol was started.
DISCUSSION
Human chorionic gonadotropin is a dimer of α and β subunits. While the α subunit is present in many hormones, the β subunit is unique to trophoblast cells and hence may be used as a marker of pregnancy. However, serum β-HCG may also be elevated in conditions not associated with pregnancy. A high level of β-HCG may be seen in choriocarcinomas and germ cell tumors. One of the causes of elevation in serum β-HCG level is paraneoplastic syndromes, seen in various malignancies. Paraneoplastic β-HCG secretion has been reported in squamous cell carcinoma of the head, breast cancer, renal cell carcinoma, gastrointestinal malignancies, gynecologic and urologic cancers, lymphoma and sarcomas (2,3,4,5,6). β-HCG secretion is rarely associated with lung cancer and limited cases have been reported previously (7,8,9).
Vicier et al. reported a β-HCG-secreting lung adenocarcinoma in a 43-year-old woman (7). They reported that, after first-line chemotherapy, a progression in tumor with an increase in β-HCG level was observed. However, after modification of chemotherapy, a partial tumor response with a markedly decrease in β-HCG level was obtained. In another report, Yoshida et al. described a case of pulmonary squamous cell carcinoma secreting β-HCG in a young female patient, in whom, after two months of surgery, the β-HCG dropped to normal levels (8).
The number of case reports on β-HCG secreting lung cancer, especially in men, is extremely rare and to our knowledge, there are only two reports in the literature (9,10). Niimi et al. reported a case of hCG-producing large cell carcinoma of the lung in a 73-year-old man patient (9). They also reported that, serum hCG levels fluctuated in parallel with the response of the cancer to surgery, chemotherapy and radiotherapy. Goyal et al. reported a case of squamous cell lung cancer with high serum β-HCG level, galactorrhoea and gynaecomastia, and the authors concluded that, lung cancer should be considered in a male patient presenting with gynaecomastia and/or galactorrhoea (10).
In most of the reported female patients with β-HCG-secreting lung cancers, β-HCG was examined because of a suspicion of pregnancy. In contrast, in the male patient reported by Niimi et al., serum β-HCG level was measured because of gynaecomastia. Our case was a young patient and had bilateral multiple mass lesions, gynaecomastia, thus, the serum β-HCG level was examined for a suspicion of germ cell tumor.
In conclusion, we report a rare case of β-HCG secreting non-small cell lung cancer in a male patient. Elevated serum β-HCG levels may be observed in lung cancer, and symptoms caused by high serum β-HCG levels may lead to an early diagnosis of malignancy.
CONFLICT of INTEREST
None declared.
REFERENCES
- Marcillac I, Troalen F, Bidart JM, Ghillani P, Ribrag V, Escudier B, et al. Free human chorionic gonadotropin beta subunit in gonadal and nongonadal neoplasms. Cancer Res 1992;52:3901-7.
- Turner JH, Ross H, Richmon J. Secretion of beta-HCG from squamous cell carcinomas of the head and neck. Otolaryngol Head Neck Surg 2010;143:169-70.
- Reisenbichler ES, Krontiras H, Hameed O. Beta-human chorionic gonadotropin production associated with phyllodes tumor of the breast: an unusual paraneoplastic phenomenon. Breast J 2009;15:52-30.
- Mohammed Ilyas MI, Turner GD, Cranston D. Human chorionic gonadotropin-secreting clear cell renal cell carcinoma with paraneoplastic gynaecomastia. Scand J Urol Nephrol 2008;42:555-7.
- Mansi IA, Ashley I, Glezerov V. Retroperitoneal leiomyosarcoma and enlarged epididymis associated with a positive pregnancy test. Am J Med Sci 2002;324:104-5.
- Inoue N, Watanabe H, Takehara H, Hamazaki M, Kagami S. Refractory pediatric nonrhabdomyosarcoma soft tissue sarcoma associated with ectopic production of beta hCG and hypercalcemia induced by PTHrP. Pediatr Blood Cancer 2011;57:1244-6.
- Vicier C, Tabouret E, Tallet A, Gon?alves A, Chetaille B, Viens P, et al. Beta HCG secretion by a pulmonary adenocarcinoma. World J Surg Oncol 2013;14;11:228.
- Yoshida J, Nagai K, Nishimura M, Takahashi K, Kakinuma R, Nishiwaki Y, et al. Secretion of hCG/beta-hCG by squamous cell carcinoma of the lung in a 31-year-old female smoker. Jpn J Clin Oncol 2000;30:163-6.
- Niimi T, Kajita M, Yamauchi M. A case of hCG-producing large cell carcinoma of the lung-clinical utility of serum hCG levels. Nihon Kyobu Shikkan Gakkai Zasshi 1992;30:964-9.
- Goyal A, Singh N, Bal A, Behera D. Gynaecomastia, galactorrhoea, and lung cancer in a man. Lancet 2013;13:1332.
Yazışma Adresi (Address for Correspondence)
Dr. Burcu CİRİT KO?ER
Ankara Atat?rk G?ğ?s Hastalıkları ve
G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi,
G?ğ?s Hastalıkları Kliniği,
ANKARA - TURKEY
e-mail: drcirit@hotmail.com