RESEARCH ARTICLE
Doi: 10.5578/tt.9167
Tuberk Toraks 2016;64(1):27-33

Akciğer t?berk?lozu temaslılarında hastalanma ve koruyucu tedavinin etkinliği
Bektaş KISA1, Nesrin SARIMURAT2, Sinem KOYMAN2, Şevket SAYICI3, Aylin BABALIK4, Zeki KILI?ASLAN5
1 ?sk?dar Verem Savaş Dispanseri, İstanbul, T?rkiye
1 Uskudar Tuberculosis Dyspanseries, Istanbul, Turkey
2 Şehremini Verem Savaş Dispanseri, İstanbul, T?rkiye
2 Sehremini?Tuberculosis Dyspanseries, Istanbul, Turkey
3 G?ng?ren Verem Savaş Dispanseri, İstanbul, T?rkiye
3 Gungoren Tuberculosis Dyspanseries, Istanbul, Turkey
4 S?reyyapaşa G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği,
İstanbul, T?rkiye
4 Clinic of Chest Diseases, Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital,
Istanbul, Turkey
5 İstanbul ?niversitesi İstanbul Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, İstanbul, T?rkiye
5 Department of Chest Diseases, Faculty of Istanbul Medicine, Istanbul University, Istanbul, Turkey
?ZET
Akciğer t?berk?lozu temaslılarında hastalanma ve koruyucu tedavinin etkinliği
Giriş: Bu ?alışmada İstanbul'da bulunan d?rt dispanserimizin 2005-2009 yıllarındaki akciğer t?berk?lozu olgularının temaslı tarama sonu?ları retrospektif olarak değerlendirildi.
Hastalar ve Metod: Bu d?nemde tedavi edilen 1909 akciğer t?berk?lozu olgusunun 7453 temaslısının 6114' ? en az bir kere kontrol edilmiş ve ortalama 2.9 yıl takip edilmişlerdi.
Bulgular: Bu takip s?reci i?inde t?m temaslılar i?inde hasta bulunma oranı %2.46 (184/7453) bulundu, bu oran yayma pozitif olgu temaslıları i?inde %3.05 (163/5335) iken, yayma (-) olgu temaslıları i?inde %0.99 (21/2118) idi. On altı yaş altı ?ocuklarda PPD pozitif bulunma oranı yayma (+) olgu temaslıları i?inde %33.3 (376/1126) iken, yayma (-) olgu temaslıları i?inde %19.50 (71/364)bulundu. Bu yaş grubu yayma pozitif olgu temaslılarında hasta bulunma oranı %2.31 (32/1384), yayma (-) olgu temaslıları i?inde ise %0.55 (3/536) idi. Yayma pozitif olgu temaslıları i?inde 16-35 yaş arası olanlarda hasta ?ıkma oranı %4.34 (96/2207) iken bu oran 35 yaş ?st? temaslılarda %2.06 (36/1744) bulundu. 16 yaş altı yayma (+) olgu temaslısı ?ocuklar i?inde altıncı aydan sonra hasta bulunma oranı koruyucu tedavi alanlar i?inde %0.65 (6/912) koruyucu tedavi almayanlar i?inde ise %1.98 (9/455) bulundu. 16-35 yaş grubu yayma pozitif olgu temaslıları i?inde bu oranlar sırasıyla %0 (0/330) ve %2.94 (54/1832), 36 yaş ?st? temaslılar i?inde ise %0 (0/215) ve %0.98 (15/1522) bulundu.
Sonu?: Sonu? olarak yayma pozitif olgu temaslıları arasında hastalanma ve infekte olma riski y?ksektir. Temaslıların koruyucu tedavisi hem ?ocuk yaş grubunda hem de, ?zellikle 15-35 yaş arasında olmak ?zere, erişkinlerde de etkilidir.
Anahtar kelimeler: Akciğer t?berk?lozu, temaslı taraması, balgam pozitifliği, profilaksi
SUMMARY
Tuberculosis screening and efficacy of prophylaxis in contacts of patients with pulmonary tuberculosis
Introduction: To evaluate tuberculosis screening and efficacy of prophylaxis in contacts of patients with pulmonary tuberculosis.
Patients and Methods: A total of 7453 contacts of 1909 patients with pulmonary tuberculosis treated at four tuberculosis dispensaries located in Istanbul, between 2005 and 2009 were included in this retrospective screening-based study. Data on demographics, smear positivity, PPD positivity, rate and onset of secondary tuberculosis and prophylaxis were recorded in contacts.
Results: Overall 184 (2.5%) secondary cases of tuberculosis were identified within a mean 2.9 (1-5) years of follow-up. The rate for secondary tuberculosis was 3.1% (163/5335) in smear positive and 1.0% (20/2118) in smear negative contacts. With and without prophylaxis rates for secondary tuberculosis after 6 months of index case was identified in 0.7% (6/912) and 2.0% (9/455) of contacts aged 0-15 years, in 0.9% (3/339) and 2.8% (51/1826) of contacts aged 16-35 years and in 0% (0/215) and 0.9% (14/1507) of contacts aged ≥ 36 years, respectively.
Conclusion: In conclusion, our findings indicate high risk of being infected and diseased in smear positive contacts along with efficacy of prophylactic therapy among contacts not only in the childhood but also in adults, particularly in contacts aged 16-35 years.
Key words: Pulmonary tuberculosis, contact investigation, smear positivity, prophylaxis
Geliş Tarihi/Received: 15.02.2015 • Kabul Edilis Tarihi/Accepted: 26.10.2015
INTRODUCTION
Tuberculosis (TB) remains a major global health problem along with 8.6 million people estimated to develop TB and 1.3 million to die from the disease in 2012 (1). In accordance with the targets to control TB set by The World Health Organization (WHO) STOP TB Partnership, including reduction of prevalence and deaths by 50% by 2015, relative to 1990 levels; and elimination TB as a public health problem by 2050, healthcare systems will need to identify more cases of TB at an earlier stage of the illness (2,3).
Detected proportion of incident global TB cases, has been indicated to be below the WHO target of 70%, while to improve the case detection rate by active and systematic screening all household contacts of pulmonary TB patients, considered to be at increased risk for TB infection, has been proposed (4,5,6). Hence, given the higher risk of exposure to the causative organism in contacts of patients with TB than in general population, active case finding has been considered to be valuable strategy, while the infectiousness of the TB patient, the duration and proximity of the contact and susceptibility of the contact have been associated with the risk of a contact becoming infected (7,8,9,10,11), or the onset of disease that may occur early, within 6 weeks, or many years later (7,8,9,10,11).
Accordingly, contact investigation, one of the most widely discussed public health strategies for reducing TB and the risk of transmission, has been recommended by WHO in two high-risk populations including children aged < 5 years and people living with, or at high risk of, HIV infection, while recently issued International Standard for Tuberculosis Care states that contact investigation warrants more effort to ensure that close contacts of infectious TB patients are evaluated and managed (4,5,13,14,15,16,17).
Prophylactic therapy aims to prevent the development of infection in a contact of tuberculosis patient, which has not yet been investigated in randomized trials, or the development of disease in a tuberculosis infected person, as demonstrated in large scale double-blind randomized placebo-controlled studies (18,19). Enabling prevention of the development of disease among patients with latent infection and thus new bacillus source, prophylactic therapy has also been considered important in the epidemiological control of tuberculosis (18,19).?
The presents study was designed to evaluate tuberculosis screening and efficacy of prophylaxis in contacts of patients with pulmonary tuberculosis, retrospectively based on data from dispensaries in Istanbul between 2005 and 2009.
METARIALS and METHODS
Study Population and Methods
A total of 7453 contacts of 1909 patients with pulmonary tuberculosis treated at four tuberculosis dispensaries (Uskudar, Beykoz, Sehremini, Gungoren) located in Istanbul, between 2005 and 2009 were included in this retrospective screening-based study (Table 1). Contacts diagnosed within the first 6 months of index case (n= 81) were excluded from the study given the existence of variability in the timing of the first control of contacts during the first 6 months (n= 76) and the diagnosis of the disease during the prophylaxis (n= 5).

The study was conducted in full accordance with the ethical principles stated in the "Declaration of Helsinki" and the permission was obtained from institutional review board of Istanbul University for the use of patient data for publication purposes.
Study parameters
Data on demographics (age, age groups), smear positivity, PPD positivity, rate and onset of secondary tuberculosis and prophylaxis were recorded in contacts.
Contacts
Household contacts (98%) and individuals having close contact with a patient at the working place or school environment were considered to be contacts of a patient with pulmonary tuberculosis. Contacts of index cases having microfilm investigation for at least once and/or PPD test were considered to be screened. Diagnosis of infection among contacts was based on the presence of PPD ≥ 15 mm in individuals with BCG scar, while PPD ≥ 10 mm in individuals without BCG scar (18).
Prophylaxis
Prophylaxis was applied to ≤ 15 year-old contacts of smear positive pulmonary tuberculosis cases in three dispensaries and to PPD positive contacts of smear negative pulmonary tuberculosis cases in one dispensary, whereas prophylaxis applied to contacts of MDR tuberculosis cases were not included in the analysis.? ?
Diagnosis of infection in a contact was based on presence of smear positivity and/or culture positivity or presence of a clinical radiological response to treatment in case of smear negativity and/or culture negativity.
Definitions
Index case was defined as the initially identified case of new or recurrent TB in a person of any age in a specific household or other comparable setting in which others may have been exposed. Any person who has been exposed to an index case was considered to be a contact of patient. Household contact was defined as the person who shared the same enclosed living space for one or more nights or for frequent or extended periods during the day with the index case during the 3 months before commencement of the current treatment episode (5).Close contact was defined as a person who is not in the household but shared an enclosed space, such as a social gathering place, workplace or facility, for extended periods during the day with the index case during the 3 months before commencement of the current treatment episode.
Contact investigation was considered to be a systematic process intended to identify previously undiagnosed cases of TB among the contacts of an index case consisting of two components including identification and prioritization, and clinical evaluation. In some settings, the goal also included testing for latent TB infection (LTBI) to identify possible candidates for preventive treatment (5).
Statistical Analysis
Descriptive statistics (count, percentage, min-max) were used to summarize results.
RESULTS
Total and Secondary Tuberculosis (+) Contacts with Respect to Age and Smear Positivity
Among the 7453 contacts (71.5% were smear positive), 25.8% aged 0-15 years (72.1% were smear positive), 40.9% aged 16-35 years (72.4% were smear positive) and 33.3% aged ≥ 36 years (70.2% were smear positive). Overall 184 (2.5%) secondary cases of tuberculosis (1.8% in 0-15 years, 3.6% in 16-35 years and 1.5% in ≥ 36 years of age) were identified within a mean 2.9 (1-5) years of follow-up. The rate for secondary tuberculosis was 3.1% (163/5335) in smear positive and 1.0% (20/2118) in smear negative contacts (Table 2).
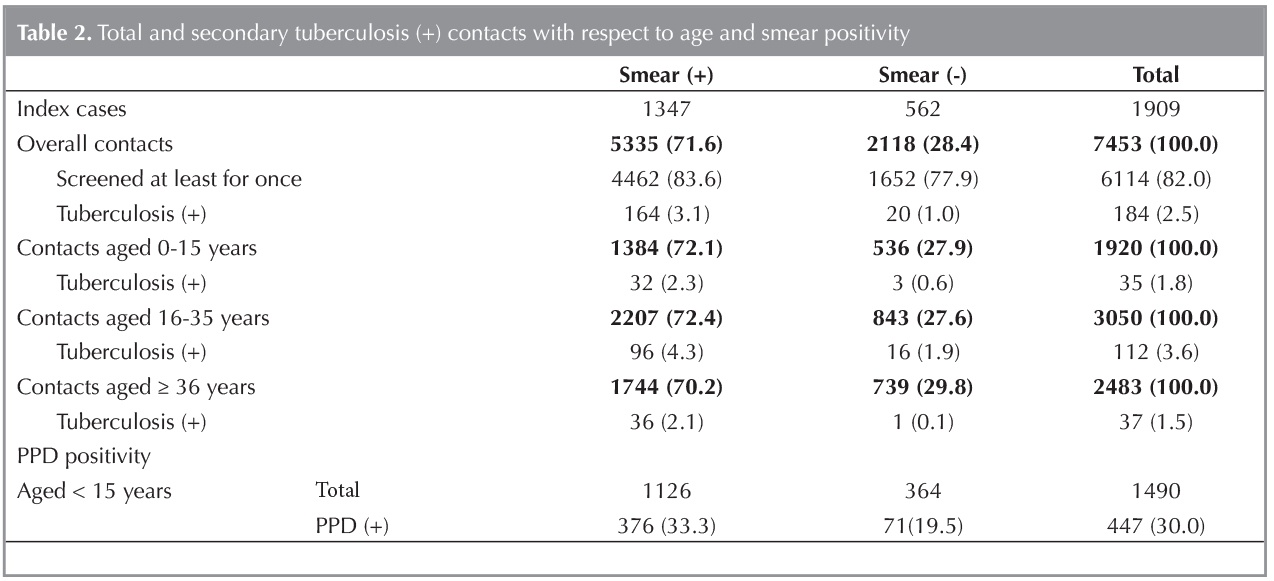
In contacts aged 0-15 years, PPD positivity was detected in 33.3% (376/1126) of smear positive? and 19.5% (71/364) of smear negative cases, while secondary tuberculosis was identified in 2.3% (32/1384) and 0.6% (3/536) of smear positive and negative cases, respectively (Table 2).?
In contacts aged 16-35 years, secondary tuberculosis was identified in 4.3% (96/2207) of smear positive and 1.9% (16/843) of smear negative cases. In contacts aged ≥ 36 years, secondary tuberculosis was identified in 2.1% (36/1744) of smear positive and 0.1% (1/739) of smear negative cases (Table 2).?
Disease Onset and Prophylaxis in Smear Positive Contacts
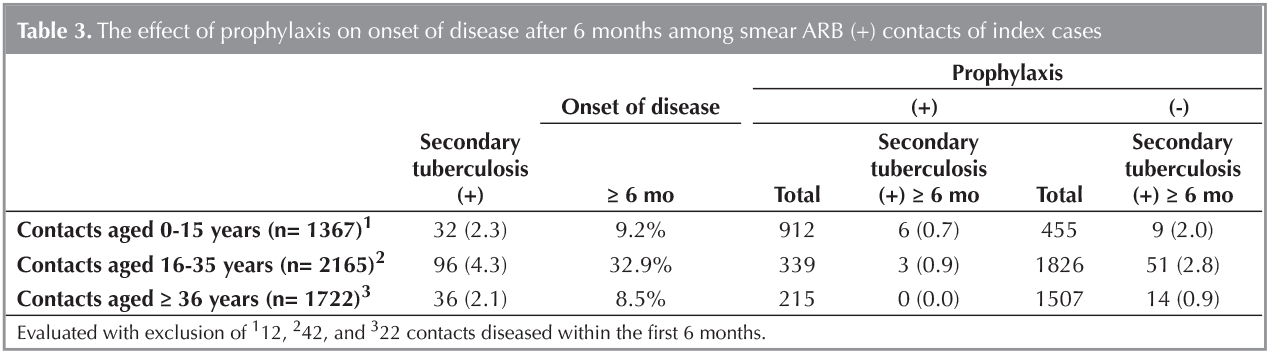
In contacts aged 0-15 years, secondary tuberculosis after 6 months of index case was identified in overall 9.2% of cases, in 0.7% (6/912) of cases who received prophylaxis and in 2.0% (9/455) of cases without prophylaxis. Total, with and without prophylaxis rates for secondary tuberculosis were 32.9% and 0.9% (3/339) and 2.8% (51/1826) in contacts aged 16-35 years, while 8.5%, 0%(0/215) and 0.9% (14/1507) in contacts aged ≥ 36 years, respectively (Table 3).
DISCUSSION
Our findings revealed the diagnosis of secondary tuberculosis in overall 2.5% of contacts within a mean 2.9 (1-5) years of follow-up. Higher rate for secondary tuberculosis was noted in smear positive (3.1%) than in smear negative (1.0%) contacts along with the efficacy of prophylaxis both in childhood and adult age groups, particularly in contacts aged 16-35 years.
Systematic reviews of published studies showed that a pooled average of 3.5-5.5% (the equivalent of a prevalence of 3500-5500 per 100.000 population) of household members or other close contact with a person who has infectious TB are themselves have previously undiagnosed, active TB, although there is considerable heterogeneity in these results (20,21).
Contact investigation has been suggested to result in earlier identification of cases, possibly decreasing disease severity and reducing transmission of Mycobacterium tuberculosis, whereas being performed in only a few countries with high to medium incidences of TB, despite this potential benefit (5).
Given that incidence of new cases is highest in the first year and remains above background incidence for at least 5 years after exposure to a patient with TB, diagnosis of secondary tuberculosis in overall 2.5% of contacts (99.8% were household contacts) within a mean 2.9 (1-5) years of follow-up in our study seems consistent with the primary goal of contact investigation, that is to identify disease and infection among high-risk individuals near the time of exposure, while also highlights the potential importance of serial screening for TB in contacts in concentric circles starting with household contacts and progressing through other close contacts to more remote contacts (21,22).
High rate for secondary tuberculosis among contacts with smear positivity in our study population is in agreement with the consideration of pulmonary tuberculosis with ARB positive sputum microscopy as the most infective cases, while lower infectivity of smear negative cases (23).
It has been recommended that contact investigation be conducted for house- hold and close contacts when the index case has any of the characteristics including having sputum smear-positive pulmonary tuberculosis, MDR-TB or XDR-TB (proven or suspected),? being a PLHIV or? a child < 5 years of age (5).
Considering smear positive contacts aged 0-15 years, 16-35 years and ≥ 36 years in our study, 2.3%, 4.3 and 2.1% had secondary tuberculosis with onset of disease after 6 months in 9.2%, 32.9% and 8.5% cases and lesser in patients received prophylaxis, respectively.
In this regard, in addition to existing priority given in WHO recommendations for screening children aged < 5 years, our findings also indicate the likelihood of being at risk of infected or developed active disease in the adult population of contacts (24). Likewise, relatively high risk of active disease and latent infection and thereby likelihood of benefit from additional interventions was also reported among contacts aged 5-14 years in a recent meta-analysis (21).
In a meta-analysis of data from 41 household contact investigation studies in low?middle-income countries up to 2005 revealed that the yield for all tuberculosis (bacteriologically confirmed and clinically diagnosed) was 4.5% (95% CI 4.3-4.8, I (2) = 95.5%) of contacts investigated and 2.3% (95% CI 2.1-2.5, I (2) = 96.6%) for cases with bacteriological confirmation, while latent tuberculosis infection was reported in 51.4% (95% CI 50.6-52.2, I (2) = 99.4%) of contacts investigated (20).
In a recent systematic review and meta-analysis of 203 published studies reporting the prevalence of TB and latent TB infection, and the annual incidence of TB among contacts of patients with TB, in 95 studies from low- and middle-income settings, the prevalence of active TB in all contacts was 3.1% (95% CI 2.2-4.4%, I (2) = 99.4%), microbiologically proven TB was 1.2% (95% CI 0.9-1.8%, I (2) = 95.9%), and latent TB infection was 51.5% (95% CI 47.1-55.8%, I (2) = 98.9%), while in 108 studies from high-income settings, the prevalence of TB among contacts was 1.4% (95% CI 1.1-1.8%, I (2) = 98.7%), and the prevalence of latent infection was 28.1% (95% CI 24.2-32.4%, I (2) = 99.5%) (21).
Additionally, while those with newly acquired LTBI are considered to be at high risk of progression to disease within 2 years of infection without isoniazid preventive therapy (IPT), especially if they are children under the age of 5, our findings revealed secondary tuberculosis rates after 6 months of index case in cases with and without prophylaxis to be 0.7% (6/912) and 2.0% (9/455) in contacts aged 0-15 years, 0.9% (3/339) and 2.8% (51/1826) in contacts aged 16-35 years and 0% (0/215) and 0.9% (14/1507) in contacts aged ≥ 36 years, respectively indicating that benefit obtained from prophylaxis also in older age groups of contacts, particularly in 16-35 years of age (25).
Hence, our findings support the statement that contact tracing remains an important tool for TB control given that it allows for the identification of other TB suspects in the household so that they can be evaluated for or be given prophylaxis against active TB (25).
In a systematic review of 11 randomized controlled clinical trials of isoniazid preventive therapy for 6-12 months, treatment was reported to result in a relative risk for active TB of 0.40 (95% confidence interval, 0.31-0.52) over 2 years or longer (26). Only two of these studies, however, were from high-burden, low-income countries, while factors such as feasibility, drug availability and cost have been suggested to be considered before recommending routine treatment for LTBI as a component of contact investigation in such settings (26).
In a past study on the change in child household contact management of pulmonary tuberculosis cases before and after the implementation of an isoniazid preventive therapy (IPT) in an African setting, after pilot implementation of an IPT register, documented identification of child contacts, IPT initiation and IPT adherence documentation in TB exposed children was reported to be improved (27). Indeed, adherence to tuberculosis related prophylactic therapy has been reported to be high in Turkey as reported to reach 70% in 2008, while the efficacy of prophylactic therapy in different age groups in the framework of contact investigation requires further investigation (28).
Although interferon-gamma release assays, now commonly used in high-income areas, are currently too costly for routine use in high-burden settings, they may prove valuable for identifying LTBI in places where coverage with bacillus Calmette-Gu?rin is high, if or when the price drops (29). Use of this category of tests should be evaluated under programme conditions in high-burden settings to determine their performance, practicality and feasibility in contact investigations.
Association between contact investigation and the reduction of the incidence of TB in a population, cost-effectivity of contact investigation in terms of the cost per new case identified have been suggested to be addressed in future investigations, while development of standardized protocols for optimal approaches to screening and clinical evaluation of contacts has been emphasized which would enable identification of country-specific barriers to implementation (5). Although cost-effectivity of screening strategy among the household contacts remains controversial, identification and thereby elimination of all potential transmission sources has been considered to be a prerequisite for eradicating tuberculosis from the population totally (30,31).
The main strengths of the present study is its large sample size with inclusion of number of contacts of index cases that is sufficient to reflect the overall population living in Istanbul province as well as inclusion of a follow up period of first three years as associated with the highest risk of developing disease among contacts. However, inability to include all contact cases and exclusion of contacts diagnosed within the first 6 months of index case (n= 81) and lack of data on HIV status, albeit a low prevalence to be a major confounder in Turkey, seems to be the limitations of the present study that should be taken into account in evaluating the results.
Conclusion
In conclusion, our findings indicate high risk of being infected and diseased in smear positive contacts along with efficacy of prophylactic therapy among contacts not only in the childhood but also in adults, particularly in contacts aged 16-35 years. Although our findings provide evidence that contacts are a high-risk group for developing TB, further investigation in randomized studies in relevant populations are needed to determine the cost-effectiveness of various contact tracing strategies and also to develop? a standardized tracing strategy via incorporating complementary strategies to enhance contact investigation (21).
REFERENCES
- World Health Organization. Global tuberculosis control 2011. Geneva, WHO, 2011.
- World Health Organization, Stop TB Partnership. The Stop TB Strategy: Building on and enhancing DOTS to meet the TB-related Millennium Development Goals. Geneva, WHO, 2006.
- Stop TB Partnership. The Global Plan to Stop 2011-2015. Transforming the fight towards elimination of tuberculosis. Geneva, WHO, 2010.
- World Health Organization: Global tuberculosis report 2013. Geneva, Switzerland: WHO; 2013. WHO/HTM/TB/ 2013.11.
- World Health Organization: Recommendations for investigating contacts of persons with infectious tuberculosis in low- and middle-income countries. Geneva, Switzerland: WHO; 2012. WHO/HTM/TB/2012.9.
- Thanh TH, Ngoc SD, Viet NN, Van HN, Horby P, Cobelens FG, et al. A household survey on screening practices of household contacts of smear positive tuberculosis patients in Vietnam. BMC Public Health 2014;14:713.
- Greenaway C, Palayew M, Menzies D. Yield of casual contact investigation by the hour. Int J Tuberc Lung Dis 2003;7(Suppl 3):S479-S85.
- Fok A, Numata Y, Schulzer M, FitzGerald MJ. Risk factors for clustering of tuberculosis cases: a systematic review of population-based molecular epidemiology studies. Int J Tuberc Lung Dis 2008;12:480-92.
- Kenyon TA, Valway SE, Walter WI, Onorato IM, Castro KG. Transmission of multidrug-resistant Mycobacterium tuberculosis during a long airplane flight. N Engl J Med 1996;334:933-8.
- Yim J, Selvaraj P. Genetic susceptibility in tuberculosis. Respirology 2010;15:241-6.
- Suggaravetsiri P, Yanai H, Chongsuvivatwong V, Naimpasan O, Akarasewi P. Integrated counseling and screening for tuberculosis and HIV among household contacts of tuberculosis patients in an endemic area of HIV infection: Chiang Rai, Thailand. Int J Tuberc Lung Dis 2003;7(Suppl 3): S424-S31.
- Marks SM, Taylor Z, Qualls NL, Shrestha-Kuwahara RJ, Wilce MA, Nguyen CH. Outcomes of contact investigations of infectious tuberculosis patients. Am J Respir Crit Care Med 2000;162:2033-8.
- Reichler MR, Reves R, Bur S, Thompson V, Mangura BT, Ford J, et al. Contact investigation study group. Evaluation of investigations conducted to detect and prevent transmission of tuberculosis. JAMA 2002;287:991-5.
- Joint Tuberculosis Committee of the British Thoracic Society. Control and prevention of tuberculosis in the United Kingdom: code of practice 2000. Thorax 2000; 55: 887-901.
- Riechler HL. Contacts of tuberculosis patients in high-incidence countries. Int J Tuberc Lung Dis 2003;7(Suppl 3):S333-S6.
- World Health Organization. International Standards for Tuberculosis Care: Diagnosis, Treatment, Public Health. The Hague, Tuberculosis Coalition for Technical Assistance, 2006.
- Tuberculosis Coalition for Technical Assistance: International standards for tuberculosis care, 3rd ed. The Hague: TB CARE I; 2014.
- Ministry of Health Tuberculosis Diagnosis and Treatment Guide, Ankara 2011, paper 115.
- Iseman MD. Guide for Tubeculosis for clinicians [Klinisyenler i?in t?berk?loz kılavuzu]. Translated by Ozkara S. Istanbul: Nobel Tip Publications, 2002:355-98.
- Morrison J, Pai M, Hopewell PC. Tuberculosis and latent tuberculosis infection in close contacts of people with pulmonary tuberculosis in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis 2008;8:359-68.
- Fox GJ, Barry SE, Britton WJ, Marks GB. Contact investigation of tuberculosis, a systematic review and meta-analysis. Eur Respir J 2013;41:140-56.
- Veen J. Microepidemics of tuberculosis: the stone-in-the-pond principle. Tuber Lung Dis 1992;73:73-6.
- Behr MA, Warren SA, Salamon H, Hopewell PC, Ponce de Leon A, Daley CL, et al. Transmission of Mycobacterium tuberculosis from patients smear-negative for acid-fast bacilli. Lancet 1999;353:444-9.
- World Health Organization Stop TB Partnership Childhood TB Subgroup. Chapter 4: childhood contact screening and management. Int J Tuberc Lung Dis 2007;11:12-15.
- De D, Kinikar A, Adhav P, Kamble S, Sahoo P, Koli H, et al. Source case investigation for children with TB disease in Pune, India. Tuberc Res Treat 2014;2014:182836.
- Smieja MJ, Marchetti CA, Cook DJ, Smaill FM. Isoniazid for preventing tuberculosis in non-HIV infected persons. Cochrane Database Syst Rev 2000;2:CD001363.
- van Soelen N, du Preez K, van Wyk SS, Mandalakas AM, Enarson DA, Reid AJ, et al. Does an isoniazid prophylaxis register improve tuberculosis contact management in South African children? PLoS One 2013;8:e80803.
- Bozkurt H, Musaonbasioglu S, Turkkanı MH, et al. T?berk?lozda koruyucu tedavi alanların değerlendirmesi. XXVI. Ulusal T?berk?loz ve G?ğ?s Hastalıkları Kongresi Bildiri ?zetleri Kitabı, 2011.
- Centers for Disease Control and Prevention. Updated guidelines for using interferon gamma release assays to detect Mycobacterium tuberculosis infection-United States, 2010. Morbidity and Mortality Weekly Report 2010;59:1-25.
- Chang KC, Leung CC, Tam CM. Household contact investigation of tuberculosis in low-income and middle-income countries: public-health impact. Lancet Infect Dis 2009;9:3-4.
- Jia Z, Cheng S, Ma Y, Zhang T, Bai L, Xu W, et al. Tuberculosis burden in China: a high prevalence of pulmonary tuberculosis in household contacts with and without symptoms. BMC Infect Dis 2014;14:64.
Yazışma Adresi (Address for Correspondence)
Dr. Aylin BABALIK
S?reyyapaşa G?ğ?s Hastalıkları ve
G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi,
G?ğ?s Hastalıkları Kliniği,
İSTANBUL - TURKEY
e-mail: aylinbabalik@gmail.com