LETTER TO EDITOR
Doi: 10.5578/tt.9050
Tuberk Toraks 2015;63(4):298-299

Homozigot metilen tetra hidro folat red?ktaz-677TT gen mutasyonu:
Pulmoner tromboemboli olgusu
G?listan KARADENİZ1, Serpil BULA? KIR1, Sibel DORUK1, ?zlem İNCE2, Dilek G?ND?Z2
1 Şifa ?niversitesi Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, İzmir, T?rkiye
1 Department of Chest Diseases, Faculty of Medicine, Sifa University, Izmir, Turkey
2 Şifa ?niversitesi Tıp Fak?ltesi, Radyoloji Anabilim Dalı, İzmir, T?rkiye
2 Department of Radiology, Faculty of Medicine, Sifa University, Izmir, Turkey
Pulmonary embolism is a life-threatening condition that needs prompt diagnosis and treatment in order to avoid advers outcomes. While the mortality rate of PE reaches up to 30% in untreated patients, this rate is reduced to 3% in treated patients (1). Thus, early diagnosis and treatment is crucial. Despite?treatment recurrence can be seen in 5-23% of the patients with venous thromboembolism (VTE) (2). However, recurrence is higher in cases with inherited thrombophilia (3). Genetic risk factors should be investigated in the following conditions; unexplained recurrent VTE before 40 years of age, presence of familial history according to VTE, patients with thrombosis in unusual areas, history of skin necrosis due to warfarin,? and presence the history of neonatal (4). The use of anticoagulants for longlife would be life saving in patients with PE who have genetic risk factors. Herein, we aimed to present a young male PE patient with homozygous methylenetetrahydrofolate reductase (MTHFR) 677TT mutation who presented with PE in the light of literature.
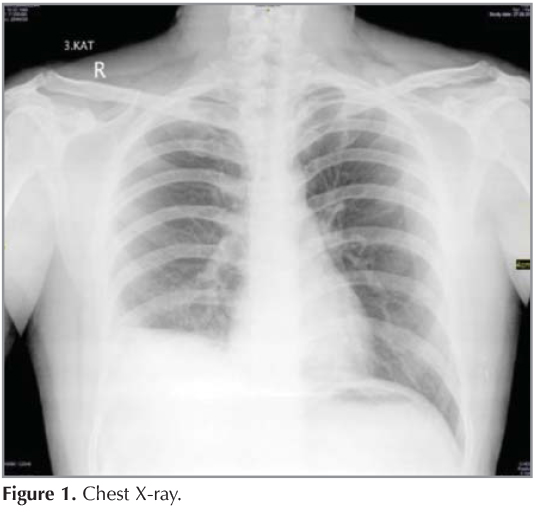
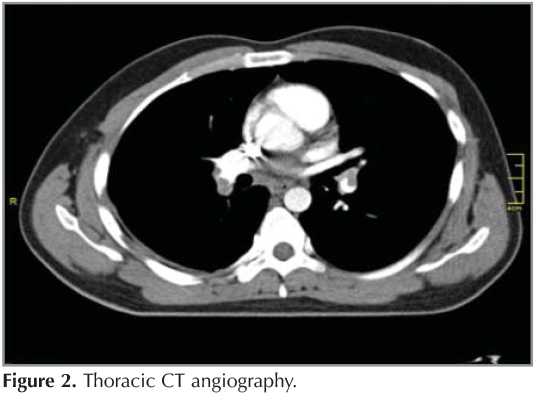
A twenty two-year-old male patient who was operated for ureteropelvic stenosis before 3 weeks, admitted to our clinic with the complaint of right flank pain.? Phsical examination other than the decreasing of the respiratory sound in the right lower lung fields were unremarkable. Chest X-ray revealed elevated right diaphragm and closed right costadiapfragmatic sinus (Figure 1). The level of d-dimer was 3.85 ug/mL in this patient with moderate clinical probabilitty.? Thoracic CT angiography was taken in order to rule out the PE. Thoracic CT showed filling defects in the bilateral lower, middle lobar and interlobar arteries consistent with thrombus, and minimal right pleural effusion (Figure 2). The anticoagulant therapy was started the patient with the absence of self and familial history. After the one month of the cessation of the anticoagulant therapy that was contiuned for 6 months, genetic screening of the patient according to possible causes of genetic factors homozygous MTHFR 677TT mutation was detected. Factor 5 Leiden and prothrombin 20210A mutations did not determined. The anti-thrombin activity was 99 (75-125), protein C activity was 119 (70-140), protein S activity was 74.8 (60-130). After the patient informed, coumadin prophylaxis was started.
Under forty years of age in patients with a history of venous thromboembolism genetic risk factors must be investigated. Although regional differences in prevalence, the most common hereditary risk factors are Factor 5 Leiden mutation, prothrombin 20210A mutation, the presence of antiphospholipid antibodies, anti-thrombin 3, protein C and protein S deficiency and hyperhomocysteinemia. Mutations in the MTHFR gene lead to reduces the MTHFR enzyme activity and this condition is resulted increasing in the plasma homocystein levels. High plasma homocystein levels are associated with the tendency to various cardiovascular advers outcomes (5). The most common mutations in the MTHFR gene are C677T ve A1298C.
Particularly, in the presence of homozygot 677TT mutation the enzyme activity is much lower, and this condition is associated with higher plasm homocystein and lower folate levels. The risk of venous and arterial thrombosis increases in these cases and lead to cardiovascular and cerebrovascular events at an early age, neural tube defects in pregnancy, and also lead to recurrent abortion and stillbirths.
Although, the previous studies and guidelines reported that hyperhomocysteinemia is commonly seen among the healthy subjects, and also was not a significant risk factor for PE. In recent years, studies have supported that homozygot MTHFR 677TT mutation is an important risk factor for venous thrombosis (6,7). Currently, there is a intense interest in studies related to the MTHFR mutations. In additon to VTE, MTHFR mutations are also investigated in neurological disorders, cardiovascular diseases, breast-lung and colorectal malignancies, in the presence of the recurrent abortions and neural tube defects.
In conclusion, patients who presented with PE at younger age should be evaluated genetic risk factors
REFERENCES
- Douketis JD, Kearon C, Bates S, Duku EK, Ginsberg JS. Risk of fatal pulmonary embolism in patients with treated venous thromboembolism. JAMA 1998;279:458-62.
- Heit JA, Mohr DN, Silverstein MD, Petterson MD, O'Fallon WM, Melton LJ. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med 2000;160:761-8.
- Cushman M. Epidemiology and risk factors for venous thrombosis. Semin Hematol 2007;44:62-9.
- Piazza G, Goldhaber SZ. Acute pulmonary embolism: Epidemiology and diagnosis. Circulation 2006;114:28-32.
- Jakubowski H. Pathophysiological consequences of homocysteine excess. J Nutr 2006;136:1741-9.
- Hotoleanu C, Trifa A, Popp R, Fodor D. The Importance of Homozygous Polymorphisms of Methylenetetrahydrofolate Reductase Gene in Romanian Patients with Idiopathic Venous Thromboembolism. Balkan Med J 2013;30:197-203.
- Moheimani F, Jackson DE. Venous thromboembolism: classification, risk factors, diagnosis, and management. ISRN Hematol 2011;2011:124610.
Yazışma Adresi (Address for Correspondence)
Dr. G?listan KARADENİZ
Şifa ?niversitesi Tıp Fak?ltesi,
G?ğ?s Hastalıkları Anabilim Dalı,
İZMİR - TURKEY
e-mail: drglstn35@gmail.com