RESEARCH ARTICLE
Doi: 10.5578/tt.8878
Tuberk Toraks 2015;63(4):250-256

Fagerstr?m nikotin bağımlılığı testinin T?rk?e versiyonunun psikometrik ?zellikleri
Mehmet Atilla UYSAL1, Derya ?ZTUNA2, Ayşe BAHADIR1, Aslı G?REK DİLEKTAŞLI3, ?ağatay KARŞIDAĞ4,
Aynur HOROZ5, Sinem İLİAZ1
1 Yedikule G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği, İstanbul, T?rkiye
1 Clinic of Chest Diseases, Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey
2 Ankara ?niversitesi Tıp Fak?ltesi, Biyoistatistik Anabilim Dalı, Ankara, T?rkiye
2 Department of Biostatistics, Faculty of Medicine, Ankara University, Ankara, Turkey
3 Uludağ ?niversitesi Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, Bursa, T?rkiye
3 Department of Chest Diseases, Faculty of Medicine, Uludag University, Bursa, Turkey
4 Bakırk?y Prof. Dr. Mazhar Osman Ruh ve Sinir Hastalıkları Eğitim ve Araştırma Hastanesi, Psikiyatri Kliniği,
İstanbul, T?rkiye
4 Clinic of Psychiatry, Bakirkoy Prof. Dr. Mazhar Osman Mental Health and Neurological Diseases Training and
Research Hospital, Istanbul, Turkey
5 Okmeydanı Eğitim ve Araştırma Hastanesi, Sigara Bırakma Kliniği, İstanbul, T?rkiye
5 Clinic of Quit Smoking, Okmeydani Training and Research Hospital, Istanbul, Turkey
?ZET
Fagerstr?m nikotin bağımlılığı testinin T?rk?e versiyonunun psikometrik ?zellikleri
Giriş: Fagerstr?m Nikotin Bağımlılığı Testi (FNBT) Fagerstr?m Tolerans Anketinden uyarlanmıştır ve sigara i?icisinin sigarayı bırakmaya ?alışırken nikotin yerine koyma tedavisine ihtiyacını değerlendirmek i?in kullanılır. FNBT pek ?ok dile ?evrilmiş ve d?nya ?apında sigara literat?r?nde yer almıştır. Ancak ?ok az sayıda ?alışmada İngilizce olmayan FTND versiyonlarının psikometrik ?zellikleri araştırılmıştır. Bu ?alışma FTND'nin T?rk?e versiyonunun psikometrik ?zelliklerini değerlendirmeyi ama?lamıştır.
Materyal ve Metod: Doğrulama faktor analizi (DFA) ile anketin T?rk?e versiyonunun fakt?riyel yapısı İstanbul, T?rkiye'de bulunan iki b?y?k sigara bırakma polikliniğindeki b?y?k bir ?rneklem grubu kullanılarak değerlendirilmiştir. ?alışmamız, 1 Ekim ve 31 Aralık 2011 tarihleri arasında bu sigara bırakma polikliniklerinden birine başvuran 502 sigara i?icisinden oluşmaktadır. B?t?n katılımcılar ?alışma i?in aydınlatılmış onam vermiştir. FNBT'nin ge?erliliğini ?l?mek i?in DFA y?ntemi kullanıldı ve g?venilirliği belirlemek i?in Cronbach's alpha katsayısı hesaplandı.
Bulgular: Bir fakt?rl? DFA FNBT'deki t?m bileşenlerden oluşmaktadır. Bu fakt?rdeki t?m bileşenler 0.40 ve ?zerinde puan almıştır. Uyum istatistikleri yeterliydi ve karşılaştırmalı uyum indeksi (CFI) = 0.922, Tucker-Lewis İndeksi (TLI) = 0.902 ve k?k ortalama yaklaşım hatası (RMSEA) = 0.081 idi.? İki fakt?rl? DFA, birinci factor olarak sabah i?iciliğiyle ilgili 3 bileşenden ve ikinci factor olarak i?icilik ?zelliğiyle ilgili ?? bileşenden oluşmaktadır. Fakt?r değerleri ve uyumun iyiliği istatistikleri FNBT'nin iki fakt?rl? yapısını doğrulamıştır.
Sonu?: Değerlendirme FNBT'nin T?rk?e versiyonunun iki fakt?rl? yapısı olduğunu orta derece g?venilirlikle doğrulamıştır. Bu ?alışma g?stermiştir ki; nikotin bağımlılığının tahmini i?in toplam skoru kullanmak, spesifik sigara bağımlılığını değerlendirmeyi ve tedavi ve m?dahaleleri buna g?re bi?imlendirmeyi engelleyebilir. İki fakt?rl? bir FNBT'nin hastaların nikotin bağımlılığını daha doğru olarak belirleyebileceğini d?ş?n?yoruz.
Anahtar kelimeler: Nikotin, t?t?n kullanım bozukluğu, analiz, fakt?r
SUMMARY
Psychometric properties of the Turkish version of the Fagerstr?m test for nicotine dependence
Introduction: The Fagerstr?m Test for Nicotine Dependence (FTND), modified from Fagerstr?m Tolerance Questionnairre (FTQ), is used to determine whether a smoker trying to quit will need nicotine replacement therapy to treat with drawal symptoms. The FTND has been translated into many languages and has been referred to in the smoking literature worldwide. However, only a few studies have examined the psychometric propertiesof the non-English FTND versions. This study aimed to assess the psychometric properties of the Turkish version of the FTND.
Materials and Methods: Confirmatory factor analysis (CFA) was used to test the factor structure of the Turkish version of the questionnaire using a large sample from two smoking cessation clinics in Istanbul, Turkey. Our study comprised 502 smokers who entered one of these smoking cessation clinics between October 1 and December 31, 2011. All subjects gave informed consent to the study. We assessed the validity of the FTND using CFA, and we calculated Cronbach's alpha coefficients to determine reliability.
Results: One-factor CFA included all of the items on the FTND. All items loaded on this factor with a score of 0.40 or higher. The goodness of fit statistics were adequate, with a Comparative Fit Index (CFI) of 0.922, a Tucker-Lewis Index (TLI) of 0.902, and a root-mean-square error of approximation (RMSEA) of 0.081. Two-factor CFA comprised the three "morning smoking" items, and the three "smoking pattern" items. The factor loadings and the goodness-of-fit statistics confirmed that the FTND has a two-factor structure.
Conclusions: Analyses confirmed that the Turkish version of the FTND has a two-factor structure with moderate reliability. This study found that using a total score as an estimate of nicotine dependence may limit the assessment of specific smoking dependency and tailoring intervention approaches. We suggest that a two-factor FTND in clinical practice would more accurately determine the nicotine dependence of patients.
Key words: Nicotine, tobacco use disorder, analysis, factor
INTRODUCTION
Smoking cigarettes remains a top cause of avoidable disease (cancer, cardiovascular disease) and premature death in most countries (1). The prevalence of cigarette smoking within developed countries has decreased significantly in recent decades, but developing nations are experiencing the opposite. Research shows that by 2030, 80% of tobacco-related deaths will occur in developing nations. Therefore, both prevention and quitting smoking are crucial goals for public health policy in these nations (2).
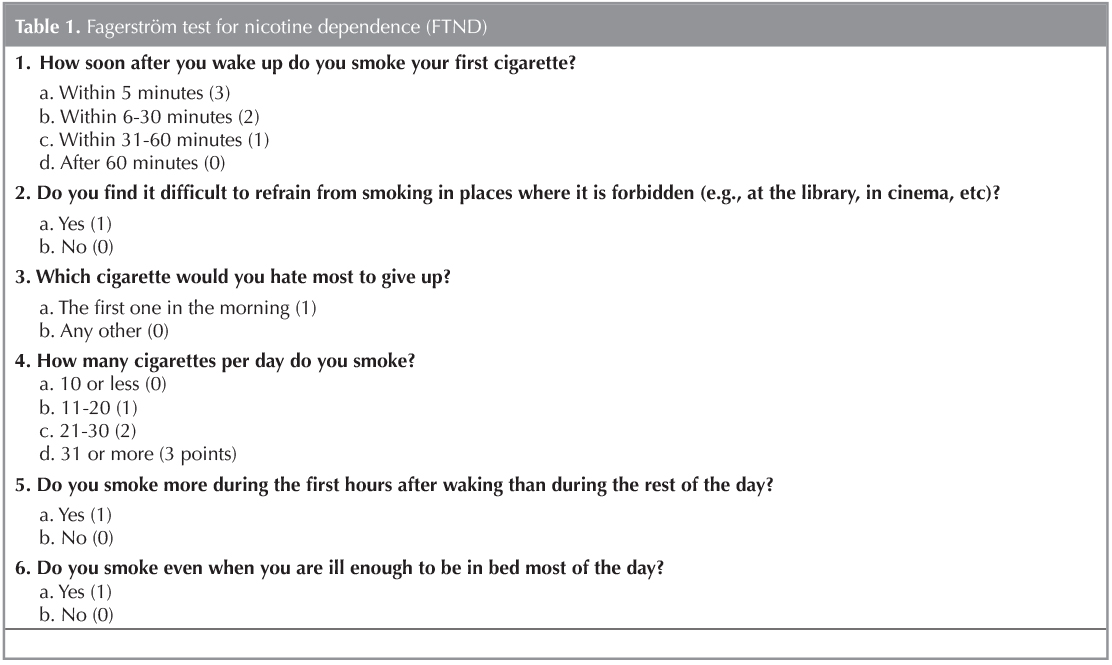
The Fagerstr?m Test for Nicotine Dependence (FTND), modified from Fagerstr?m Tolerance Questionnairre (FTQ), was developed by Heatherton et al. to determine whether a smoker trying to quit will need nicotine replacement therapy to treat withdrawal symptoms (3,4). This easy tool comprises six easily understood questions that can be rapidly applied. Healthcare workers use scores from this tool to classify nicotine dependence? according to a 10-point scale: very low (0 to 2 points), low (3 to 4 points), moderate (5 points), high (6 to 7 points), or very high (8 to 10 points) (Table 1) (5).
The FTND has been adapted globally as a measure of physical dependence on nicotine, specifically cigarette use, due to its ease of understanding and rapidity of application (6). The instrument's validity and reliability have been assessed in a variety of cultural settings (7,8,9,10,11,12).
The FTND has been translated into many languages and has been referred to in the smoking literature targeted toward English-and non-English-speaking populations worldwide. However, only a few studies have examined the psychometric properties of the non-English FTND versions specifically, the Chinese, French, Japanese, Korean, Spanish, and Turkish versions (7,8,9,13,14,15,16).
When the FTND was introduced, the authors used an exploratory factor analysis (EFA) to recommend a unidimensional structure, but more recent factor analytic research has proven this scale to have an unstable factor solution (4,5,13,17). Researchers using EFA and confirmatory factor analysis (CFA) of the FTND have proven that one question how soon after you wake up do you smoke your first cigarette? loads on two factors (morning smoking and daytime smoking) (18,19).
Authors in a 2009 study using CFA found that a one-factor model consisting of the items from the Smoking Pattern factor from the EFA provided an excellent fit with the data. Thus, the unidimensional structure of the the six-item has not been effectively replicated in subsequent studies using heterogeneous groups of smokers (10).
Uysal MA et al. conducted the first study of the Turkish version of the FTND (8). They employed EFA using principal components with no rotation and found the instrument to be unidimensional.
Radzius et al., in contrast, recommended two factors: Factor 1 they named the "morning smoking pattern", and Factor 2 they defined as "smoking pattern" (18). They discovered that items 1, 3, and 5 loaded on Factor 1, which assesses the degree of urgency to restore nicotine levels to a given threshold after nighttime. Items 2, 4, and 6 loaded on Factor 2, which reflects the persistence with which smokers maintain nicotine concentrations during waking hours.
In light of these conflicting findings, we aimed to analyze the structure the Turkish version of the FTND using CFA to determine whether the one- or two-factor structure was more appropriate.
Materials and methods
Design and Setting
The data analyzed in this study were collected from two big smoking cessation clinics in Istanbul, Turkey.
Participants
Our study comprised 502 smokers who entered one of these smoking cessation clinics between October 1 and December 31, 2011. All participants met the following criteria: (a) they were self-identified as current, regular, daily smokers; (b) they expected to quit smoking; and (c) they understood and could answer the questions themselves, and they completed the FTND.
Statistical Analysis
We assessed the validity of the FTND using CFA, and we calculated Cronbach's alpha coefficients to determine reliability.
Construct validity: Studies assessing the validity of the FTND have shown inconsistent results. To assess whether the data would fit either a factorial or a two-factorial model (while Item 1, 3 and 5 formed the first factor, Item 2, 4 and 6 formed the second factor), we applied CFA with a weighted least squares estimation with robust standard errors and mean- and variance-adjusted (WLSM) χ2 statistics for categorical data. Items with factor loadings below 0.40 were eliminated. The following goodness-of-fit indices were used to assess the degree of fit: the Comparative Fit Index (CFI; > 0.90 acceptable, > 0.95 excellent), the Tucker-Lewis Index (TLI; > 0.90 acceptable, > 0.95 excellent), and root-mean-square error of approximation (RMSEA; < 0.08 acceptable, < 0.05 excellent) (20).
Reliability: The most common form of reliability for a Likert-type scale, such as the FTND, is internal consistency, which can be tested using Cronbach's alpha coefficients. A Cronbach's alpha value between 0.7 and 0.8 is considered "acceptable" reliability, but studies have shown that a large number of items in a scale can artificially inflate the value of alpha (21,22).
Data were analyzed using the Statistical Package for the Social Sciences (SPSS for windows ver. 11.5, SPSS Inc., Chicago, USA and MPLUS ver. 6.11, Los Angeles, CA, USA.)
Results
A total of 541 patient files were screened for inclusion in the study. Of those, 39 patients were omitted due to missing data. Our final sample data consisted of 502 patients with a mean ? standard deviation age of 42 ? 11. The average number of years the participants had smoked was 23.6 ? 10.4, with an average number of cigarettes smoked per day of 25 ? 11.
Confirmatory Factor Analysis
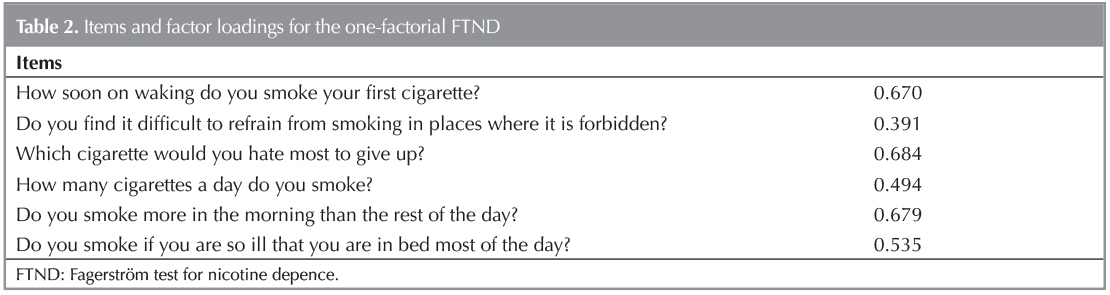
We first ran a one-factor CFA that included all of the items on the FTND. All items loaded on this factor with a score of 0.40 or higher (Table 2). The goodness of fit statistics were adequate, with a CFI of 0.922, a TLI of 0.902, and a RMSEA of 0.081.
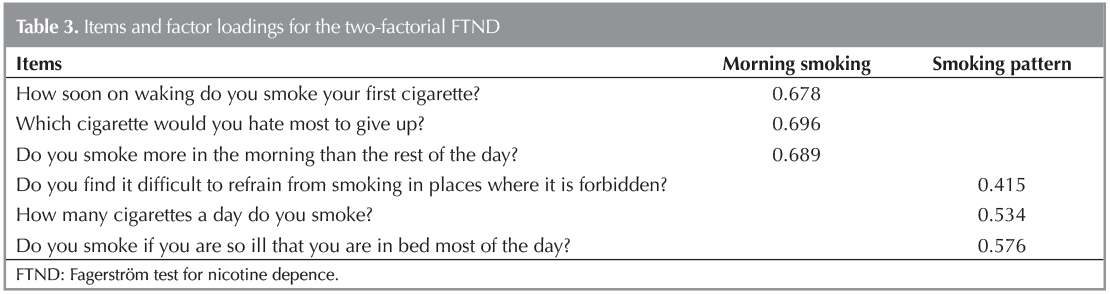
We next ran a two-factor CFA. The first factor comprised the three "morning smoking" items (questions 1, 3, and 5), and the second, the three "smoking pattern" items (questions 2, 4, and 6). The factor loadings and the goodness-of-fit statistics confirmed that the FTND has a two-factor structure. Table 3 shows a high correlation (r= 0.871) between the two factors. The items in the two factors loaded at 0.42 or higher. The data showed a reasonable fit to the model, with CFI= 0.927, TLI= 0.895, and RMSEA= 0.084.
Reliability
In regard to reliability of the one-factorial FTND, we found a Cronbach's alpha of 0.586. In addition, the internal consistency of the FTND was not adequate at this factor level, with Cronbach's alphas of 0.455 and 0.336 for the morning smoking and smoking pattern factors, respectively.
Discussion
Our analysis of the Turkish version of the FTND confirms the previously proposed two-factor model. Table 2 illustrates that the first factor is characterized by questions involving morning smoking (Q1, Q3, and Q5). These questions clearly assess the urgency to restore nicotine levels after nighttime abstinence. The second factor, determined by questions 2, 4, and 6, appears to measure daytime smoking patterns and has been interpreted as measuring the persistence with which nicotine levels are maintained throughout waking hours (18). Consistent with Payne et al., Burling et al. and Radzius et al., we found the following factors: Factor 1 [(morning smoking (Q1, 3, 5)] and Factor 2 [Smoking Pattern (Q2, 4, 6)] (5,18,23).
A recent systematic review examined the bi-factorial structure of the FTND and observed small differences among the questions that compose the factors (24). The two factors revealed from the promax rotation showed two distinguishable and correlated domains of nicotine dependence, which lends further support to a construct of nicotine dependence that manifests itself by urgency of use and maintenance of nicotine levels (11).
A recent systematic review examined the bi-factorial structure of the FTND and observed small differences among the questions that compose the factors (24). The two factors revealed from the promax rotation indicated two distinguishable and correlated domains of nicotine dependence, which offers further support to a construct of nicotine dependence that manifests itself through urgency of use and maintenance of nicotine levels (11).
Although some previous studies have reported that question 1-How soon do you smoke your first cigarette after you wake up?-is loaded on both factors, we found this question to be only loaded on Factor 1 (10).
Our study had a sufficient sample size for modeling categorical data using CFA (n= 502) and was within the recommended range for Mplus software. The size and direction of the estimated parameters goodness of fit measures were consistent with previous FTND research, which provides further support for the use of our two-factor modeling strategy.
Our results support the reliability of the Turkish version of the FTND. The internal consistency of the Cronbach's alpha score was low (58) and did not reach the standard Cronbach's alpha threshold of ≥ 0.80 (25). However, these results are consistent with Meneses-Gaya et al. systematic review, which supports the usefulness of the test in clinical settings (24). The authors reported that the internal consistency of the FTND ranged from 0.55 to 0.74, indicating that the FTND had moderate internal consistency.
While reliability of the Spanish version FTND has been reported to be similar to that of our study, the French and the Dutch versions of the FTND have been found to have higher reliability (7,13,26). We therefore suggest that the moderate reliability measures might be a consequence of cultural variances that affect nicotine dependence among populations in different countries.
Because the FTND includes measures of daily consumption, it may not be ideal for cross-cultural comparisons where the cost and affordability of tobacco differs substantially, or over time as tobacco prices change, or in comparisons between racial groups with varied rates of nicotine metabolism (27). Furthermore, because the instrument does not measure withdrawal or indicate what areas of addiction are troublesome? for an individual, patients' responses are not particularly helpful for modifying the content of? smoking cessation counseling (28,29,30).
The previously reported issues with the FTND (e.g.,? low reliability) may be partially due to the instrument's forced-choice response format. Radzius et al. indicated that the FTND questions that require a "yes" or "no" forced-response may not reflect "true dichotomies," suggesting that these questions may have a normal distribution of thresholds in which smoker's can respond, thereby reflecting a dimensional construct (18).
?Another area of concern is the high correlation that we found between the two factors, consistent with prior studies (9,18,19). It showed the complex structure of FTND again.
This study has a few limitations and disadvantages. First, our sample comprised smokers who wanted to quit. Although the FTND asks smokers to report reasonably objective information about long-term smoking patterns, the fact that these smokers were in withdrawal may have influenced the participants' responses to the items.
Our results are not representative of the full smoking population in Turkey. All single sample studies are similarly limited in their generalizability, but our study is the first multicenter study to evaluate the psychometric properties of the Turkish version of the FTND.
Prior research also indicates that the FTND has limited use in predicting smoking-related outcomes, such as changes in smoking behavior over time or the ability to detect the biochemical markers of smoking dependence (13).
We suggest that the Turkish version of the FTND must be used carefully. Measurement error can occur if a simple scoring method is used to combine the six items on the FTND into a single overall score. For instance, subjects can score higher on one dimension and lower on the other, producing an average for the two factors that might not adequately reflect a smoker's dependency. In clinical practice, this lack of dimension-specific scoring can limit the usefulness of the scale when attempting to adjust interventions to match specific dependence profiles. This increasing evidence of a consistent two-factor structure across several languages, cultures, and different samples supports our assertion that the results of this study can be generalized.
Therefore, we conclude that the Turkish version of the FTND is useful for assessing nicotine dependence among smokers at smoking cessation clinics. When used appropriately with an awareness of this two-factor dimensionality, the FTND can provide clinically valuable information that can help determine patients' nicotine dependence.
REFERENCES
- 2010 Surgeon General's Report How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease. Accesed date: 2013 July 5. Available from: http://www.cdc.gov/tobacco/data_statistics/sgr/2010/.
- Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006;3:e442.
- Fagerstrom KO. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addict Behav 1978;3:235-41.
- Heatherton TF, Kowloski KL, Frecker RC, Fagerstr?m KO. The fagerstrom test for nicotine dependence: a revision of the fagerstrom tolerance questionnaire. Br J Addict 1991;86:1119-27.
- Payne TJ, Smith PO, McCracken LM, McSherry WC, Antony MM. Assessing nicotine dependence: a comparison of the Fagerstrom Tolerance Questionnaire (FTQ) with the Fagerstrom Test for Nicotine Dependence (FTND) in a clinical sample. Addict Behav 1994;19:307-17.
- Fagerstrom K, Russ C, Yu CR, Yunis C, Foulds J. The Fagerstrom Test for Nicotine Dependence as a predictor of smoking abstinence: a pooled analysis of varenicline clinical trial data. Nicotine Tob Res 2012;14:1467-73.
- Becona E, Vazquez FL. The Fagerstrom test for nicotine dependence in a spanish sample. Psychol Rep 1998; 83:1455-8.
- Uysal MA, Kadakal F, Karsidag C, Bayram NG, Uysal O, Yilmaz V. Fagerstrom test for nicotine dependence: reliability in a Turkish sample and factor analysis. Tuberk Toraks 2004;52:115-21.
- Huang CL, Lin HH, Wang HH. The psychometric properties of the Chinese version of the Fagerstrom Test for Nicotine Dependence. Addict Behav 2006;31:2324-7.
- de Meneses-Gaya C, Zuardi AW, de Azevedo Marques JM, Souza RM, Loureiro SR, Crippa JA. Psychometric qualities of the Brazilian versions of the Fagerstrom Test for Nicotine Dependence and the Heaviness of Smoking Index. Nicotine Tob Res 2009;11:1160-5.
- Jhanjee S, Sethi H. The Fagerstrom test for nicotine dependence in an Indian sample of daily smokers with poly drug use. Nicotine Tob Res 2010;12:1162-6.
- Korte KJ, Capron DW, Zvolensky M, Schmidt NB. The Fagerstrom test for nicotine dependence: do revisions in the item scoring enhance the psychometric properties? Addict Behav 2013;38:1757-63.
- Etter JF, Duc TV, Perneger TV. Validity of the Fagerstrom test for nicotine dependence and of the Heaviness of Smoking Index among relatively light smokers. Addiction 1999;94:269-81.
- Chabrol H, Niezborala M, Chastan E, de Leon J. Comparison of the Heavy Smoking Index and of the Fagerstrom Test for Nicotine Dependence in a sample of 749 cigarette smokers. Addict Behav 2005;30:1474-7.
- Mikami I, Akechi T, Kugaya A, Okuyama T, Nakano T, Okamura H, et al. Screening for nicotine dependence among smoking-related cancer patients. Jpn J Cancer Res 1999;90:1071-5.
- Park SM, Son KY, Lee YJ, Lee HC, Kang JH, Lee YJ, et al. A preliminary investigation of early smoking initiation and nicotine dependence in Korean adults. Drug Alcohol Depend 2004;74:197-203.
- Haddock CK, Lando H, Klesges RC, Talcott GW, Renaud EA. A study of the psychometric and predictive properties of the Fagerstrom Test for Nicotine Dependence in a population of young smokers.? Nicotine Tob Res 1999;1:59-66.
- Radzius A, Gallo JJ, Epstein DH, Gorelick DA, Cadet JL, Uhl GE, et al. A factor analysis of the Fagerstrom Test for Nicotine Dependence (FTND).? Nicotine Tob Res 2003;5:255-60.
- Richardson CG, Ratner PA. A confirmatory factor analysis of the Fagerstrom Test for Nicotine Dependence. Addict Behav 2005;30:697-709.
- Pai AL, Mullins LL, Drotar D, Burant C, Wagner J, Chaney JM. Exploratory and confirmatory factor analysis of the Child Uncertainty in Illness Scale among children with chronic illness. J Pediatr Psychol 2007;32:288-96.
- Kline P. A handbook of test construction: Introduction to psychometric design. 1st ed. New York, USA: Methuen, 1986:259.
- Cortina JM. What is coefficient alpha? An examination of theory and applications.? Journal of Applied Psychology 1993;78:98-104.
- Burling AS, Burling TA. A comparison of self-report measures of nicotine dependence among male drug/alcohol-dependent cigarette smokers. Nicotine Tob Res 2003;5:625-33.
- Meneses-Gaya IC, Zuardi AW, Loureiro SR, Crippa JA. Psychometric properties of the Fagerstrom Test for Nicotine Dependence. J Bras Pneumol 2009;35:73-82.
- Nunnally JC BI. Psychometric Theory. 3rd ed. New York, USA: McGraw-Hill, 1994:248-92.
- Vink JM, Willemsen G, Beem AL, Boomsma DI. The Fagerstrom Test for Nicotine Dependence in a Dutch sample of daily smokers and ex-smokers. Addict Behav 2005;30:575-9.
- Perez-Rios M, Santiago-Perez MI, Alonso B, Malvar A, Hervada X, de Leon J. Fagerstrom test for nicotine dependence vs heavy smoking index in a general population survey. BMC Public Health 2009;9:493.
- Contreras KR, Kominiarek MA, Zollinger TW. The impact of tobacco smoking on perinatal outcome among patients with gestational diabetes. J Perinatol 2010;30:319-23.
- Difranza JR, Savageau JA, Wellman RJ. A comparison of the autonomy over tobacco scale and the Fagerstrom test for nicotine dependence. Addict Behav 2012;37:856-61.
- Kassim S, Salam M, Croucher R. Validity and reliability of the Fagerstrom Test for Cigarette Dependence in a sample of Arabic speaking UK-resident Yemeni khat chewers. Asian Pac J Cancer Prev 2012;13:1285-8.
Yazışma Adresi (Address for Correspondence)
Dr. Mehmet Atilla UYSAL
Yedikule G?ğ?s Hastalıkları ve G?ğ?s Cerrahisi
Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği, ?
İSTANBUL-TURKEY
e-mail: dratilla@me.com