LETTER TO THE EDITOR
Doi: 10.5578/tt.7841
Tuberk Toraks 2015;63(1):67-70

Tekrarlayan pn?moninin nadir bir sebebi: FMF
Hikmet ?OBAN1, Hasan D?ZENL?1
1 Sakarya E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? Klini?i, Sakarya, T?rkiye
1 Clinic of Chest Diseases, Sakarya Training and Research Hospital, Sakarya, Turkey
INTRODUCTION
Recurrent pneumonia is a condition characterized by fever, infiltrative lesion and leukocytosis experienced at least twice in a year by the same patient. At least a one-month interval following the recovery between two episodes is necessary in order to distinguish slow-resolving pneumonias from this group (1). The most common causes in the unilateral liver lobe include foreign material aspiration, malignancy, bronchiectasis, sequestration, bronchogenic cyst and lymph node pressure. In multiple node involvement, the causes include central nervous system diseases, antibody and complement failure, cystic fibrosis, primary ciliary dyskinesia, asthma, ABPA and diabetes mellitus (2).
CASE REPORT
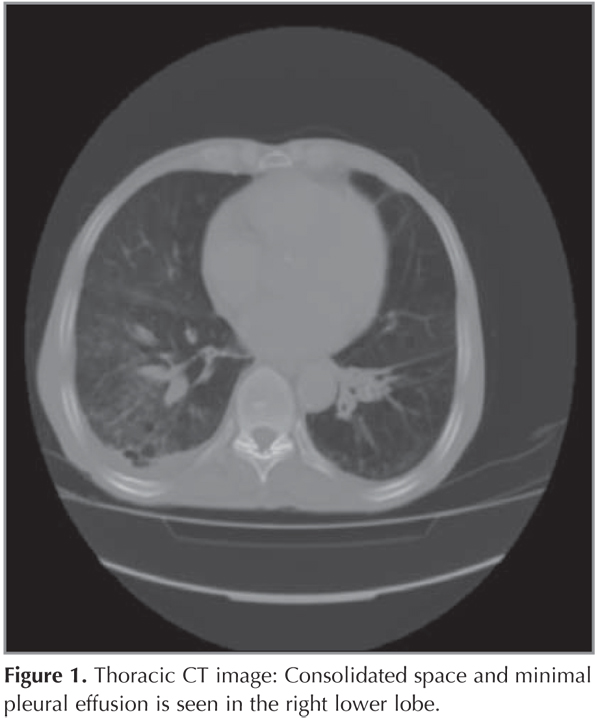
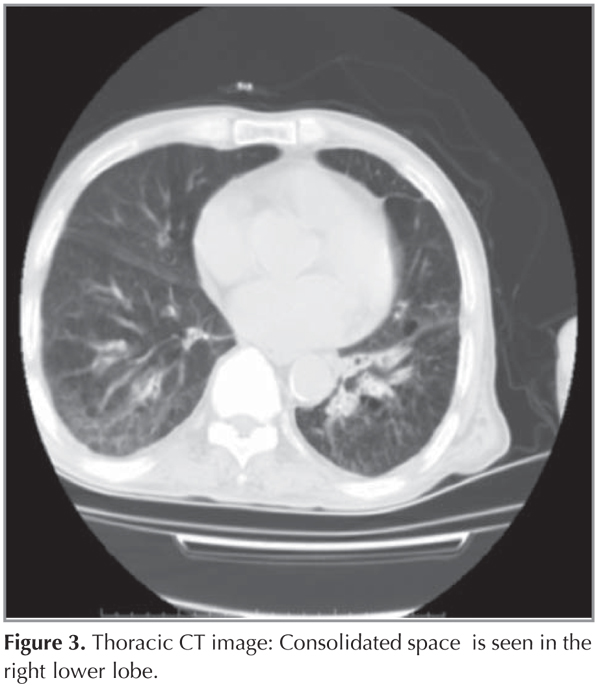
The 80-year-old male patient first presented in August 2010 with fever, abdominal pain and difficulty in breathing. His medical history included chronic anemia. The patient had undergone upper and lower gastrointestinal endoscopy to investigate the etiology of anemia and abdominal pain. The patient was diagnosed with diminutive polyp and non-specific colitis. On examination, he had bilateral rales. Laboratory analyses demonstrated leukocytosis, anemia and hypoxia. The patient was admitted for inpatient care due to bronchopneumonia and minimal pleurisy (right) and, following antibiotherapy, clinical improvement was achieved and he was discharged (Thoracic CT is provided in Figure 1). In March 2011, the patient was treated for the same complaints and similar laboratory results. At both hospitalizations, phlegm cultures and phlegm ARRB were tested negative. Bronchoscopy was performed due to recurrent pneumonia. No intrabronchial lesions were detected. Bronchial lavage culture, AARB and cytology results were also negative. ECHO showed EF: 55%, mild-moderate mitral valve failure (MF) and mild aortic valve failure (AF). The patient was discharged with clinical and radiological response post-antibiotherapy (Thoracic CT is provided in Figure 2). In October 2012, the patient was hospitalized once again for similar clinical, radiological and laboratory findings. pANCA, cANCA, ANA, anti-ds DNA, immunoglobulin and complement levels were normal. Responses to fever and leukocyte treatment were achieved after 48 hours and the patient was discharged (Thoracic CT is provided in Figure 3). In November 2012, the patient presented with the same symptoms. Haemogram and biochemistry results were normal. Chest radiography demonstrated bilateral minimal pleurisy with no parenchymal pneumonic infiltration. Colonoscopy was performed to investigate nausea, vomiting and abdominal pain. Mucosal biopsy results were consistent with colitis. Protein electrophoresis and glucose 6 phosphate dehydrogenase enzyme activity results were normal. Homozygous m694v was positive in gene mutation analysis. Colchicine treatment was started with dose titration. Colon biopsy was studied for amyloid and was negative.

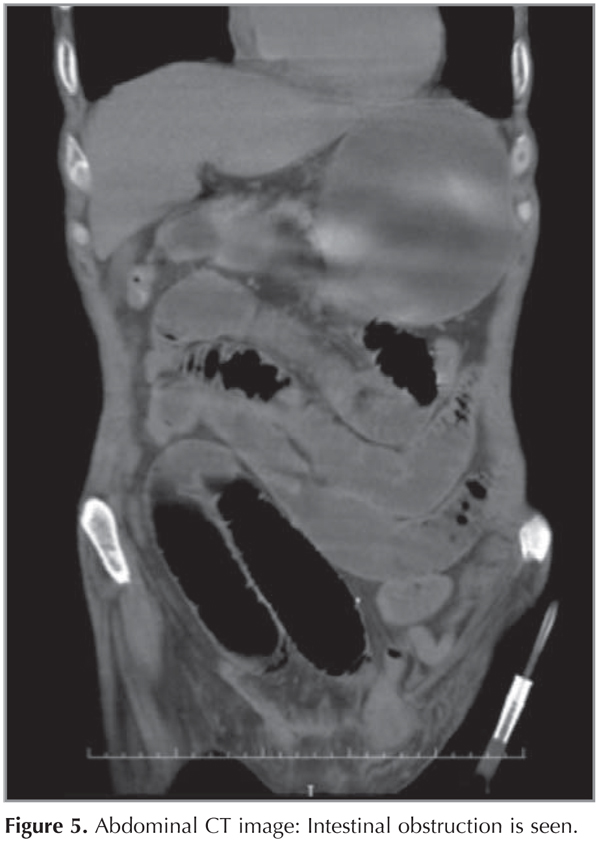
At week 2 of the medical treatment, the patient presented to the emergency unit with abdominal pain, fever, weakness, impaired consciousness and severe hypoxia. Chest radiography demonstrated diffuse infiltrations bilaterally (Figure 4). The patient, under intensive care, developed sudden deterioration in urea, creatinine, AST and ALT values. These were suspected to be the side effects of colchicineand therefore the drug was discontinued. After clinical and radiological improvements were achieved, the patient was transferred to the clinic but he developed sudden abdominal pain, nausea and vomiting in January 2013. Abdominal CT demonstrated ileus, and the patient was operated (Figure 5). Colchicine was reintroduced and no pneumonia episodes were observed after treatment with colchicine. Post-treatment follow-up pulmonary X-ray is provided in Figure 6.


DISCUSSION
Familial Mediterranean fever is an autosomal recessively inherited autoimmune disorder with unknown pathogenesis most commonly seen in the Jews, Arabs, Armenians and Turks. Clinically, the disorder presents with abdominal pain with fever, chest pain, joint pain and erysipelas-like rash which last for 12-96 hours and are self-limiting. Amyloidosis is the most serious complication. It is primarily a childhood disease (3). FMF is observed below 20 years of age in 80% of the cases and is diagnosed very rarely above 40 years. In Turkey, the incidence of FMF in individuals above 40 years of age is 0.5% of all FMF patients (4).
The most common pulmonary manifestation of FMF is plevral involvement between acute episodes. When systemic amyloidosis develops, amyloid accumulation may occur in the lungs. Mesothelioma and pulmonary hemorrhage secondary to vasculitis have also been reported (5). The patient we present here is the first case of recurrent pneumonias, where control over pneumonia attacks could be achieved with colchicine treatment. The patient has been suffering from abdominal pain for the past 5 years. He had had 4 episodes of pneumonia during the last 2 years. Arthritis and erythema is less common in adult FMF patients and it has been described that the adult form may have different clinical characteristic (6). Recurrent pneumonias may be a feature of the adult form.
The FMF gene (MEFV) was identified in the chromosome 16 p arm in 1997 and gene mutations associated with the disease have been reported (4). M694V mutation has been reported frequently from studies conducted in Turkey (7). The Turkish FMF Working Group has demonstrated close link between the M694V mutation and disease severity (8). Homozygous m694v mutation was identified in our patient. Homozygous m694v mutation was also found in the patient's 44-year-old son who was non-symptomatic other than abdominal pain.
Almost 95% of the patients with FMF have peritoneal involvement and acute abdominal pain may present a significant problem. It may lead to unnecessary laparotomies due to false diagnosis of appendicitis. Recurrent peritonitis may lead to intestinal obstruction due to intra-abdominal tissue attachment (9,10). Our patient developed acute abdominal pain, vomiting and nausea. Ileus was corrected with surgery. It should also be borne in mind that intestinal obstruction may develop under colchicine treatment (10).
CONCLUSION
Because FMF is an autoimmune disorder, it should be taken into account that the patients may be predisposed to infection and may lead to recurrent pneumonias in patients whose diagnoses have been delayed.
CONFLICT of INTEREST
None declared.
Geli? Tarihi/Received: 04.06.2014 • Kabul Edili? Tarihi/Accepted: 15.07.2014
REFERENCES
- Guidelines for the initial management of adults with community acquired pneumonia: Diagnosis, assessment of severity and initial antibiotic therapy. Am Rev Respir Dis 1993;148;1418-26.
- Savas I. Slow decline, unresolved, and recurrent pneumonia. Turk Thor J 2000;1(3):81-6.
- Shohat M, Halpern GJ. Familial Mediterranean fever--a review. Genet Med 2011;13(6):487-98.
- Sayarlioglu M, Cefle A, Inanc M, Kamali S, Dalkilic E, Gul A, et al. Characteristics of patients with adult-onset familial Mediterranean fever in Turkey: analysis of 401 cases. Int J Clin Pract 2005;59:202-5.
- Lidar M, Pras M, Langevitz P, Livneh A. Thoracic and lung involvement in familial Mediterranean fever (FMF). Clin Chest Med 2002;23(2):505-11.
- The French FMF Consortium. A candidate gene for familial mediterranean fever. Nat Genet 1997;17:25-31.
- Etem E, Deveci S, Erol D, Yuce H, Elyas H. Familial Mediterranean Fever: A Retrospective Clinical and Molecular Study in the East of Anatolia Region of Turkey. Open Rheumatol J 2010;4:1-6.
- The Turkish FMF Study Group. Familial Mediterranean Fever (FMF) in Turkey: The results of a nationwide multicenter study. Medicine (Baltimore) 2005;84:1-11.
- Sohar E, Gafni J, Pras M, Heller H. Familial Mediterranean fever. A survey of 470 cases and review of the literature. Am J Med 1967;43:227-53.
- Kaya B, Eris C, Uctum B. Delay in Diagnosis of Intestinal Obstruction in a Patient with Familial Mediterranean Fever. Clin Med Insights Case Rep 2010;3:59-62.
Yaz??ma Adresi (Address for Correspondence)
Dr. Hikmet ?OBAN
Sakarya E?itim ve Ara?t?rma Hastanesi,
G???s Hastal?klar? Klini?i,
SAKARYA - TURKEY
e-mail: hikmetcoban04@gmail.com