REVIEW
Doi: 10.5578/tt.8378
Tuberk Toraks 2015;63(1):53-59

Obstr?ktif uyku apne sendromu olan hastalarda perioperatif de?erlendirme
Mustafa ??RT?K1, Kemal K?RAZ2, Abdurrahman S?NMEZLER3, Selahattin AKYOL4
1 Adana Numune E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? ve T?berk?loz B?l?m?, Adana, T?rkiye
1 Department of Pulmonology, Adana Numune Training and Research Hospital, Adana, Turkey
2 Antalya E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? ve T?berk?loz B?l?m?, Antalya, T?rkiye
2 Department of Pulmonology, Antalya Training and Research Hospital, Antalya, Turkey
3 Adana Numune E?itim ve Ara?t?rma Hastanesi, N?roloji B?l?m?, Adana, T?rkiye
3 Department of Neurology, Adana Numune Training and Research Hospital, Adana, Turkey
4 Adana Numune E?itim ve Ara?t?rma Hastanesi, Kardiyoloji B?l?m?, Adana, T?rkiye
4 Department of Cardiology, Adana Numune Training and Research Hospital, Adana, Turkey
?ZET
Obstr?ktif uyku apne sendromu olan hastalarda perioperatif de?erlendirme
Obstr?ktif uyku apne sendromu son y?llarda daha s?k tan? koyulan ve ?nemi giderek daha iyi anla??lan yayg?n bir sa?l?k problemidir. Bu sendroma s?kl?kla obezite e?lik eder. Obstr?ktif uyku apne sendromunda hipoksi ve bazen de ek olarak hiperkarbi oldu?u, yine bu hasta grubunda kardiyovask?ler problemlerin di?er ki?ilere g?re daha s?k oldu?u bilinmektedir. ?nvaziv i?lemler s?ras?nda hastaya uygulanan anestezik maddeler ve analjezi i?in kullan?lan baz? ila?lar obstr?ktif uyku apne sendromunda bahsi ge?en bu hipoksi ve kardiyovask?ler problemlerin artmas?na neden olabilir. Bu derleme sa?l?k kurulu?lar?na ula??m?n ve dolay?s?yla cerrahi uygulamalar?n say?s?n?n artt??? g?n?m?zde bu hasta grubunda anestezi ?ncesi ve sonras? al?nmas? gereken ?nlemler ve yakla??m konusunda klinisyenlere yard?mc? olabilece?i d???ncesi ile haz?rlanm??t?r.
Anahtar kelimeler: Uyku apne sendromlar?, anestezi, perioperatif bak?m
SUMMARY
Perioperative evaluation for the patients with obstructive sleep apnea syndrome
Obstructive sleep apnea syndrome, that has been more frequently diagnosed lately and whose importance has been gradually understood better, is a widespread health problem. This syndrome has been accompanied by obesity frequently. In the obstructive sleep apnea syndrome, it has been known that hypoxia and sometimes hypercarbia additionally has been observed, nevertheless cardiovascular problems have been observed more frequently in the aforementioned patient group in comparison with other individuals. Anesthetic substituents applied during the invasive operations and some medicine used for analgesia may cause the increase of the aforesaid hypoxia and cardiovascular problems in the obstructive sleep apnea syndrome. Nowadays, with the improvements in accessing to health agencies and consequently with the increase in the number of surgical applications, this review has been prepared with the thought of helping to clinicians about the approach and the pre-anesthetic and post-anesthetic precautions required to be taken within the mentioned patient group.
Key words: Sleep apnea syndromes, anesthesia, perioperative care
Geli? Tarihi/Received: 30.09.2014 • Kabul Edili? Tarihi/Accepted: 07.10.2014
Introduction and General Information
Obstructive sleep apnea syndrome (OSAS) is characterized with the existence of recurrent apnea and hypopnea during sleeping along the upper respiratory tract (1). These apnea and hypopnea episodes should last at least 10 seconds. Community-based epidemiological studies have shown that morbidity and mortality have increased in patients with OSAS (2,3). In addition, it is known that for about 80% of the patients OSAS have not been diagnosed yet and so have remained as not receiving a treatment yet (4). These apneas and hypopneas occurring during sleeping may cause cardiovascular complications resulting in sudden and unexpected deaths (5).
It is well-known fact that there is a relationship between obesity and OSAS (6). Lately, it has been accepted by all of the health authorities that obesity has been spreading. Therefore, it is inferred that the sensitivity among health staff on the OSAS issue, which may accompany to growing obesity, should increase. It is reported that OSAS frequency in men is about 4% and %2 in women (7). Also in another study, the patients, who would be treated with upper airway surgery, were isolated and it was detected that the OSAS rate was 22% in the other surgical patient population and that of the 70% of the mentioned patients received no diagnosis and no treatment - in consequence (8). The necessity of a special perioperative approach for such a common patient group that not even diagnosticated or received any treatment is obvious.
It appears that undesired incidents increase among the patients with OSAS when the perioperative preparations haven't been done properly in the cases like in anesthesia applications with loss of conscious (9). Liao et al. have proved postoperative complications were higher in the patients with OSAS considering the other group (44% and 28%, p< 0.01) (10). In this retrospective cohort study, he pointed out to the increased respiratory complication, prolonged monitorization requirement and enhanced intensive care need. Yet, in the similar studies, the patients treated with orthopedic surgery with OSAS and without OSAS were compared; and some complications like reintubation, acute hypercapnia, arrhythmia, myocardial ischemia, infarct and delirium were observed more frequent among the patient group with OSAS (8,11).
The carbon dioxide level increased during apneas and hypopneas due to upper airway obstruction in the patients with OSAS stimulates the respiratory center and, because of this stimulus, the apnea and hypopnea ends with the stimulation of the respiratory reflex. However; propofol, pentothal, halothane, benzodiazepine and opioid agents frequently used during the anesthesia suppress the respiratory response resisting the increased carbon dioxide level (12). Under the light of these data, the reason why a better perioperative preparation process is required for the patients with OSAS can be obviously seen.
The standard test for OSAS diagnosis is polysomnography. Sleep electroencephalography (EEG), electrocardiography (EKG), leg and chin electromyography (EMG), pulse oximeter and oxygenation monitoring, nasal and oral airflow, position sensor, abdomen and thorax effort sensors and the record of more than one parameters are all done in the same time (13). The apnea is defined as the total or approximate airflow discontinuance for at least 10 seconds. The widely used definition for hypopnea is given as the 4% reduction in partial oxygen pressure (SPO2) on pulse oximeter together with a reduction of %30 in airflow (14). The frequency of apneas and hypopneas per hour is defined as apnea hypopnea index (AHI) and according to the guidelines published by American Academy of Sleep Medicine (AASM), it is accepted as sleep apnea syndrome when the AHI is over 5. The patients whose values are between 5 and 15 are considered as mild, 15- 30 are as moderate and over 30 are as critically ill (14). In the United States of America, the treatment is advised when the AHI alone is over 15 or in the presence of accompanying comorbidity such as cerebrovascular illness, ischemic heart disease, hypertension and excessive daytime sleepiness for the patients with values of AHI> 5 (15).
As well as the rest of the world, polysomnography is a relatively high-cost test whose appointments are future-dated. Due to these limitations, the estimations obtained through portable polysomnograps at home for perioperative evaluation by AASM are announced to be able to be the alternative for the standard PSG practice. In the cases where even the portable screen tests cannot be held, polling questionnaires prepared upon patient amnesia and physical examination findings can be utilized.
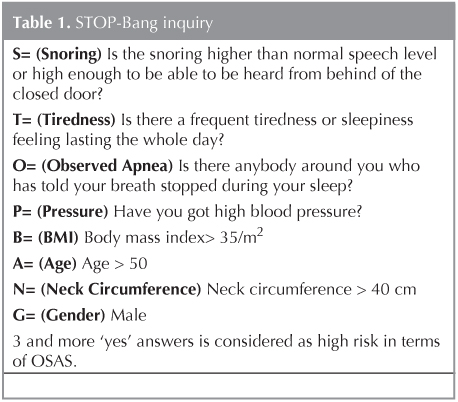
Berlin questionnaire or STOP-Bang polling method can be applied in OSAS inquiry (16,17). STOP-Bang inquiry is given Table 1. It has been reported that there is a correlation between the positivity of this inquiry and especially the respiratory postoperative complications. When the score is 3 or over in this inquiry, it is accepted highly risky in terms of OSAS. In recent years, perioperative sleep apnea syndrome prediction score (P-SAP) has also been used. However, in spite of the high sensitivity of this scoring, its specifity was observed low (18).
Surgical Strategies
The patients who will receive surgical treatment must be evaluated in sense of OSAS. Early diagnosed patients must directly be prepared according to this. But, non-diagnosed patients should be evaluated according to Berlin Questionnaire or inquiries such as STOP-Bang and the preparations should be made as if there are high risks in terms of OSAS. Preparing the patients will be determined under the separate titles as preoperative, intraoperative and post operative.
Preoperative Preparation
All the patients should be evaluated in terms of OSAS using an OSAS inquiry questionnaire. In the study held 1/4 of the patients questioned were detected to have high risk of OSAS. In this patient group ear, nose and throat examination is important. The existence of examination findings such as micrognathia, retrognathia, adenotonsillar hypertrophy and macroglossia both helps in terms of possible OSAS diagnosis and facilitates having an opinion about possible difficult intubation. It is known that tracheal intubation is harder in patients with OSAS (19). Other basic examination findings in terms of possible OSAS have been presented during STOP-Bang inquiry. It should be kept in mind that comorbidity incidents like ischemic heart disease, obesity, hypertension may be observed in the patients, who were diagnosed as OSAS or found risky in the inquiry; they should be evaluated accordingly, and when needed, demanding a consultation from the related optimal surgeon preparations should be done.
Various studies have proved that the possibility of pulmonary arterial hypertension (PAH) increases in the patients with OSAS. In these studies, PAH rate was detected between 15% and 20% in the patients without a known significant pulmonary that may cause PAH and any cardiac disease (20,21). Hypoxia, hypercapnia, acidosis and fever that may occur during perioperative period may trigger this pulmonary hypertension. In the routine application, forward examination is not suggested for any patients having OSAS in terms of PAH (22). However, for the appropriate patients at least an echocardiography may be intended.
As a result, OSAS risk must be considered by holding a polysomnographic examination if possible; if not, utilizing one of the inquiry questionnaires during the preoperative period; afterwards required preparations must be done for the possible comorbidities that may accompany.
Intraoperative Follow-up
As far as possible, local or regional anesthesia instead of general anesthesia should be preferred for the patients with OSAS. If tracheal intubation is required for the patient, necessary equipment in case of difficult intubation must be kept available. Anxiolytic medicines, which are used before the anesthesia induction to patient, should be given slowly and with the dozes as lower as possible and complete sedation must be avoided.
It has been shown that, making the patient breath with 10 cmH2O pressure about 3 or 5 minutes through CPAP device and positioning the head 25 degrees high will be beneficial before starting the general anesthesia (23). It is supposed that the mentioned preoperative CPAP practice decreases the edema in upper respiratory tract and reduces the inflammation. Besides, it also provides an advantage like starting the operation with high oxygen level of the patient in the event of difficult intubation.
In this patient group, intubation with auxiliary intubation techniques such as fiber optic intubation may be required to be applied to the patient because of difficult intubation. Moreover, intubation without complete sedation may be required. In such cases, it should be kept in mind that the local anesthetics that will be used in upper airway will damage the oropharyngeal and upper respiratory tract suppressive reflexes, and therefore, that the risk of upper respiratory tract obstruction will increase.
The correct measure of tension arterial may be appropriate for opening an artery line, during the operation for both metabolic and close monitoring of respiratory situation especially among the patients suffering morbid obesity. Oxygenation, hypercarbia, PH follow-up and constant tension arterial follow-up can be held owing to the blood gases obtained through this artery line.
Choosing the agents except for opioid must be paid attention both in intraoperative and postoperative periods. If opioid usage is needed, very short-acting medicines such as remifentanil should be preferred.
Postoperative Follow-up
Close monitoring of the patient is necessary until the patient completely awakens after intubation and the upper respiratory tract suppressive reflexes such as coughing and the muscle strength of the patient recovers. It is adviced that, this patient group should be observed in postoperative care unit or in intensive care unit positioning the head to 30 degrees height during the postoperative period. It is known that apnea and hypopneas of the OSAS patients may increase in supine position (24). Still, CPAP can be applied during postoperative period in order to prevent the apnea and hypopnea as well as to heal the oxygenation.
It is proved that opioid use may cause hypoxia (25). For this reason, non-steroid anti-inflammatory drugs (NSAID) and non-opioid drugs like acetaminophen should be preferred for analgesia in the mentioned patient group. For the patients opioid usage is required despite NSAID and acetaminophen, the needed opioid dosage will be lower. Also, selective alpha-2 adrenergic blockers such as ketamine, dexmedetomidine may reduce the necessity of opioid.
Oxygen desaturation may be observed among patients with OSAS within 24-48 hours in postoperative period (26). Therefore, the patient should be kept in postoperative care unit or intensive care unit for the close SPO2 monitoring, pain control, presence of apnea or hypopnea and cardiovascular monitorization during this period. The patient can be transferred to normal hospital room when he/she reaches to pre-surgery oxygen saturation, is stabilized in terms of cardiovascular conditions and when the pain control is ensured.
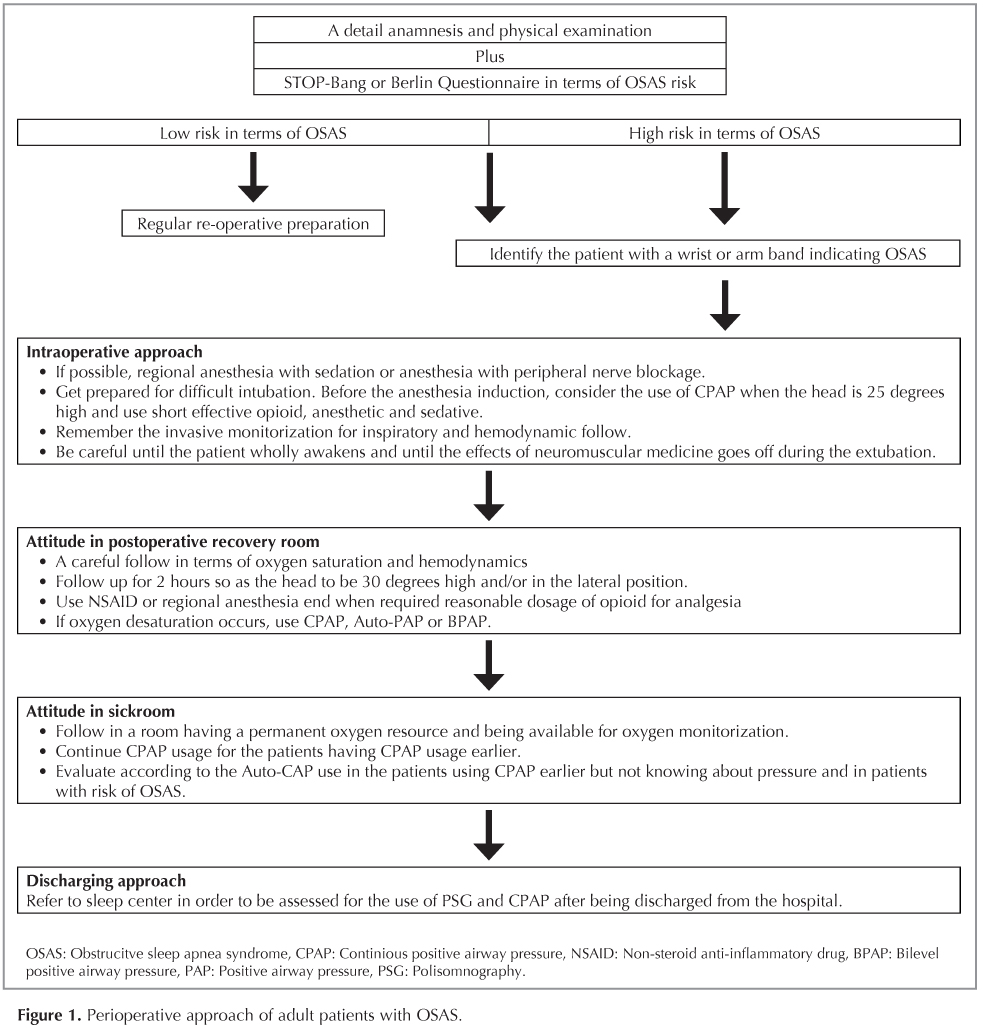
The algorithm published by Adesanya et al. and prepared in the review summarizes smoothly the approach presented thus far about the patients with OSAS (Figure 1) (27).
OSAS in Ambulatory Surgery
In same surgical cases the patient can be discharged the same day. In such patient group, aforementioned preoperative and intraoperative suggestions are to be applied exactly, general anesthesia and opioid use should be avoided as far as possible. According to the guidelines released by ASA, it is suggested that the latter patients should be observed additionally 3 hours more considering the others in hospital; and be kept and monitored additionally 7 hours more if apnea or hypopnea develops during this postoperative follow-up (28). However, these suggestions are based upon expertize rather than proved studies.
Place of CPAP Device
CPAP device has been still the most effective treatment method in OSAS treatment (29). The studies by Gupta et al. have proved that CPAP use reduces the postoperative complications and the hospitalization duration in the preoperative period for the patients with OSAS (11). In this patient group, it is supposed that 100% oxygen usage for 3 or 5 minutes may be beneficial just before the anesthesia induction.
Although the data on CPAP use is limited in postoperative period, the use is accepted as beneficial considering the present conditions. Yet, there is not adequate data about the use of intraoral apparatus, which can be used alternatively to CPAP treatment for OSAS treatment during postoperative period. In the pre-surgery period, the data on which pressure adjustments and in what amount will the CPAP use be done in postoperative period is limited concerning the patients without OSAS diagnosis and not using CPAP. It is considered that CPAP treatment should be maintained according to the follow-up of the parameters such as pulse oximeter and blood gas during the respiratory monitorization and observing the apneas and hypopneas in the clinical follow-up of this group of patients.
Despite the fact that the working principle of the Auto-CPAP devices is similar to CPAP device, there are some differences in this device. In Auto-CPAP device, lower limit and upper limit pressure range is determined and during each patients' inspirium if there is an apnea or hypopnea pressure is given enough to surpass the obstruction; if there is no obstruction, it releases the pressure from the lower level adjusted earlier. So, the mentioned Auto-CAP devices are considered as a good alternative of treatment since the required pressure values the needed for the patient have not been predetermined in the group with high risk of OSAS and without any applications of CPAP. Also, the BPAP devices presenting high pressure in inspiration and low pressure in expiration should be preferred to CPAP instead of this fixed pressure devices for the patient group with a known cardiac insufficiency and with chronic obstructive pulmonary disease (30).
It should be remembered that opioid use for analgesia and all of the aforementioned devices may trigger the central based apneas in especially postoperative period. There is no obstruction in central apnea and the respiratory effort is not been triggered by the central nerve system. These devices do not inhibit the central apneas because of the working principle. Rarely encountered epidemic encephalitis such as central sleep apnea syndrome and isolated obesity hypoventilation syndrome related with respiration should be appraised separately.
Result
OSAS is a commonly encountered sickness increasing the perioperative complication risk among people. Additionally, a significant proportion of the patients with OSAS have not been diagnosed yet. For the patients being suspected from OSAS in the physical examination and anamnesis, PSG should be done first, if not possible, inquiries defining the OSAS risk should be held. After the inquiry, is the OSAS risk seems high, these expected surgical individuals should be treated as if they were OSAS diagnosed patients. If particularly opioid and neuromuscular blocking agent is to be used in this patient group, short-acted drugs should be preferred as far as possible. A reliable anesthesia plan in terms of anesthesia must be designed for these individuals. CPAP application is considered appropriate in the preoperative and postoperative periods; however, prospective studies are needed about the application method and duration.
CONFLICT of INTEREST
None declared.
REFERENCES
- Caples SM, Gami AS, Somers VK. Obstructive sleep apnea. Ann Intern Med 2005;1423:187-97.
- Bahammam A, Delaive K, Ronald J, Manfreda J, Roos L, Kryger MH. Health care utilization in males with obstructive sleep apnea syndrome two years after diagnosis and treatment. Sleep 1999;22:740-7.
- He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and apnea index in obstructive sleep apnea. Experience in 385 male patients. Chest 1988;94:9-14.
- Kapur V, Strohl KP, Redline S, Iber C, O'Connor G, Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath 2002;62:49-54.
- Liao P, Yegneswaran B, Vairavanathan S, Zilberman P, Chung F. Postoperative complications in patients with obstructive sleep apnea: a retrospective matched cohort study. Can J Anaesth 2009;5611:819-28.
- Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest 2010;1373:711-9.
- Krieger J, Turlot JC, Mangin P, Kurtz D. Breathing during sleep in normal, young, and elderly subjects: hypopneas, apnoeas and correlated factors. Sleep 1983;6:108-20.
- Finkel KJ, Searleman AC, Tymkew H, Tanaka CY, Saager L, Safer-Zadeh E, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med 2009;107:753-8.
- McNicholas WT, Ryan S. Obstructive sleep apnoea syndrome: translating science to clinical practice. Respirology 2006;112:136-44.
- Liao P, Yegneswaran B, Vairavanathan S, Zilberman P, Chung F. Postoperative complications in patients with obstructive sleep apnea: a retrospective matched cohort study. Can J Anaesth 2009;56:819-28.
- Gupta RM, Parvizi J, Hanssen AD, Gay PC. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: a case-control study. Mayo Clin Proc 2001;769:897-905.
- Waters KA, McBrien F, Stewart P, Hinder M, Wharton S. Effects of OSA, inhalational anesthesia, and fentanyl on the airway and ventilation of children. J Appl Physiol 2002;925: 1987-94.
- Kushida CA, Littner MR, Morgenthaler T, Alessi CA, Bailey D, Coleman J Jr, et al. Practice parameters for the indications for polysomnography and related procedures: an update for 2005. Sleep 2005;284:499-521.
- Iber C, Ancoli-Israel S, Chesson A, Quan S. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications for the American Academy of Sleep Medicine. 1st ed. Westchester: IL: American Academy of Sleep Medicine; 2007.
- Centers for Medicare and Medicaid Services. Medicare National Coverage Determinations Manual. Chapter 1, part 4 (Section 200-310.1) Covarage Determinations. Accessed Date: 29 September 2014. Available from: www.cms.gov/Regulations-and- Guidance/Guidance/Manual/downloads/ncd103c1_Part4.pdf.
- Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med 1999;1317:485-91.
- Chung F, Yegneswaran B, Liao P, Chung SA, Vairavanathan S, Islam S, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;1085:812-21.
- Ramachandran SK, Kheterpal S, Consens F, Shanks A, Doherty TM, Morris M, et al. Derivation and validation of a simple perioperative sleep apnea prediction score. Anesth Analg 2010;1104:1007-15.
- Siyam MA, Benhamou D. Difficult endotracheal intubation in patients with sleep apnea syndrome. Anesth Analg 2002;954:1098-102.
- Sajkov D, Cowie RJ, Thornton AT, Espinoza HA, McEvoy RD. Pulmonary hypertension and hypoxemia in obstructive sleep apnea syndrome. Am J Respir Crit Care Med 1994;1492:416-22.
- Barst RJ, McGoon M, Torbicki A, Sitbon O, Krowka MJ, Olschewsky H, et al. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004;4312:40-7.
- Atwood CW Jr, McCrory D, Garcia JG, Abman SH, Ahearn GS. American College of Chest Physicians Pulmonary artery hypertension and sleep-disordered breathing: ACCP evidence-based linical practice guidelines. Chest 2004;1261:72-7.
- Delay JM, Sebbane M, Jung B, Nocca D, Verzilli D, Pouzeratte Y, et al. The effectiveness of noninvasive positive pressure ventilation to enhance preoxygenation in morbidly obese patients: a randomized controlled study. Anesth Analg 2008;1075:1707-13.
- Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep 1984;72:110-4.
- Brown KA, Laferri?re A, Lakheeram I, Moss IR. Recurrent hypoxemia in children is associated with increased analgesic sensitivity to opiates. Anesthesiology 2006;1054:665-9.
- Gali B, Whalen FX, Schroeder DR, Gay PC, Plevak DJ. Identification of patients at risk for postoperative respiratory complications using a preoperative obstructive sleep apnea screening tool and postanesthesia care assessment. Anesthesiology 2009;1104:869-77.
- Adesanya AO, Lee W, Greilich NB, Joshi GP. Perioperative management of obstructive sleep apnea. Chest 2010;138:1489-98.
- Gross JB, Bachenberg KL, Benumof JL, Caplan RA, Connis RT, Cot? CJ, et al. American Society of Anesthesiologists Task Force on Perioperative Management Practice guidelines for the perioperative management of patients with obstructive sleep apnea: a report by the American Society of Anesthesiologists Task Force on Perioperative Management of patients with obstructive sleep apnea. Anesthesiology 2006;1045:1081-93.
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;3659464:1046-53.
- Khayat RN, Abraham WT, Patt B, Pu M, Jarjoura D. In-hospital treatment of obstructive sleep apnea during decompensation of heart failure. Chest 2009;1364:991-7.
Yaz??ma Adresi (Address for Correspondence)
Dr. Mustafa ??RT?K
Adana Numune E?itim ve Ara?t?rma Hastanesi,
G???s Hastal?klar? ve T?berk?loz B?l?m?,
ADANA - TURKEY
e-mail: mcortuk@yahoo.com