RESEARCH ARTICLE
Doi: 10.5578/tt.8673
Tuberk Toraks 2015;63(1):22-30

T?rnak yata?? kapillaroskopisinin interstisyel akci?er hastal???ndaki yeri - idiyopatik olgular? kollajen doku hastal??? ile ili?kili interstisyel akci?er hastal?klar?ndan ay?rabilir mi?
Dilek ?AKMAK?I KARADO?AN1, Ay?e BALKARLI2, ?zg?r ?NAL3, G?ksel ALTINI?IK4, Veli ?OBANKARA2
1 Hopa Devlet Hastanesi, G???s Hastal?klar? B?l?m?, Artvin, T?rkiye
1 Department of Chest Diseases, Hopa State Hospital, Artvin, Turkey
2 Pamukkale ?niversitesi T?p Fak?ltesi, Romatoloji Anabilim Dal?, Denizli, T?rkiye
2 Department of Rheumatology, Faculty of Medicine, Pamukkale University, Denizli, Turkey
3 Pamukkale ?niversitesi T?p Fak?ltesi, Halk Sa?l??? Anabilim Dal?, Denizli, T?rkiye
3 Department of Public Health, Faculty of Medicine, Pamukkale University, Denizli, Turkey
4 Pamukkale ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Denizli, T?rkiye
4 Department of Chest Diseases, Faculty of Medicine, Pamukkale University, Denizli, Turkey
?ZET
T?rnak yata?? kapillaroskopisinin interstisyel akci?er hastal???ndaki yeri - idiyopatik olgular? kollajen doku hastal??? ile ili?kili interstisyel akci?er hastal?klar?ndan ay?rabilir mi?
Giri?: T?rnak yata?? kapillaroskopisi (TYK) ?o?unlukla kollajen doku hastal?klar?n?n erken tan?s?nda kullan?lan noninvaziv bir tan? y?ntemidir. Bu ?al??mada TYK bulgular?n?n idiyopatik interstisyel akci?er hastal?klar?n? (idiyopatik-?AH) kollajen doku hastal??? ile ili?kili olan interstisyel akci?er hastal?klar?ndan (KDH-?AH) ayr?m?nda ve ola?an interstisyel pn?moni paternini de nonspesifik interstisyel pn?moni paterninden ay?rmada yarar? olup olmayaca??n? de?erlendirmeyi ama?lad?k.
Materyal ve Metod: Hastalar ?? ana grupta incelendi; KDH-?AH grubunda 15 hasta, idiyopatik ?AH olan grupta 18 ve kontrol grubunda da 17 hasta mevcuttu. KDH-?AH grubu da iki subgruba ayr?ld?; Sj?gren sendromuna (SjS) ba?l?-?AH olan 8 ve romatoid artrite (RA) ba?l? ?AH olan 7 hasta mevcuttu. Kontrol grubunu olu?turanlar da akci?er tutulumu olmayan 10 SjS ve 7 RA hastalar? idi. Hastalar?n hi?biri inceleme s?ras?nda atakta d?neminde de?ildi ve hi?bir hastan?n Reynaud fenomeni yoktu.
Bulgular: Ortalama kapiller yo?unluk yaln?zca KDH-?AH grubunda kontrol grubuna g?re d???kt? (p= 0.006). Subgroup analizinde, RA-?AH, ?PF ve SJS-?AH olan subgruplar?n kapiller anormalliklerinin daha ciddi d?zeyde oldu?u saptand?. Ortalama kapiller yo?unlu?un O?P paterni olanlarda, NS?P paterni olanlar ve kontrol grubunda olanlara g?re daha d???k oldu?u saptand?; p de?eri s?ras?yla 0.008 ve < 0.001 idi.
Sonu?: Bu ?al??ma NS?P ve O?P paterni olan hastalar?n t?rnak yata?? kapillaroskopik bulgular?n? tan?mlayan ve k?yaslayan literat?rdeki ilk ?al??mad?r. TYK bulgular?n?n bu iki radyolojik paternin ayr?m?nda yard?mc? olabilece?ini g?stermektedir. Ancak, idiyopatik interstisyel akci?er hastal???n?n ay?r?c? tan?s?ndaki yerinin de?erlendirilmesi i?in daha geni? hasta gruplar?n? inceleyen daha fazla say?da ?al??maya ihtiya? vard?r.
Anahtar kelimeler: ?nterstisyel akci?er hastal?klar?, t?rnak yata?? kapillaroskopisi
SUMMARY
The role of nailfold capillaroscopy in interstitial lung diseases - can it differentiate idiopathic cases from collagen tissue disease associated interstitial lung diseases?
Introduction: Nailfold capillaroscopy (NFC) is a non-invasive diagnostic test that is mostly used for early diagnosis of collagen tissue diseases (CTDs). We aimed to evaluate whether NFC findings could be a clue for discriminating idiopathic interstitial lung diseases (ILD) from CTD associated ILDs (CTD-ILD). Additionally it was aimed to determine whether NFC could be helpful in discriminating usual interstitial pneumonia (UIP) pattern from non-specific interstitial pneumonia (NSIP) pattern.
Materials and Methods: We grouped patients into three main groups: 15 CTD-ILD, 18 idiopathic ILD, and 17 patients in the control group. The CTD-ILD group was split into two subgroups: 8 patients with Sj?gren's syndrome (SJS)-associated ILD and 7 with rheumatoid arthritis (RA)-associated ILD. The idiopathic-ILD group consisted of 10 idiopathic NSIP and 8 IPF patients. The control group consisted of 10 SJS and 7 RA patients without lung disease. None of the patients were on acute exacerbation at the time of examination, and none had Reynaud's phenomenon.
Results: Mean capillary density was significantly reduced only in the CTD-ILD group as compared to the control group (p= 0.006). In subgroup analysis, it was determined that RA-ILD, IPF, and SJS-ILD subgroups had more severe capillaroscopic abnormalities. Mean capillary density in patients with the UIP pattern was reduced compared to patients with the NSIP pattern and those in the control group; p values were 0.008 and < 0.001, respectively.
Conclusion: This study is to be the first describing and comparing the nailfold capillaroscopic findings of patients with NSIP and UIP patterns. NFC findings can be helpful in discriminating UIP patterns from NSIP patterns. But to show its role in differentiating idiopathic disease, more studies with more patients are needed.
Key words: Interstitial lung diseases, nailfold capillaroscopy
Geli? Tarihi/Received: 20.08.2014 • Kabul Edili? Tarihi/Accepted: 24.12.2014
INTRODUCTION
Interstitial lung diseases (ILD), also called diffuse parenchymal lung diseases, are a group of more than 200 diseases characterized by fibrosis and inflammation of lung parenchyma and interstitium (1,2).
ILD has been classified into four groups: diseases with a known cause, granulomatous diseases, rare diseases, and idiopathic interstitial pneumonias (1). Between idiopathic interstitial pneumonias, idiopathic pulmonary fibrosis (IPF), and idiopathic nonspecific interstitial pneumonia (NSIP) are the most commonly seen (3).
In IPF and idiopathic NSIP the radiologic patterns are UIP and NSIP, respectively. Radiologically, the UIP pattern is characterized by subpleural honeycombing, traction bronchiectasis, thickened interlobular septae predominantly at the peripheral, subpleural, and bibasilar lung fields. NSIP pattern is characterized with ground-glass opacities, rare consolidation, and lower lobe volume loss. Relative peribronchovascular distribution, a large extent of areas with ground-glass attenuation, and subpleural sparing are more highly seen in patients with NSIP, whereas a wide extent of honeycombing and subpleural distribution are more common characteristics in patients with UIP (4).
Collagen tissue disease associated- interstitial lung diseases (CTD-ILD) have similar clinical, radiological, and pathological findings to idiopathic ILDs; therefore, it is difficult to discriminate these two groups from each other (5,6,7). Also, some CTDs are present with ILD before the rheumatologic findings, meaning they can be misdiagnosed as idiopathic ILD (8). Though autoantibodies are helpful for early diagnosis, more tests are required.
Nailfold capillaroscopy (NFC) is a noninvasive test that shows local microvascular changes. It is frequently used for early diagnosis of systemic sclerosis. The typical scleroderma pattern is characterized by decreased capillary density, neoangiogenesis (new bushy, bizarrely shaped loops), micro-hemorrhages, avascular areas, and the disorganization of capillary architecture (9,10).
Most of the studies showing specific NFC findings have involved patients with systemic sclerosis, polymyositis, and/or Reynaud's phenomenon (RP). There are several studies about NFC findings in patients with RA and primary Sj?gren's syndrome (SJS); the typical scleroderma pattern is less common in this group of patients and is associated with the presence of RP (11,12,13,14,15). But none of these studies show the relation between lung involvement and nailfold changes. When NFC findings in RA patients have been examined, elongated capillaries and a prominent subpapillary plexus have been reported as the most frequent capillaroscopic changes (16). Capillaroscopic abnormalities in SJS range from non-specific findings (crossed capillaries) to more specific findings (confluent hemorrhages and pericapillary hemorrhages) or scleroderma-type findings (13).
There is one study that shows NFC differences in IPF patients and compares these findings between scleroderma-associated lung fibrosis and chronic obstructive pulmonary disease (COPD) patients (9). There is no study about capillaroscopic findings in patients with the NSIP pattern.
We planned this study to find whether NFC findings could be a clue for discriminating the idiopathic ILD from CTD-ILD, and to determine whether NFC could be helpful to discriminate UIP patterns from NSIP patterns.
MATERIALS and METHODS
Patients
A total of 50 patients were included in the study. They were classified into 3 main groups and 6 subgroups: the idiopathic interstitial lung disease group (idiopathic-ILD) consisted of idiopathic pulmonary fibrosis (IPF) and idiopathic non-specific interstitial pneumonia (iNSIP) subgroups; the collagen tissue disease associated-interstitial lung disease (CTD-ILD) group consisted of rheumatoid arthritis associated-interstitial lung disease (RA-ILD) and Sj?gren's syndrome associated-interstitial lung disease (SJS-ILD) subgroups; and the control group consisted of patients with rheumatoid arthritis-control (RA-control) and Sj?gren's syndrome-control (SJS-control) subgroups. Patients in the control group did not have any lung disease. Also according to radiologic lung patterns, patients were classified as UIP pattern or NSIP pattern for comparison with control group.
All patients in each group had been diagnosed at least 1 year previously and were involved with the study at the time of their periodic control, or invited by us to join the study. From patients' follow-up documents, their clinical, laboratory, radiologic, and functional data were recorded. At the time of their clinical visit for the study, additional demographic data, complaints, and the results of current physical examinations were also recorded.
Nailfold capillaroscopy was performed on all patients; none of them were in an acute phase of pulmonary disease or taking vasoactive drugs. Patients suffering from peripheral microangiopathies-such as diabetes, hypertension, or recent trauma-that could potentially modify the capillaroscopic findings were excluded. None of the patients were suffering from Reynaud's phenomenon.
All tests were performed and subsequently analyzed by two independent observers who had no knowledge about the patient's diagnosis. Appropriate informed consent was obtained from each patient and the study was approved by the Institutional Ethics Committee.
Capillaroscopy Technique and Image Analysis
NFC was performed at room temperature (between 20-22?C) with the patient kept inside in a seated position with the hand being examined placed at heart level for at least 15 minutes before the exam. One drop of immersion oil was applied to the nailfold to maximize the translucency of the keratin layer. Capillary tests were performed on 4 fingers of each hand (thumbs were excluded.) For each finger, two images (from right and from left side of median line) were captured. NFC was performed using a computerized video-capillaroscopy system with a fiber-optic probe magnified by x200 (Optiplex 780). Images were subsequently captured, coded, stored, and analyzed later by two independent observers.
For each capillaroscopic image, the following parameters were evaluated: linear capillary density (number of capillaries/mm), presence of megacapillaries, tortuosity, avascular area, neoformation, meandering, capillary disarrangement, and neo-angiogenic aspects (number of bushy and strangely shaped capillaries/mm).
Neoangiogenesis, or neoformation, is a highly tortuous and arborized capillary loop cluster, often surrounded by a dropout of normal capillary loops. ?Enlarged capillary? or ?ectazie? is used to describe the situation when the magnitude of a capillary is wider than 0.05 micrometers. Micro-hemorrhages are defined as the presence of 2 or more bleeding areas in at least 2 fingers. Loops with limbs that originate from multiple small buds are labelled ?bushy.? Capillaries with limbs upon themselves or that cross another several times are defined as ?meandering.? Tortuosity is reached with the presence of 2 or more cross-capillaries in a 1 mm area. Capillaries with striking atypical morphology, not conforming to the previously defined categories, were called ?bizarre.?
The overall capillaroscopic patterns were defined as follows:
Normal: 7-10 capillaries/mm, hairpin-shaped loops arranged in parallel rows, absence of hemorrhages, tortuous loops, crosses, or neoangiogenesis aspect;
Minor abnormalities: 7-10 capillaries/mm, less than 50% tortuous loops, arranged in parallel rows, with no hemorrhages or neoangiogenesis aspect;
Major abnormalities: decreased capillary density, more than 50% tortuous, enlarged, and/or disarranged loops, with hemorrhages; more than 50% neoangiogenesis, ectazie, and/or microhemorrogia.
Statistical Analysis
The mean and SD of all examined fingers were calculated for quantitative capillaroscopic parameters in each patient. To detect differences between the three groups and six subgroups, the Kruskal-Wallis non-parametric test and chi-square test were used when applicable. A p value ≤ 0.05 was considered significant.
RESULTS
Patients
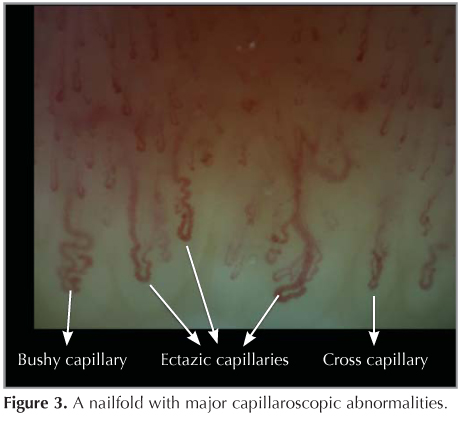
We performed NFC on 18 patients with idiopathic interstitial pneumonias (10 iNSIP, 8 IPF), 15 patients with CTD-associated ILD (8 SJS, 7 RA), and 17 patients with CTD without lung involvement (10 SJS, 7 RA). We analyzed the differences in morphological capillaroscopic parameters between the groups. Table 1 summarizes the clinical and demographic characteristics of patients in each group. Most of the patients were men in the RA-ILD, IPF, and iNSIP groups, while there were women in the control groups and SJS-ILD subgroup.
The mean age of patients was 56.5 ? 12.0 (min. 31, max. 85). Between the main groups' ages there was no significant difference, but in subgroups' analysis, IPF patients were statistically significantly older than SJS-control group patients (p= 0.01).
Most of the patients were never smokers (36, 72.0%). Only 13 (20%) patients were former smokers; 1 (2%)patient was a current smoker. The current smoker was IPF, former smokers were 5 IPF, 3 iNSIP, and 5 RA-ILD. There were 11 patients with finger clubbing; 6 of them were in the iNSIP group, 5 of them were in the IPF group.
Mean medical history was 4.94 ? 5.49 years (min. 1, max. 30 years). For disease duration there was no statistically significant difference between the groups and subgroups. There were 17 patients with the UIP pattern (8 IPF, 7 RA-ILD, 2 SJS-ILD) and 16 patients with the NSIP pattern (10 idiopathic NSIP and 6 SJS-NSIP).
Between pulmonary function test parameters there were significant differences only in diffusion capacity (DLCO) between groups and subgroups. DLCO was lower in the idiopathic-ILD group compared to the control group (p= 0.001). Also, the RA-ILD subgroup's and the IPF subgroup's DLCO was significantly lower compared to all other subgroups (p= 0.002).
Peripheral oxygen saturation was significantly different between groups and subgroups (p< 0.001). The idiopathic-ILD and CTD-ILD groups' levels were significantly lower compared to the control group. The idiopathic-ILD group's SpO2 was lower than the CTD-ILD group as well (p= 0.001). At subgroup analysis, IPF patients' SpO2 levels were lower than those in all other subgroups. RA-ILD and SJS-ILD subgroups' levels were low compared to both control subgroups (p< 0.001). The idiopathic NSIP group's was lower than both control subgroups (p< 0.05).
Capillaroscopic Findings
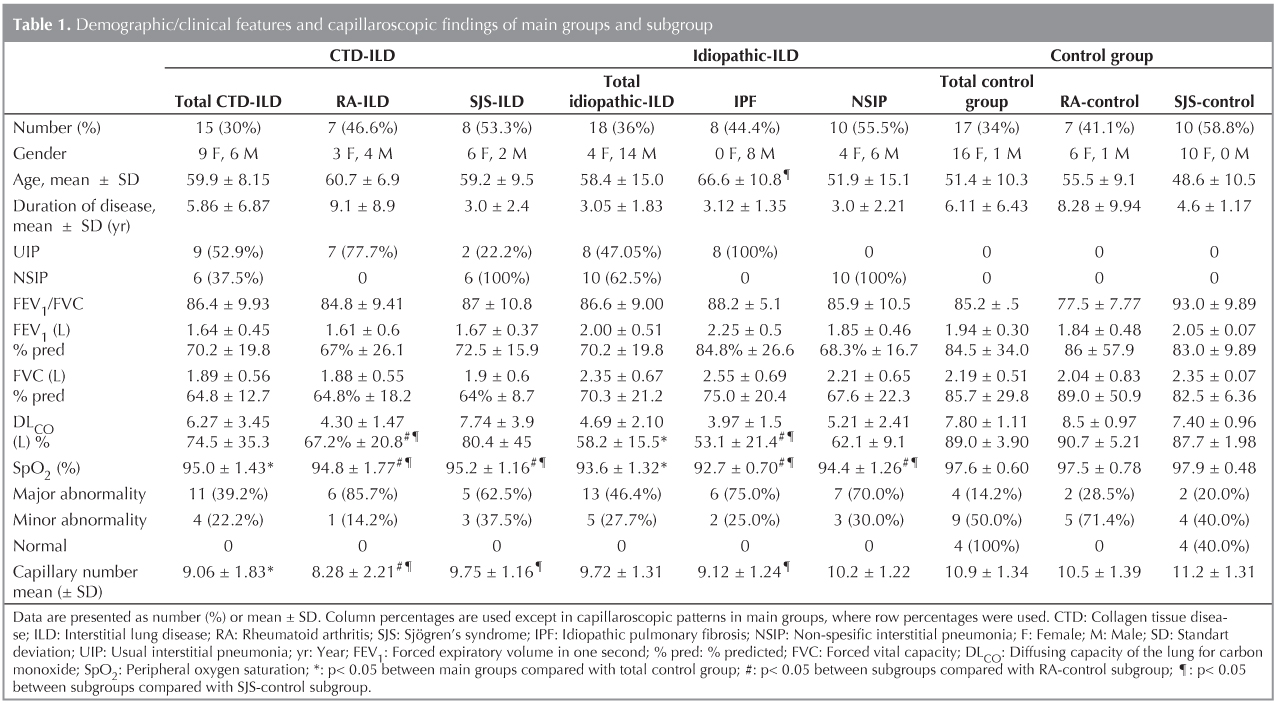
The mean capillary number per millimeter was 9.85 ? 1.61 (range 6-13). Figure 1 and Table 1 show the capillaroscopic findings in the main groups. Most of the patients with major abnormalities were in the idiopathic-ILD and CTD-ILD groups (46.4% and 39.2%, respectively). Half of the minor abnormalities (50.0%) were seen in the control group. All of the patients with normal capillaroscopic findings were in the control group. Because of the small amount of patients (not enough for analysis), we couldn't compare the differences in capillary alterations. The mean capillary number was 9.06 ? 1.83 in the CTD-ILD group, 9.72 ? 1.31 in the idiopathic-ILD group, and 10.9 ? 1.34 in the control group. Between groups, the CTD-ILD group's capillary number was significantly lower than the control group's (p= 0.006).
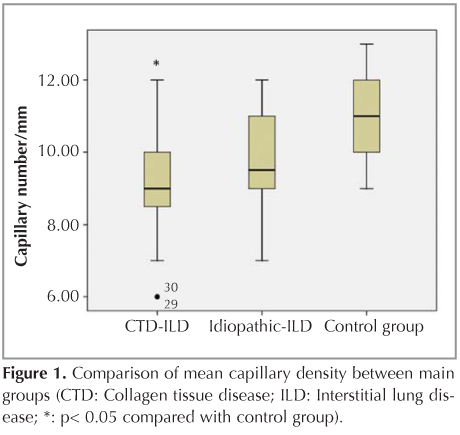
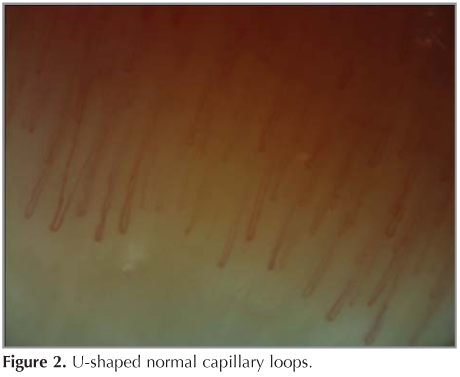
All of the patients with normal capillary findings, as seen in Figure 2, were in the SJS-control subgroup. Most of the patients in the control subgroups showed minor capillaroscopic abnormalities, while most patients in other subgroups showed major abnormalities (Table 1). Figure 3 is an example of a nailfold with major abnormalities. Between subgroups, mean capillary density was 8.28 loops/mm (range 6-12) in RA-ILD patients; 9.75 loops/mm (range 9-12) in Sj?gren-ILD; 9.12 loops/mm (range 7-11) in IPF; 10.2 loops/mm (range 9-12) in idiopathic NSIP; 10.5 loops/mm (range 9-12) in RA-control; and 11.2 loops/mm (range 9-13) in the Sj?gren control group (Table 1).
Mean capillary density was significantly different between subgroups (p= 0.003). The RA-ILD subgroup's capillary number was significantly lower than that of the idiopathic NSIP, RA-control, and SJS-control subgroups; p value was 0.01, 0.005, and < 0.001, respectively. SJS-ILD patients and IPF patients had significantly lower mean capillary numbers than those in the SJS-control subgroup (p values were 0.03 and 0.004, respectively).
None of the patients had megacapillaries, avascular areas, or a specific scleroderma pattern. Table 2 shows the number of patients with certain capillaroscopic findings for each subgroup.
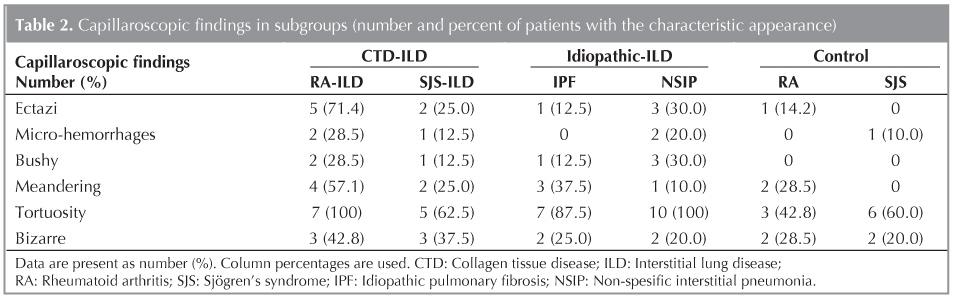
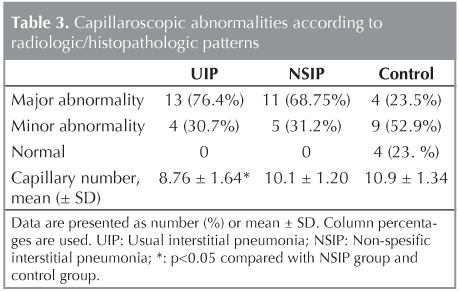
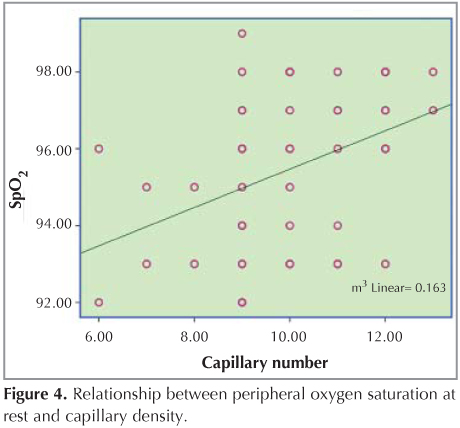
Table 3 shows the capillaroscopic findings according to lung patterns. Capillaries per millimeter were 8.7 ? 1.64, 10.1 ? 1.20, and 10.9 ? 1.34 in patients with UIP pattern, NSIP pattern, and in the control group, respectively. The difference was statistically significant between these groups (p= 0.001). This difference was due to the UIP pattern; patients with a UIP pattern had lower capillary numbers compared to patients with the NSIP pattern and the control group, (p values were 0.008 and < 0.001, respectively. There was a positive correlation between SpO2 measured at rest and capillary density (Figure 4).
Discussion
Capillaroscopy is a non-invasive diagnostic method used for looking at microcirculation. Nailfold video-capillaroscopy is known to be the best predictor of transition from a primary to a secondary Reynaud's phenomenon (17,18). Peripheral microangiopathy can be detected by NFC at early stages of disease. Between CTDs, NFC findings give typical information, especially in scleroderma, dermatomyositis, mixed connective tissue disease, and undifferentiated connective tissue disease-all are called a ?scleroderma-like pattern.? Such changes are not observed in patients with rheumatoid arthritis (RA) or SJS.
ILD can be the first presenting finding in CTDs. Before accepting IIP as an undefined ILD, NFC should be performed on this group of patients (8). Also, it is recognized that there is a need to provide a clinical algorithm for classifying and managing IIP cases. This is particularly applicable when no biopsy is available and high-resolution computed tomography is not diagnostic (3). In our study we intended to discover whether NFC findings could be a clue for discriminating idiopathic ILD from CTD-ILD. Our second aim was to determine whether NFC could be helpful to discriminate UIP pattern from NSIP pattern.
The first result of this study is the finding that capillaroscopic alterations were more severe in the CTD-ILD and idiopathic-ILD groups than the control group. Most patients who had major abnormalities were in these two groups. The ratio of minor abnormalities was similar between groups. All of the patients with normal nailfold capillaroscopic findings were in the control group. Mean capillary density was significantly reduced only in the CTD-ILD group as compared to the control group (p= 0.006). In subgroup analysis it was determined that RA-ILD, IPF, and SJS-ILD subgroups had more severe capillaroscopic abnormalities. The RA-ILD subgroup's capillary density was significantly lower than that of the RA-control, SJS-control, and idiopathic NSIP subgroup. IPF and SJS-ILD subgroups had significantly lower capillary density than the SJS-control subgroup.
Our second finding from this study is that mean capillary density in patients with the UIP pattern was reduced compared to patients with the NSIP pattern and those in the control group (p= 0.001). The third finding is that there was a positive correlation between oxygen saturation and capillary density.
We categorized issues as major abnormalities when at least one of the following findings were determined: ectazic capillary, micro-hemorrhages, neoangiogenic aspects (bushy, bizarre, or meandering loops), decreased capillaries, or tortuosity more than 50%. A recent study showing the capillaroscopic findings in healthy subjects has shown that the most frequent morphologic features are U-shaped loops and tortuous loops, with 7-10 capillaries per millimeter (19). Bushy, crossed, and meandering capillaries, as well as pericapillary hemorrhages, are not frequently observed in healthy subjects (19). So, the findings that we grouped as major abnormalities in our study had not been observed in healthy subjects, however, minor abnormalities, as we described loops with less than 50% tortuosity, can be seen in healthy subjects as well.
Giant or ectazic capillaries are thought to be a local auto-regulatory response to tissue hypoxia-the dilatation may present as the first sign of vessel wall damage. In the current study, 24% of patients had ectazic capillaries; most of them were in the RA-ILD subgroup. Micro-hemorrhages have also been associated with early vascular damage. The microvascular extravasation of the red blood cells is linked to damage to the vessel wall. The number of patients with micro-hemorrhages in this study was 12%. A decreased number of loops (< 30 over 5 mm in the distal row of the nailfold) is highly specific for secondary Reynaud's phenomenon. Loss of capillaries is thought to be relevant in determining critical tissue hypoxia (20). None of the patients in our study had decreased capillary loops.
We found a positive correlation between capillary density and peripheral oxygen saturation. However, it is not possible to say that this is only a consequence of hypoxemia. Although IPF patients' SpO2 levels were lower than that of the RA-ILD group, the RA-ILD group had more severe NFC findings than other groups. A study comparing capillaroscopic findings of IPF patients, systemic sclerosis?related lung fibrosis patients, and COPD patients with chronic hypoxemia found normal NFC findings in COPD patients. Also in this study, researchers found greater severity of capillary lesions in the systemic sclerosis?related pulmonary fibrosis group than IPF groups. They emphasized that this could be due to different weights of vascular involvement in the pathogenesis of tissue damage from the two diseases (9).
NSIP is the most frequent pathological pattern in CTD-ILD, except for RA. Only RA has a higher frequency of UIP. RA-UIP patients have worse survival rates than all other CTD- associated NSIP or UIP patients (21). RA-UIP pattern also has a worse prognosis than IPF-UIP, while all other CTD-UIP patients have better survival rates and prognosis than IPF-UIP (22). In our study we found more severe capillaroscopic lesions in patients with UIP patterns than in those with NSIP patterns and the control group. Most patients with UIP pattern were in the IPF and RA-ILD subgroups. Between these two subgroups, the RA-ILD subgroup had more severe findings. In our study, patients with NSIP-pattern were in the SJS-ILD and the idiopathic NSIP subgroups. Only SJS-ILD patients' capillary density was significantly decreased compared to the SJS-control subgroup. These results could be related to the systemic vascular dysfunction due to different pathophysiological mechanisms of the diseases.
Changes in microcirculation are thought to be a result of an imbalance between angiogenic and angiostatic factors. Also, the prevalence of a high anti-endothelial cell antibody (AECA) has been frequently associated with vascular lesions and activity of autoimmune diseases (11,23).
In a previous study about NFC findings in RA patients, more severe abnormalities were found in patients with RP. The diameter of capillary loops in RA patients without Reynaud's phenomenon had been found to be significantly wider than healthy controls. This was associated with endothelial damage in different mechanisms in these patients (16). There is not currently any study in the literature that shows the NFC findings of RA patients with lung fibrosis. In our study, the RA-ILD subgroup's capillary density was significantly reduced compared to the RA-control group. Because of the small number of patient participants, we couldn't compare their capillaroscopic patterns. But the ratio of patients with major abnormalities was 85.7% in the RA-ILD subgroup and 28.5% in the RA-control subgroup. These findings could be associated with different intensities of endothelial damage due to disease severity.
In SJS patients, major capillaroscopic abnormalities are generally associated with the presence of systemic manifestations and Reynaud's phenomenon (12,24). In the current study, the SJS-ILD subgroup's capillary density was significantly reduced compared to the SJS-control subgroup; the ratio of major abnormalities was 62.5% in the SJS-ILD subgroup while it was only 20.0% in the SJS-control subgroup.
There is only one study that compares the NFC findings in IPF patients as mentioned above, and they hypothesized that capillary changes could be a consequence of systemic endothelial dysfunction, similar to other CTDs but a less pronounced form. The predicted cause was an imbalance between angiogenic and antiangiogenic cytokines, such as vascular endothelial growth factor (VEGF), IL-8, and endothelin-1 (9). There is no study in the literature that evaluates NFC findings of NSIP patients. In our study, the NSIP group showed significantly higher capillary density than the UIP group, but the ratio of major abnormalities was similar (68.7%).
CONCLUSION
This study is to be the first describing and comparing the nailfold capillaroscopic findings of patients with NSIP pattern and UIP pattern. We found that patients with UIP pattern had more severe capillaroscopic abnormalities than both NSIP and control groups. UIP patterns due to rheumatologic diseases had significantly reduced capillary density compared to IPF and control groups. However, a limitation of the current study is the small number of patients in each group; therefore, it is difficult to make strong associations between groups. Additional studies are needed to better define the exact role of nailfold capillaroscopy in the diagnostic procedure of ILD.
CONFLICT of INTEREST
None declared.
REFERENCES
- Harari S, Caminati A. Update on diffuse parenchymal lung disease. Eur Respir Rev 2010;19:97-108.
- Morgenthau AS, Padilla ML. Spectrum of Fibrosing Diffuse Parenchymal Lung Disease. Mount Sinai J Medicine 2009;76:2-23.
- Travis WD, Costabel U, Hansell DM, KingTE Jr, Lynch DA, Nicholson AG, et al.; ATS/ERS Committee on Idiopathic Interstitial Pneumonias. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2013;188:733-48.
- Johkoh T. Non-specific interstitial pneumonia and usual interstitial pneumonia: is differentiation possible by high-resolution computed tomography? Semin Ultrasound CT MR 2014;35(1):24-8. doi: 10.1053/j.sult.2013.10.004. Epub 2013 Oct 17.
- G?mez Carrera L, Bonilla Hernan G. Pulmonary manifestations of collagen diseases. Arch Bronconeumol 2013;49:249-60. doi: 10.1016/j.arbres.2012.11.005. Epub 2013 Feb 4.
- Gutsche M, Rosen GD, Swigris JJ. Connective tissue disease-associated interstitial lung disease: a review. Curr Respir Care Rep 2012;1:224-32.
- Cottin V. Significance of connective tissue diseases features in pulmonary fibrosis. Eur Respir Rev 2013;22:273-80 DOI: 10.1183/09059180.00003013.
- Fischer A, Meehan RT, Feghali-Bostwick CA, West SG, Brown KK. Unique characteristics of systemic sclerosis sine scleroderma-associated interstitial lung disease. Chest 2006;130(4):976-81.
- Corrado A, Carpagnano G, Gaudio A, Foschino-Barbaro MP, Cantatore FP. Nailfold capillaroscopic findings in systemic sclerosis related lung fbrosis and in idiopathic lung fibrosis. Joint Bone Spine 2010;77:570-4.
- Lambova S, M?ller-Ladner U. Capillaroscopic findings in systemic sclerosis-Are they associated with disease duration and presence of digital ulcers? Discov Med 2011;12(66):413-8.
- Riccieri V, Sciarra I, Ceccarelli F, Alessandri C, Croia C, Vasile M, et al. Nailfold capillaroscopy abnormalities are associated with the presence of anti-endothelial cell antibodies in Sjogren's syndrome. Rheumatology (Oxford) 2009;48(6):704-6. Epub 2009 Mar 23.
- Capobianco KG, Xavier RM, Bredemeier M, Restelli VG, Brenol JC. Nailfold capillaroscopic findings in primary Sj?gren's syndrome: clinical and serological correlations. Clin Exp Rheumatol 2005;23(6):789-94.
- Tektonidou M, Kaskani E, Skopouli FN, Moutsopoulos HM. Microvascular abnormalities in Sj?gren's syndrome: nailfold capillaroscopy. Rheumatology (Oxford). 1999;38(9):826-30.
- Kuryliszyn-Moskal A. Cytokines and soluble CD4 and CD8 molecules in rheumatoid arthritis: relationship to systematic vasculitis and microvascular capillaroscopic abnormalities. Clin Rheumatol 1998;17(6):489-95.
- Altomonte L, Zoli A, Galossi A, et al. Microvascular capillaroscopic abnormalities in rheumatoid arthritis patients. Clin Exp Rheumatol 1995;13(1):83-6.
- Lambova SN, M?ller-Ladner U. Capillaroscopic pattern in inflammatory arthritis. Microvasc Res 2012;83(3):318-22. doi: 10.1016/j.mvr.2012.03.002.
- Cutolo M, Smith V. State of art on nailfold capillaroscopy: a reliable diagnostic tool and putative biomarker in rheumatology? Rheumatology (Oxford). 2013 Apr 25.
- Dolijanovic S, Damjanov NS, Stojanovic RM, Vujasinovic Stupar NZ, Stanisavljevic DM. Scleroderma pattern of nailfold capillary changes as predictive value for the development of a connective tissue disease: a follow-up study of 3,029 patients with primary Raynaud's phenomenon. Rheumatol Int 2012;32(10):3039-45.
- Ingegnoli F, Gualtierotti R, Lubatti C, Bertolazzi C, Gutierrez M, Boracchi P, et al. Nailfold capillary patterns in healthy subjects: a real issue in capillaroscopy. Microvasc Res 2013;90:90-5. doi: 10.1016/j.mvr.2013.07.001.
- Cutolo M, Pizzorni C, Secchi ME, Sulli A. Capillaroscopy. Best Pract Res Clin Rheumatol 2008;22(6):1093-108. doi: 10.1016/j.berh.2008.09.001.
- Park JH, Kim DS, Park IN, Jang SJ, Kitaichi M, Nicholson AG, et al. Prognosis of fibrotic interstitial pneumonia: idiopathic versus collagen vascular disease-related subtypes. Am J Respir Crit Care Med 2007;175:705-11.
- Wuyts WA, Agostini C, Antoniou KM, Bouros D, Chambers RC, Cottin V, et al. The pathogenesis of pulmonary fibrosis: a moving target. Eur Respir J 2013;41(5):1207-18. doi: 10.1183/09031936.00073012.
- Riccieri V, Germano V, Alessandri C, Vasile M, Ceccarelli F, Sciarra I, et al. More severe nailfold capillaroscopy findings and anti-endothelial cell antibodies. Are they useful tools for prognostic use in systemic sclerosis? Clin Exp Rheumatol 2008;26:9927.
- Kabasakal Y, Elvins DM, Ring EF, McHugh NJ. Quantitative nailfold capillaroscopy findings in a population with connective tissue disease and in normal healthy controls. Ann Rheum Dis 1996;55(8):507-12.
Yaz??ma Adresi (Address for Correspondence)
Dr. Dilek ?AKMAK?I KARADO?AN
Hopa Devlet Hastanesi,
G???s Hastal?klar? B?l?m?,
ARTV?N - TURKEY
e-mail: cakmakcidilek@yahoo.com