RESEARCH ARTICLE
Doi: 10.5578/tt.8725
Tuberk Toraks 2015;63(1):8-12

Yo?un bak?m d??? kliniklerde geli?en hastanede geli?en pn?moninin mali y?k?
Ebru ?AKIR ED?S1, Osman Nuri HAT?PO?LU1, ?lker YILMAM2, Necdet S?T3
1 Trakya ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Edirne, T?rkiye
1 Department of Chest Diseases, Faculty of Medicine, Trakya University, Edirne, Turkey
2 Samsun G???s Hastal?klar? ve G???s Cerrahisi Hastanesi, G???s Hastal?klar? Klini?i, Samsun, T?rkiye
2 Clinic of Chest Diseases, Samsun Chest Diseases and Chest Surgery Hospital, Samsun, Turkey
3 Trakya ?niversitesi T?p Fak?ltesi, Biyoistatistik Anabilim Dal?, Edirne, T?rkiye
3 Department of Biostatistics, Faculty of Medicine, Trakya University, Edirne, Turkey
?ZET
Yo?un bak?m d??? kliniklerde geli?en hastanede geli?en pn?moninin mali y?k?
Giri?: Literat?rdeki hastanede geli?en pn?moniler (HGP) ile ili?kili maliyet verilerinin hemen hepsi ventilat?rle ili?kili pn?monili hastalarla yap?lan ?al??malardan elde edilmi?tir. Bu ?al??mada ama? hastane kliniklerinde yatan hastalarda pn?moni geli?mesinin mali y?k?n? saptamakt?r.
Materyal ve Metod: Yo?un bak?m d??? kliniklerde pn?moni geli?en ya? ortalamas? 64.53 ? 14.92 olan 97'si erkek toplam 154 HGP'li eri?kin hastaya ait maliyet verileri prospektif olarak kaydedildi. Kar??la?t?rma i?in ayn? tarihler aras?nda ayn? tan?lar ile hastanede yatan, ya?? (ort: 65.66 ? 13.86) ve cinsiyeti (94'? erkek) benzer olup (p> 0.05) hastanede yatt??? s?re i?inde pn?moni geli?memi? olan 148 olgu da kontrol grubuna al?nd?. Her iki gruptaki hastalar?n hastanede yatt?klar? g?n say?lar? ve hastane otomasyon program?ndan (Avicenna) elde edilen maliyet verileri Mann-Whitney U testiyle kar??la?t?r?ld?.
Bulgular: HGP'li hastalarda ortalama yat?? g?n say?s? 32.8 iken kontrol grubunda 9.8 idi (p< 0.0001). Yatak maliyeti HGP'li hasta grubunda ortalama 631$ iken kontrol grubunda 153$ olarak hesapland? (p< 0.0001). Toplam maliyet HGP'li grupta ortalama 6241$ iken kontrol grubunda 1117$ olarak tespit edildi (p< 0.0001).
Sonu?: HGP, yat?? s?resini yakla??k 3.5, yatak maliyetini 4, toplam maliyeti 5.5 kat art?ran mali y?k? y?ksek bir hastal?kt?r.
Anahtar kelimeler: Yo?un bak?m d???, hastanede geli?en pn?moni, maliyet
SUMMARY
Economic burden of nosocomial pneumonia in non-intensive care clinics
Introduction: Almost all data on the cost of nosocomial pneumonia (NP) in the literature is associated with ventilator-associated pneumonia. This study aims to determine the economic burden of nosocomial pneumonia in clinical inpatients.
Materials and Methods: Data on costs of the 154 adult patients (97 male, 57 female; mean age 64.53 ? 14.92) who were hospitalized in non-intensive care clinics and developed NP were recorded prospectively. The control group consisted of 148 patients without pneumonia matched for age (mean age 65.66 ? 13.86), sex (94 male), diagnosis, and hospitalization date. Data obtained from both groups of patients for the number of hospitalization days and the data obtained from the hospital automation program (Avicenna) for costs were compared using the Mann-Whitney U test.
Results: While the mean duration of hospitalization was 32.8 days in patients with NP, it was 9.8 (p< 0.0001) in the control group. The cost of hospital beds was $631 for NP patients and $153 for the controls (p< 0.0001). The total cost was $6241 for NP patients and $1117 for the controls (p< 0.0001).
Conclusion: NP is a high-cost condition that increases the duration of hospitalization 3.5-fold, hospital-bed cost 4-fold, and the total cost 5-fold.
Key words: Non-intensive care, nosocomial pneumonia, cost
Geli? Tarihi/Received: 06.03.2014 • Kabul Edili? Tarihi/Accepted: 11.12.2014
INTRODUCTION
Nosocomial pneumonia (NP) remains a major cause of morbidity and mortality despite all preventive measures and the use of wide spectrum antibiotics (1). In addition, NP prolongs the duration of hospitalization and increases associated costs (2).
Almost all studies on the cost of NP include ventilator-associated pneumonia (VAP) (3,4,5,6,7,8,9,10). The studies on NP in non-intensive care clinics are very limited and only include specific groups of patients (11,12,13). This study aims to determine the economic burden of NP on developed clinics of the hospital.
MATERIALS and METHODS
Patients
The demographic data and surveillance rates of patients with NP hospitalized in the our hospital have been published elsewhere (14). NP diagnoses in those patients were made according to national and international guidelines (1,15). Immunosupressed patients who developed pneumonia and cases with NP in intensive care units were excluded.
This study analyzes the data on costs of the above-mentioned patients. This was designed as a case-control study. To establish a control group, age-, sex- and diagnosis- matched patients who were hospitalized on the same dates were listed using the hospital automation program (Avicenna). The list was reviewed, and those patients who had not developed pneumonia were included in the control group.
Study Protocol
Patients with NP and control patients were followed-up until death or discharge from the hospital. The number of hospitalization days was recorded. Data on costs were obtained from the hospital automation program (Avicenna). Costs for both groups were assessed under the following topics:
Hospital bed costs
Caregiver costs
Costs of antibiotics used for non-pneumonia conditions (surgical prophylaxis, other infections, etc.)
Non-antibiotic treatment costs
Microbiological test costs for isolation of pathogens
Laboratory costs (blood chemistry, complete blood count)
Consultation costs
Total costs
In addition, the costs of antibiotics used to treat pneumonia in NP patients were calculated.
The costs in Turkish lira was converted to US dollars based on the Central Bank of the Turkish Republic's US dollar exchange rates on the day of discharge from the hospital (16).
Statistical Methods
The numeric results were expressed as mean ? sd, and categorical results were expressed as a number (percentage). Normality distribution of the variables was tested using one sample Kolmogorov Smirnov test. Differences between groups were assessed using the Mann-Whitney U test. The chi-square test was used to compare the differences of categorical variables between the groups. A p value < 0.05 was considered as statistically significant. Statistical 7.0 (Stat Soft Inc. Tulsa, OK, USA) statistical software was used for statistical analyses.
RESULTS
Patient Characteristics
Of the 154 NP patients, 57 (37%) were female, and 97 (63%) were male. The mean age was 64.53 ? 14.92. In the control group comprising 148 cases, 54 (36.5%) were female (36.5%) and 94 (63.5%) were male and the mean age was 65.66 ? 13.86. The two groups were similar in terms of gender (p= 0.92) and mean age (p= 0.49). Of the patients with NP, 71.4% were hospitalized in internal medicine clinics and 28.6% in surgical clinics. The mean number of hospitalization days was 32.85 ? 27.33 in NP patients and 9.85 ? 7.08 in control cases (p< 0.0001) (Table 1).
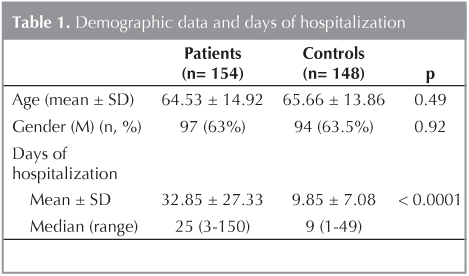
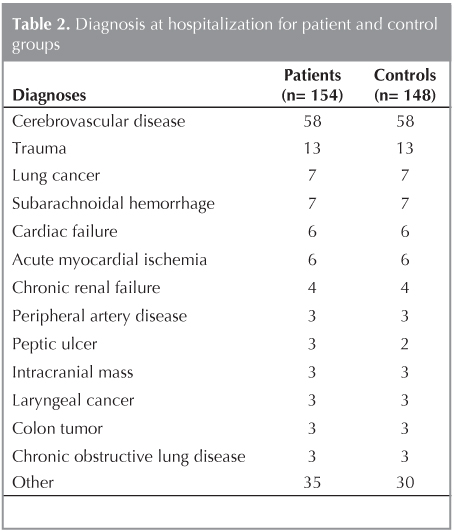
Table 2 shows the diagnoses at hospitalization for NP patients and controls. The control group comprised 148 patients, six fewer than the NP patients, because six NP patients had no control case with an identical diagnosis. They were myasthenia gravis, Guillain-Barre syndrome, peptic ulcer, nasopharyngeal carcinoma, tongue base carcinoma, and suprarenal cancer.
Cost Analyses
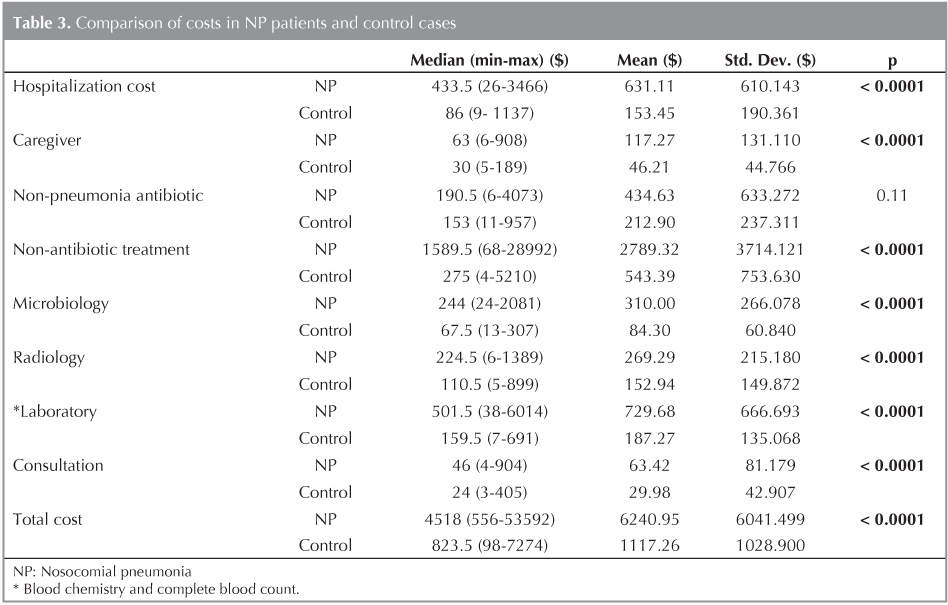
The costs for the NP group were significantly higher than for the control group for all parameters except antibiotics used for non-pneumonia conditions (p= 0.11). The total cost of hospital beds was $631.11 ? 610.14 for the NP group and $153.45 ? 190.36 for the controls. The overall cost was $6240 ? 6041.49 in the NP group and $1117.26 ? 1028.9 for controls (Table 3). The mean cost of antibiotics for pneumonia was $1062.83 ? 1241.47.
DISCUSSION
The nosocomial pneumonia rate is second among nosocomial infections and first among intensive-care unit infections (17). Almost all studies on NP costs include intensive care unit patients with NP. The studies on NP in non-intensive care clinics are very limited.
In a study analyzing the economic burden of NP on the insurance system, the cost of one episode was calculated at $5800 (18). However, that study, including 33 patients with NP and 11 control cases, is not comparable to this study, which has a significantly higher number of cases. Moreover, the data in that study were obtained exclusively from the health insurance database.
Another study investigating the costs of NP patients in medical clinics calculated the cost-effectiveness of invasive procedures for isolation of pathogens and had a different design than this study (13).
A study assessing the outcomes and costs of patients who underwent intraabdominal surgery and developed NP suggested that postoperative pneumonia increased costs (11). However, the study did not report whether the postoperative pneumonia developed in the intensive care unit or the clinic.
In a study investigating nosocomial infections following head and neck surgery, pneumonia was suggested to increase the duration of hospitalization for 17 days and the cost to $19.000 (12). That study included not only postoperative pneumonia but also surgical wound infections.
This study differs from the others in that it was a large-scale study assessing all patients with NP in 23 departments, including all internal medicine and surgery clinics except intensive care and pediatrics in a university hospital. The mean number of hospitalization days was 32.8 and 9.8, the mean hospital bed cost was $631 and $153, and the mean total cost was $6241 and $1117 in the NP and control groups, respectively.
In a meta-analysis assessing the clinical and economic outcomes of patients with VAP, VAP increased the duration of hospitalization for 6.1 days and the cost for $410.019 (4).
A study from Turkey reported the duration of hospitalization as 8 and 2.5 days and the costs $2832.2 and $868.5 in patients with VAP and control cases, respectively (5). The lower costs compared to other studies from Europe and the US was attributed to the low cost of hospital beds in Turkey.
Hospital bed costs, consultation costs, and costs of invasive procedures are significantly lower in Turkey than in other countries. For example, the price of a hospital bed was $8-10, and the consultation price was $5-6 while we ran our study. Thus, comparison of costs in Turkey with the costs in other countries, even based on US dollars, would be inappropriate. We rather would like to emphasize the increase in cost with NP compared to controls.
The major limitation in our study was that, although NP and control cases were matched for age, gender, diagnosis, and hospitalization dates, the severity of their primary conditions were not considered. This may be attributed to the retrospective design of the study and the scattered distribution of control patients in various clinics with various diagnoses. Assessment of scoring systems for severity of disease is much easier in studies including VAP patients because they are routine and critical assessments in such patients.
In conclusion, NP is a high-cost disease that increases the duration of hospitalization 3.5-fold, hospital-bed cost 4-fold, and total cost 5.5-fold. All of the increasing cost not only explain to NP but it is important part of the economic burden. It is essential to take measures for the prevention of NP considering its high cost.
CONFLICT of INTEREST
None declared.
REFERENCES
- American Thoracic Society Documents. Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated and Healthcare-associated Pneumonia. Am J Respir Crit Care Med 2005;171:388-416.
- Craven DE, Steger KA. Epidemiology of nosocomial pneumonia: new perspectives on an old disease. Chest 1995;108:1-16.
- Dietrich ES, Demmler M, Schulgen G, Fekec K, Mast O, Pelz K, et al. Nosocomial pneumonia: A cost of illness analysis. Infection 2002;30:61-7.
- Safdar N, Dezfulian C, Collard HR, Saint S. Clinical and economic consequences of ventilator- associated pneumonia: a systematic review. Crit Care Med 2005;33:2184-93.
- Erbay RH, Yalcin AN, Zincir M, Serin S, Atalay H. Costs and risk factors for ventilator-associated pneumonia in a Turk?sh university hospital's intensive care unit: a case-control study. BMC Pulm Med 2004;4:3.
- Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, et al. Epidemiology and outcomes of ventilator- associated pneumonia in a large US database. Chest 2002;122:2115-21.
- Rosenthal VD, Guzman S, Migone O, Safdar N. The attributable cost and length of hospital stay because of nosocomial pneumonia in intensive care units in 3 hospitals in Argentina: A prospective, matched analysis. Am J Infect Control 2005;33:157-61.
- Eagy KJ, Nicolau DP, Kuti JL. Impact of superinfection on hospital length of stay and costs in patients with ventilator-associated pneumonia. Semin Respir Crit Care Med 2009;30:116-23.
- Kappstein I, Schulgen G, Beyer U, Gieger K, Schumacher M, Daschner FD. Prolongation of hospital stay and extra costs due to ventilator-associated pneumonia in an intensive care unit. Eur J Clin Microbiol Infect Dis 1992;11:504-8.
- Cocanour CS, Ostrosky-Zeichner L, Peninger M, Garbade D, Tidemann T, Domonoske BD, et al. Cost of ventilator- associated pneumonia in a shock trauma intensive care unit. Surg Infect 2005;6:65-7.
- Thompson DA, Makary MA, Dorman T, Pronovost PJ. Clinical and economic outcomes of hospital acquired pneumonia in intra-abdominal surgery patients. Ann Surg 2006;243:547-52.
- Penel N, Lefebvre JL, Cazin JL, Clisant S, Neu JC, Dervaux B et al. Additional direct medical costs associated with nosocomial infections after head and neck cancer surgery: a hospital- perspective analysis. Int J Oral Maxillofac Surg 2008;37:135-9.
- Herer B, Fuhrman C, Gazevic Z, Cabrit R, Chouiad C. Management of nosocomial pneumonia on a medical ward: a comparative study of outcomes and costs of invasive procedures. Clin Microbiol Infect 2009;15:165-72.
- Cakir Edis E, Hatipoglu ON, Yilmam I, Eker A, Tansel O, Sut N. Hospital- acquired pneumonia developed in non-intensive care units. Respiration 2009;78:416-22.
- Turkish Thoracic Society Documents. Guidelines for the Management of Adults with Hospital-acquired Pneumonia 2002. Turkish Thoracic Journal 2002;3:1-13.
- www.tcmb.gov.tr
- Ewig S, Bauer T, Torres A. The pulmonary physician in critical care: Nosocomial pneumonia. Thorax 2002;57:366- 71.
- Boyce JM, Potter- Bynoe G, Dziobek L, Solomon SL. Nosocomial pneumonia in Medicare patients. Hospital costs and reimbursement patterns under the prospective payment system. Arch Intern Med 1991;151:1109-14.
Yaz??ma Adresi (Address for Correspondence)
Dr. ?lker YILMAM
Trakya ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
SAMSUN - TURKEY
e-mail: ebruckr@yahoo.com