LETTER TO THE EDITOR
Doi: 10.5578/tt.8130
Tuberk Toraks 2014;62(4):325-326

Amfizemde elektrokardiyogram: h?zl? yatakba?? tan?sal tarama testi
Nauman KHALID1, Lovely CHHABRA1, David H. SPODICK2
1 Connecticut ?niversitesi T?p Fak?ltesi, ?? Hastal?klar? Anabilim Dal?, Hartford Hastanesi, Hartford, CT
1 Department of Internal Medicine, Faculty of Medicine, University of Connecticut, Hartford Hospital, Hartford, CT
2 Massachusetts ?niversitesi T?p Fak?ltesi, ?? Hastal?klar? Anabilim Dal?, Saint Vincent Hastanesi, Worcester, MA
2 Department of Medicine, Faculty of Medicine, University of Massachusetts, Saint Vincent Hospital, Worcester, MA
We read with great pleasure the work by Akturk et al. published in a recent issue of the Tuberk Toraks (1). In their study, the authors have highlighted the importance of vertical P-vector in diagnosing chronic obstructive pulmonary disease (COPD).
Our group previously published a similar study on a larger patient population which demonstrated that a vertical frontal P-vector can serve as a rapid bedside screening tool for screening emphysema in the general unselected hospitalized population (2). We also showed an inverse correlation of the degree of P-vector verticalization with forced expiratory volume (FEV1). In our other studies, we also showed a correlation of the frontal P-vector verticalization with the radiological severity of emphysema (as estimated by radiographic percentage of emphysematous area and visual scoring of emphysema) (3,4). Interestingly, predominant lower lobe emphysema was found to have the most significant correlation with the frontal P-vector verticalization as compared to the other forms of emphysema. Several explanations have been proposed previously to explain the P-wave verticalization in emphysema, however the most plausible is the downward displacement of the right atrium caused by a progressive flattening of the diaphragm, as the right atrium is attached to the diaphragm by a dense pericardial ligament (5). The schematic illustration is provided in the Figure 1.
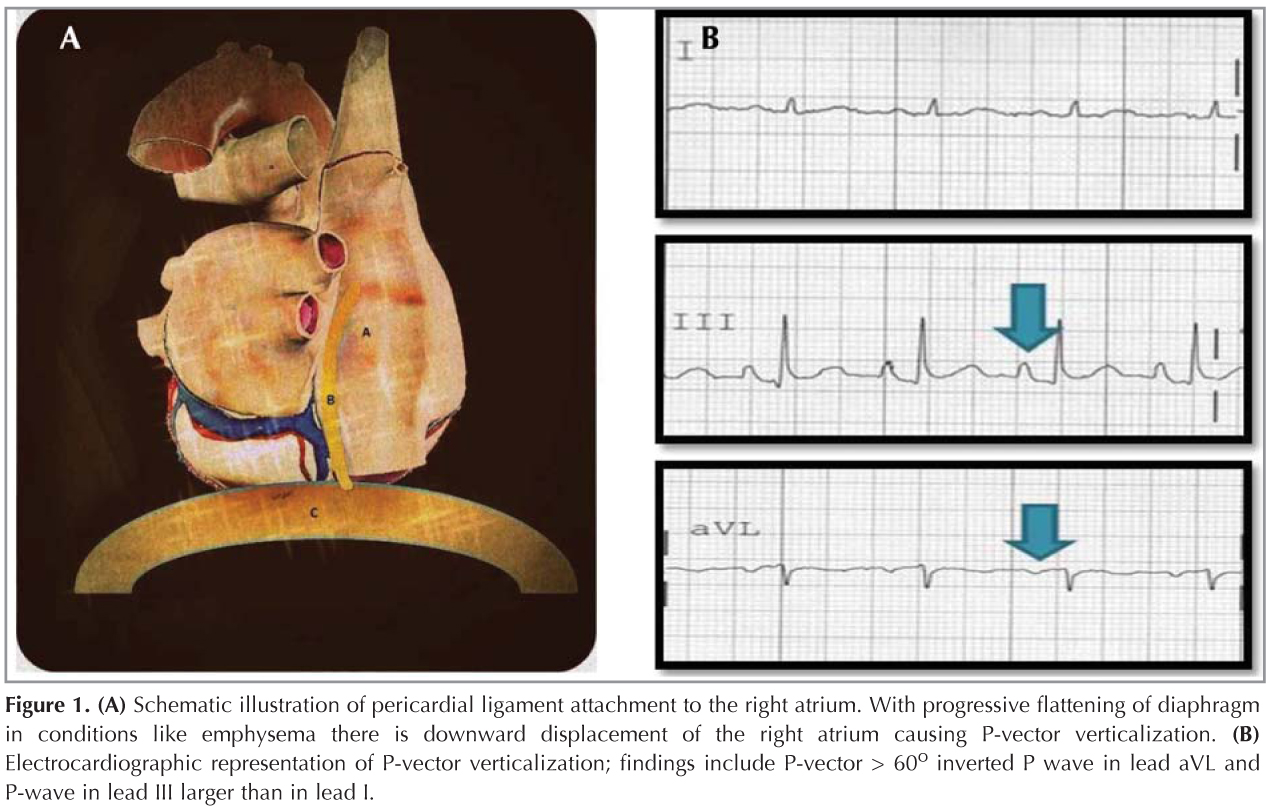
One must also remember that the P-vector verticalization in emphysema has a direct correlation with some of the other P-wave indices like terminal force in V1 (Ptf), thus caution should be employed while interpreting left atrial enlargement based on the Ptf in such patients (6). This finding could possibly be due to either net cancellation of right atrial potential by overwhelming left atrial forces, or it could be more likely due to positional displacement of the right atrium (6). P-pulmonale is a well known electrocardiographic marker for diagnosing emphysema, however interestingly in contrast to a general clinical perception, this is the least sensitive electrocardiographic marker for diagnosing pulmonary emphysema although it carries a high specificity (6). We commend the authors for reiterating the importance of electrocardiography for diagnosing pulmonary disorders such as emphysema. Given the current evidence, clinicians can use electrocardiography (an inexpensive tool) not only for routine emphysema screening, but also for assessing the disease severity. A quick look at the surface ECG for either an inverted P wave in lead aVL or the P-wave amplitude in lead III > I can serve as a quasi-diagnostic marker for emphysema (7). Clinicians should thus be aware of these valuable electrocardiographic facts for a quick diagnostic emphysema screening and should employ cautionary interpretation of other P-indices like P-tf.
CONFLICT of INTEREST
Dr. David Spodick receives royalties from his textbook, "The Pericardium: A Comprehensive Textbook (Fundamental and Clinical Cardiology), Marcel Dekker, New York 1997".
REFERENCES
- Akt?rk F, B?y?k ?, Koca? C, Ert?rk M, Yal??n AA, Sava? AU, et al. The role of electrocardiography in evaluation of severity of chronic obstructive pulmonary disease in daily clinical practice. Tuberk Toraks 2013;61(1):38-42.
- Chhabra L, Sareen P, Perli D, Srinivasan I, Spodick DH. Vertical P-wave axis: the electrocardiographic synonym for pulmonary emphysema and its severity. Indian Heart J 2012;64(1):40-2.
- Chhabra L, Sareen P, Gandagule A, Spodick D. Computerized tomographic quantification of chronic obstructive pulmonary disease as the principal determinant of frontal P vector. Am J Cardiol 2012;109(7):1046-9.
- Chhabra L, Sareen P, Gandagule A, Spodick DH. Visual computed tomographic scoring of emphysema and its correlation with its diagnostic electrocardiographic sign: the frontal P vector. J Electrocardiol 2012;45(2):136-40.
- Shah NS, Koller SM, Janower ML, Spodick DH. Diaphragm levels as determinants of P axis in restrictive vs obstructive pulmonary disease. Chest 1995;107(3):697-700.
- Chhabra L, Chaubey VK, Kothagundla C, Bajaj R, Kaul S, Spodick DH. P-wave indices in patients with pulmonary emphysema: do P-terminal force and interatrial block have confounding effects? Int J Chron Obstruct Pulmon Dis 2013;8:245-50.
- Chhabra L, Spodick DH. Electrocardiographic Screening of Emphysema: Lead aVL or Leads III and I? Acta Inform Med 2013;21(3):223.
Yaz??ma Adresi (Address for Correspondence)
Dr. Nauman KHALID
Connecticut ?niversitesi T?p Fak?ltesi,
?? Hastal?klar? Anabilim Dal?,
Hartford Hastanesi,
HARTFORD - CT
e-mail: naumankhalid84@gmail.com