LETTER TO THE EDITOR
Doi: 10.5578/tt.8345
Tuberk Toraks 2014;62(4):319-321

?lk kez Robinow sendromu olgusunda solunum yetmezli?i noninvaziv mekanik ventilasyonla tedavi edildi
Fatma ??FTC?1, S?meyye AY?Z1, Ayd?n ??LEDA?1, Ak?n KAYA1
1 Ankara ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Ankara, T?rkiye
1 Department of Chest Diseases, Faculty of Medicine, Ankara University, Ankara, Turkey
Robinow syndrome is a genetic syndrome characterized by mesomelic limb shortening, facial and genital anomalies, and skeletal disorders. In these patients restrictive lung disease and respiratory failure may develop secondary to vertebral and costal anomalies. We herein present a case of restrictive lung disease and acute hypercapnic respiratory failure due to kyphoscoliosis, which was successfully treated with non-invasive mechanical ventilation (1,2).
A 26-year-old male patient was referred to the department of chest diseases because of dyspnea, and cough for two months. Questioning the past history of the patient revealed that he had been diagnosed with Robinow syndrome at the age of 10 and repeatedly hospitalized due to frequent respiratory infections since childhood. He had also undergone mitral valve replacement at the age of 15. He was not on long-term oxygen therapy at the time of presentation.
He was born at term to unaffected consanguineous parents after an unremarkable pregnancy. Detailed clinical examination showed short stature, macrocephaly, midface hypoplasia, hypertelorism, down-slanted palpebral fissures, short neck, short nose with mildly anteverted nares, large nasal bridge, short philtrum, microretrognathia, large mouth, macroglossia, a highly arched palate, and posteriorly rotated and low set ears. His teeth were hypoplastic and crowded. There was mesomelic shortening of the extremities, hypoplasia and dislocation of the proximal end of the radius at the elbow joint, and hypoplasia of the distal end of the ulna with Madelung deformity. The hands were small with shortened distal phalanges. There were bilateral broad thumbs and flat foot (Figure 1). The patient's motor development was delayed, particularly affecting the coordination of the upper extremities. He had had first difficulty in feeding himself and later experienced problems with writing. However, his mental development was normal.

His vital signs were as follows: body temperature 37.2oC, blood pressure 120/80 mmHg, pulse rate 110 bpm, respiratory rate 20/minute.
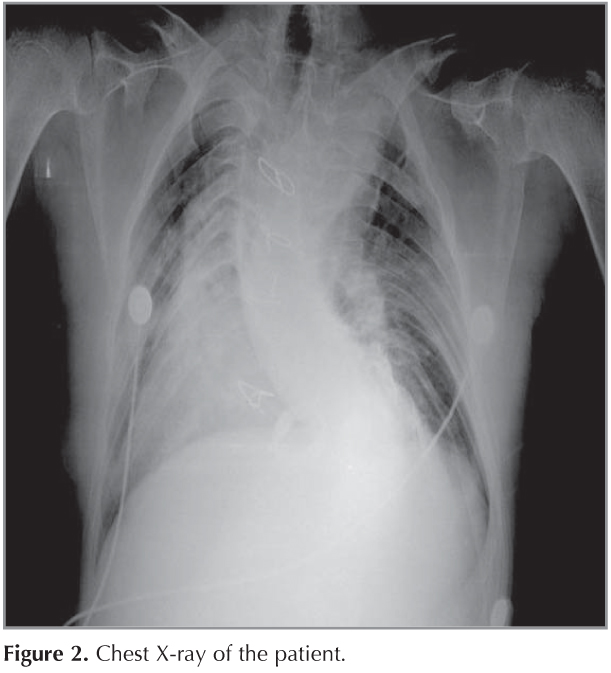
Lung auscultation revealed rales at lower zones of both lungs. Chest X-ray revealed an increased cardiothoracic index, mediastinal shift, and thoracolumbar kyphoscoliosis. The ribs were dysplastic and showed bilateral fusion (Figure 2). Arterial blood gas analysis showed respiratory acidosis (pH: 7.34), hypercapnia (pCO2: 70 mmHg), and hypoxemia (pO2: 47 mmHg). Respiratory function tests revealed restrictive flow limitation with FEV1: 1.12 L (27%), FVC: 1.53 L (32%), and FEV/FVC: 74%.
The patient was diagnosed with restrictive lung disease and hypercapnic respiratory failure. Non-invasive mechanical ventilation (NIMV) was begun via face mask in BIPAP/S mode with IPAP: 12 EPAP: 5. IPAP was later set to 18 and EPAP to 6 as dictated by the data obtained from tidal volume, respiratory frequency, and hourly arterial blood gas monitoring. NIMV therapy via BIPAP mode was delivered 10 hours per day. The patient also received nasal oxygen and bronchodilator therapy. A control arterial blood gas analysis 24 hours later revealed an improvement in hypercapnia and hypoxemia, and blood pH was compensated (PCO2: 54 mmHg, PO2: 65 mmHg, pH: 7.36).
Robinow syndrome (RS), first described in 1969. These patients were once in the pediatric age group but they have reached adulthood now. They present to healthcare centers with the health problems related to their deformities. Patients who have restrictive lung disease due to thoracic deformities as those present in Robinow syndrome who develop hypercapnic respiratory failure are candidates for NIMV therapy. Mental status of the patient should be thoroughly assessed prior to commencing NIMV therapy. As these persons may have accompanying facial disorders, an appropriate face mask should be selected (3,4).
CONFLICT of INTEREST
None declared.
REFERENCES
- Robinow M, Silverman FN, Smith HD. A newly recognized dwarfing syndrome. Am J Dis Child 1969;117:645-51.
- Hosalkar HS, Gerardi J, Shaw BA. Robinow syndrome. J Postgra Med 2002;48:50-1.
- Weksler N, Schwartz A, Klein M, Rozentsveig V, Weksler D, Guman GM. Laryngeal mask airway and the Robinow syndrome. Minerva Anestesiol 2006;72:81-3.
- Lirk P, RiederJ, Schuerholz A, Keller C. Anaesthetic implications of Robinow syndrome. Paediatr Anaesth 2003;13:725-7.
Yaz??ma Adresi (Address for Correspondence)
Dr. Fatma ??FTC?
Ankara ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
ANKARA - TURKEY
e-mail: fatmarslann@yahoo.com