LETTER TO THE EDITOR
Doi: 10.5578/tt.6786
Tuberk Toraks 2014;62(2):172-173

Lung cancer superimposed opacity of aortic arch
Koichi KURISHIMA1, Katsunori KAGOHASHI1, Hiroaki SATOH1
1 Department of Respiratory Medicine, Mito Medical Center, University of Tsukuba, Ibaraki, Japan
1 Tsukuba ?niversitesi Mito T?p Merkezi, Solunum Hastal?klar? Anabilim Dal?, Ibaraki, Japonya
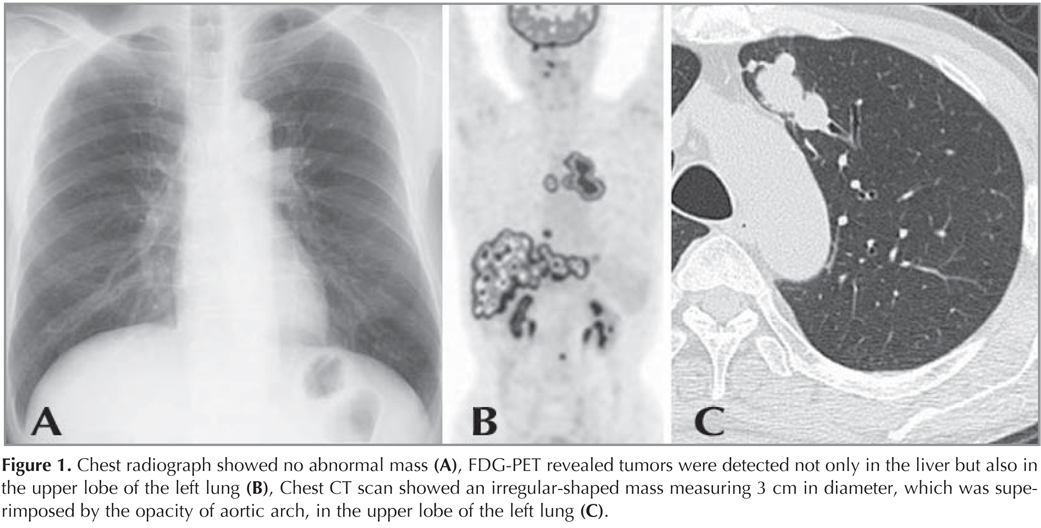
A 73-year-old man was visited our outpatient clinic complaining pain in the right upper quadrant. Abdominal echograph and CT scan revealed multiple liver masses, which were evaluated as metastatic liver tumors. Chest radiograph showed no abnormal mass, suggesting no primary lesion of the metastatic liver masses or no pulmonary metastasis from other organs (Figure 1A). Fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) was performed to assess the primary site of the metastatic liver masses. On FDG-PET, tumors were detected not only in the liver but also in the upper lobe of the left lung (Figure 1B). Chest CT scan showed an irregular-shaped mass measuring 3 cm in diameter, which was superimposed by the opacity of aortic arch, in the upper lobe of the left lung (Figure 1C). Specimens from the lung mass obtained by transbronchial biopsy proved to be a small cell lung cancer (SCLC).
The chest radiograph remains a pivotal role as the first-line imaging for initial detection of lung cancer, although imaging for staging is mainly based on CT scan. However, previous researchers reported that potentially detectable lung cancers were missed during interpretation of chest radiographs in more than 10% of patients (1,2,3,4). Missed lesions were not always small or subtle, and failure to detect them was frequently due to superimposed other normal anatomical structures (2,5,6). Among lung cancers, SCLC is an aggressive tumor and is usually detected at locally advanced or metastatic disease with a large lung mass and bulky hilar and mediastinal lymph node swelling. Liver metastases are not rare in SCLC patients and most of them had multiple nodules (7).
Although very rare, there are some patients with undetected primary lesion on chest radiograph. In such a case, FDG-PET/CT is useful in confirming exact existent of the primary tumor, which is superimposed by opacities of other anatomical structures.
CONFLICT of INTEREST
None declared.
REFERENCES
- Muhm JR, Miller WE, Fontana RS, Sanderson DR, Uhlenhopp MA. Lung cancer detected during a screening program using 4 month chest radiographs. Radiology 1983;148:609-15.
- Austin JH, Romney BM, Goldsmith LS. Missed bronchogenic carcinoma: radiographic findings in 27 patients with a potentially respectable lesion evident in retrospect. Radiology 1992;182:115-22.
- Quekel LGBA, Kessels AGH, Goei R, van Engelshoven JM. Miss rate of lung cancer on the chest radiograph in clinical practice. Chest 1999;115:720-4.
- Turkington PM, Kennan N, Greenstone MA. Misinterpretation of the chest X-ray as a factor in the delayed diagnosis of lung cancer. Postgrad Med J 2000;78:158-60.
- Kundel HL, Nodine CF, Carmody D. Visual scanning, pattern recognition and decision-making in pulmonary nodule detection. Invest Radiol 1978;13:175-81.
- Altorki N, Kent M, Pasmantier M. Detection of early-stage lung cancer: computed tomographic scan or chest radiograph. J Thorac Cardiovasc Surg 2001;121:1053-7.
- Kagohashi K, Satoh H, Ishikawa H, Ohtsuka M, Sekizawa K. Liver metastasis at the time of initial diagnosis of lung cancer. Med Oncol 2003;20:25-8.
Yaz??ma Adresi (Address for Correspondence)
Dr. Hiroaki Satoh
Tsubaka ?niversitesi Mito T?p Merkezi,
?? Hastal?klar? Anabilim Dal?,
Miya-Machi 3-2-7, Mito, 310-0015,
IBARAKI-JAPAN
e-mail: hirosato@md.tsukuba.ac.jp