SHORT REPORT
Doi: 10.5578/tt.6215
Tuberk Toraks 2014;62(2):151-153

Katamenial hemoptizi: Olgu sunumu
Aylin OKUR1, Bayram MET?N2, Yavuz Selim ?NTEPE3, Halil ?brahim SER?N1
1 Department of Radiology, Faculty of Medicine, Bozok University, Yozgat, Turkey
1 Bozok ?niversitesi T?p Fak?ltesi, Radyoloji Anabilim Dal?, Yozgat, T?rkiye
2 Department of Thoracic Surgery, Faculty of Medicine, Bozok University, Yozgat, Turkey
2 Bozok ?niversitesi T?p Fak?ltesi, G???s Cerrahisi Anabilim Dal?, Yozgat, T?rkiye
3 Department of Chest Disease, Faculty of Medicine, Bozok University, Yozgat, Turkey
3 Bozok ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Yozgat, T?rkiye
?ZET
Katamenial hemoptizi: Olgu sunumu
Bu yaz?da, mensturasyon d?neminde tekrarlayan hemoptizi ?ikayetiyle ba?vuran 25 ya??nda kad?n hasta sunulmaktad?r. Mensturasyon d?neminde ?ekilen toraks tomografisinde sol akci?er alt lob s?periyorda buzlu cam dansitesi ve asiner nod?ler g?r?n?mler saptand?. Mensturasyon d??? d?nemde ?ekilen toraks tomografisi normaldi. Klinik ve radyolojik bulgular? ile katamenial hemoptizi d???n?ld?. Akci?erde nadir g?r?len bir hastal?k olan pulmoner endometriyozis olgusunu, literat?r e?li?inde sunuyoruz.
Anahtar kelimeler: Hemoptizi, mensturasyon, pulmoner endometriyozis
SUMMARY
Catamenial hemoptysis: a case report
Herein we present a 25-year-old female patient who was admitted with recurrent hemoptysis in menstrual period. At the thorax computed tomography taken during menstruation of patient, diffuse ground glass density and acinar nodules at superior segment of lower lobe at left lung were detected. There was no this findings at the thorax tomography taken in non-menstruation period. Therefore, patient was considered catamenial hemoptysis with clinical and radiological findings. Pulmonary endometriosis is rarely seen disease of the lung, so we are presenting it in the light of the literature knowledge.
Key words: Hemoptysis, menstrual period, pulmonary endometriosis
INTRODUCTION
Thorax is a rare site of endometriosis (1). Endometriosis of the lung is associated with catamenial hemoptysis, hemothorax, pneumothorax and chest pain (2). Catamenial hemoptysis is very rare disorder that is characterized by hemoptysis occuring concomitant with menstruation in female patients (3). We aimed to present case of 25 year old who was diagnosed as catamenial hemoptysis by clinic and multidetector computed tomography (MDCT) with literature.
CASE REPORT
Twenty five year old female patient attended to chest surgery clinic with complaints of hemoptysis presenting for five months and repeating at menstruation period. She had history of one parturition with normal vaginal way. She had no history of smoking. Hemoptysis was present for every menstruation period which lasted for about five days and a total amount of a cup of tea. Patient had taken three thorax computed tomography (CT) at outer clinics, two of them at menstrual period and one non-menstrual period. Diffuse ground glass density and acinar nodules in the superior segment of the left lower lobe was present on CT taken at our clinic in menstrual period which was compatible with CTs taken at outer clinic in menstrual period. There was not abnormal finding at CT taken at outer clinic in period of non-menstruation. The pathological finding did not reveal at bronchoscopy. Primarly hormone therapy was suggested to the case which was thought as catamenial hemoptysis with existing findings. Patient did not accept hormone therapy. Upon this, video thoracoscopic wedge resection was proposed according to observing source of bleeding bounding in the superior segment of the left lower lobe at CTs. Patient was obliged to discharge due to desisting surgery after accepting surgery and planning preoperation arrangements.
Discussion
Endometriosis is the presence of functional endometrial tissue in extrauterine sites. It is most commonly localized in the ovaries, uterosacral ligaments and peritoneum. Thoracic endometriosis is a rare from of extrapelvic endometriosis. Endometrial tissue may be within the pleura, the lung parenchyma or the airways in thoracic endometriosis. In menstruation period, clinic emerge according to changes at areas where endometrial tissue present due to circulating sex hormones (1). The pathogenesis of thoracic endometriosis is not clear. Hypotheses for the spread of endometrial tissue have been explained microembolization theory, peritoneal-pleural migration and coelomic metaplasia. Microembolization theory states that endometrial tissue can be transported via pelvic vasculary channels or lymphatics. Peritoneal-pleural migration theory states that endometrial tissue reaches the thorax as retrograde through diaphragmatic defect. Coelomic metaplasia theory states that mesothelial cells differentiated into endometrial cells (4). But, this theories is debated. Obstetric or gynecologic procedures may be an important risk factor for catamenial hemoptysis (5). Recently, new insights have been proposed about etiology and patogenesis of this disease such as genetic susceptibility, environmental factors, the immun system, intrinsic endometrial abnormalities and the secreted products of endometrial lesions (6).
Pulmonary endometriosis has varying clinical manifestations such as pneumothorax, hemothorax, hemoptysis and pulmonary nodules and the most common of them is catamenial pneumothorax (73%) (7). Other presentations include catamenial hemothorax (14%), catamenial hemoptysis (7%) and pulmonary nodules (6%). A clinical picture of hemoptysis concurrent with menstrual periods helps to differentiate catamenial hemoptysis from hemoptysis of the other causes (1).
Thorax CT is the modality of choice for localization of endometrial deposits in the lung and pleura but radiologic findings are usually non-spesific. The CT findings of pulmonary endometriosis may include well-defined opacities, nodular lesions, thin-wall cavities (8). Kim et al. reported that ground glass opacities were most commonly appeared on thorax CT (9). In our patient, the CT images taken durig her menstrual period showed a ground glass opacity and acinar nodules in the superior lingual segment of left lung. Any lesion or opacity was seen at CT taken at outer clinic in non-menstruation period. Lung lesions are usually present at right lung and lower lobes (9). In our case, lesion was in the superior segment of lower lobe at left lung.
The utility of bronchoscopy is limited because most cases of pulmonary endometriosis involve the distal parenchyma and therefore bronchoscopic examination of the air ways usually obtains normal findings as in our case. CT guided aspiration or biopsy is also difficult, because biopsy or resected specimens should be obtained just before the onset of menstrual period (1).
Medical and surgical treatment options can be considered for the treatment of pulmonary endometriosis. Danazol and Gonadotropin releasing hormon (GnRH) are the treatment of choice for pulmonary endometriosis. Medical therapy is expensive, and the symptoms may be repeated after it is discontinued. But, these drugs have side effects like menopausal symptoms (10). Therefore, hormonal therapy would not be preferred for young women of reproductive age. The indications for pulmonary surgical procedure are medical therapy failure, adverse effects, recurrent symptoms after stopping hormonal therapy (1).
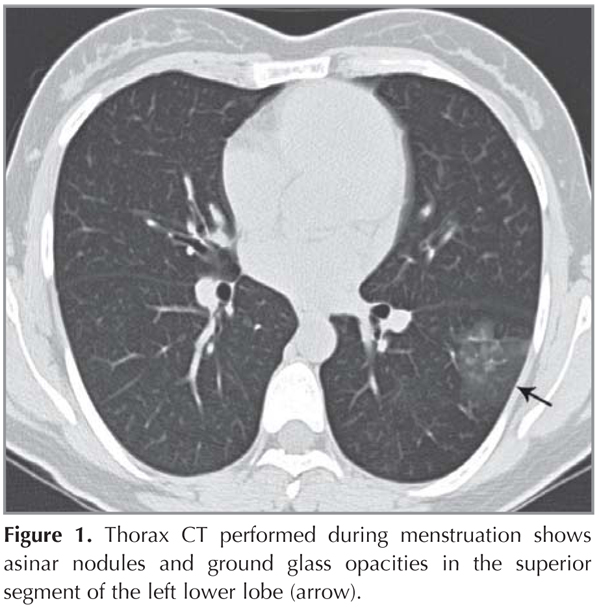
At presenting case, diffuse ground glass density and acinar nodules in the superior segment of lower lobe at left lung at CT taken simultaneously was present at our patient who has hemoptysis repeating in menstruation period and CT taken in non-menstrual period was normal (Figure 1). These findings combined with clinical was thought catamenial hemoptysis.
As a result, pulmonary endometriosis should be considered at cases of hemoptysis related with menstruation. Bronchoscopic findings may be normal in these patients. For this reason, comparison of thorax CTs which will be taken in menstruation and non-menstruation period is very important to support diagnosis.
CONFLICT of INTEREST
None declared.
REFERENCES
- Augoulea A, Lambrinoudaki I, Christodoulakos G. Thoracic endometriosis syndrome. Respiration 2008;75:113-9.
- Giudice LC, Kao LC. Endometriosis. Lancet 2004;364:1789-99.
- Joseph J, Sahn SA. Thoracic endometriosis syndrome: new observations from an analysis of 110 cases. Am J Med 1996;100:164-70.
- Alifano M, Trisolini R, Cancellieri A, Regnard JF. Thoracic endometriosis: current knowledge. Ann Thorac Surg 2006;81:761-9.
- Kervancioglu S, Andic C, Bayram N, Telli C, Sarica A, Sirikci A. Bronchial artery embolization in the management of pulmonary parenchymal endometriosis with hemoptysis. Cardiovasc Intervent Radiol 2008;31:824-7.
- Pergialiotis V, Lagkadas A, Polychronis O, Natsis S, Karakalpakis D, Giannakopoulos K. Endometriosis-associated ovarian cancer. Presentation of a case report and review of the literature. Eur J Gynaecol Oncol 2011;32:682-5.
- Lee YR, Choi YW, Jeon SC, Paik SS, Kang JH. On the AJR viewbox. Pleuropulmonary endometriosis: CT-pathologic correlation. AJR Am J Roentgenol 2006;186:1800-1.
- Orriols R, Mu?oz X, Alvarez A, Sampol G. Chest CT scanning: utility in lung endometriosis. Respir Med 1998;92:876-7.
- Kim CJ, Nam HS, Lee CY, Yum HK, Yang SH, Seo KH, et al. Catamenial hemoptysis: a nationwide analysis in Korea. Respiration 2010;79:296-301.
- Hong YJ, Paik HC, Kim HJ, Lee DY, Kim SJ, Cho SH, et al. A case of parenchymal pulmonary endometriosis. Yonsei Med J 1999;40:514-7.
Yaz??ma Adresi (Address for Correspondence)
Dr. Aylin OKUR
Bozok ?niversitesi T?p Fak?ltesi,
Radyoloji Anabilim Dal?,
YOZGAT - TURKEY
e-mail: draylinokur@hotmail.com