SHORT REPORT
Doi: 10.5578/tt.6872
Tuberk Toraks 2014;62(2):147-150

K???k h?creli akci?er kanseri, cilt metastaz?
Koichi KURISHIMA1, Katsunori KAGOHASHI1, Gen OHARA1, Kunihiko MIYAZAKI2, Mio KAWAGUCHI2,
Norio TAKAYASHIKI3, Hiroaki SATOH1
1 Department of Respiratory Medicine, Mito Medical Center, Tsukuba University, Ibaraki, Japan
1 Tsukuba ?niversitesi Mito T?p Merkezi, Solunum Hastal?klar? Anabilim Dal?, Ibaraki, Japonya
2 Department of Respiratory Medicine, Faculty of Medicine, Tsukuba University, Ibaraki, Japan
2 Tsukuba ?niversitesi T?p Fak?ltesi, Solunum Hastal?klar? Anabilim Dal?, Ibaraki, Japonya
3 Department of Pathology, Mito Medical Center, Tsukuba University, Ibaraki, Japan
3 Tsukuba ?niversitesi Mito T?p Merkezi, Patoloji Anabilim Dal?, Ibaraki, Japonya
?ZET
K???k h?creli akci?er kanseri, cilt metastaz?
Cilt metastaz? olan olgularda daima bir?ok organda yayg?n metastazlar bulunmaktad?r. Burada, k???k h?creli akci?er kanser (KHAK)'li ve cilt metastazl? nadir g?r?len bir olgu sunulmaktad?r. Hasta platin- bazl? kemoterapi ile tedavi edildi ve tedavi yan?t?, parsiyel yan?t olarak de?erlendirildi. Hastal?k yava? seyirli bir progresyon g?sterdi ve olgu tan?dan 16 ay sonra kaybedildi. KHAK'li hastalarda tipik olsun olmas?n deri lezyonlar? saptand???nda, biyopsi d???n?lmelidir. En s?k tutulum b?lgesi g?vde olmas?na ra?men, KHAK'li hastalarda b?yle lezyonlar g?r?ld???nde ??phelenilmesi ?nemlidir.
Anahtar kelimeler: Cilt metastaz?, k???k h?creli akci?er kanseri
SUMMARY
Skin metastasis from small cell lung cancer
Patients with skin metastasis always had disseminated metastases in many organs. We herein report an unusual case with skin metastasis from small cell lung cancer (SCLC). The patient was treated with platinum-containing chemotherapy, and the response to the therapy was evaluated as partial response. The patient had slowly progressive disease and died of SCLC 16 months after the diagnosis of the diseases. If skin lesions, whether it may be typical or not, are found in SCLC patients, biopsy from the lesion would be considered to perform. Although trunk may be the most common sites, it is important to suspect such metastasis occurs in patients with SCLC.
Key words: Skin metastasis, small cell lung cancer
Introduction
Skin metastasis implies that cancer cells may reach many sites of the whole body via the bloodstream and the lymphatic system. We herein report an unusual case with skin metastasis from small cell lung cancer (SCLC).
Case report
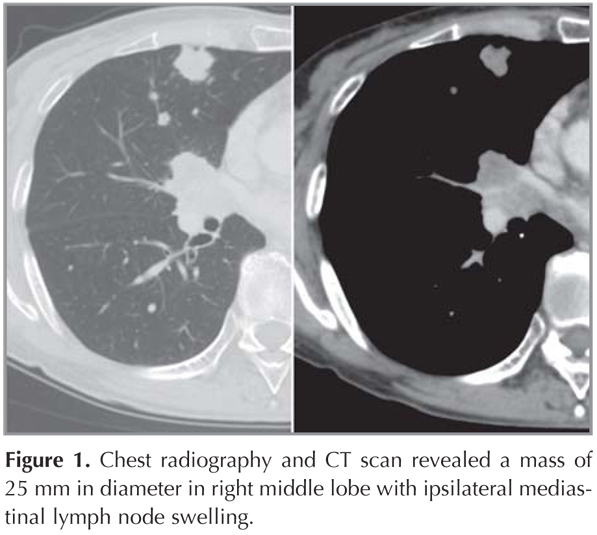
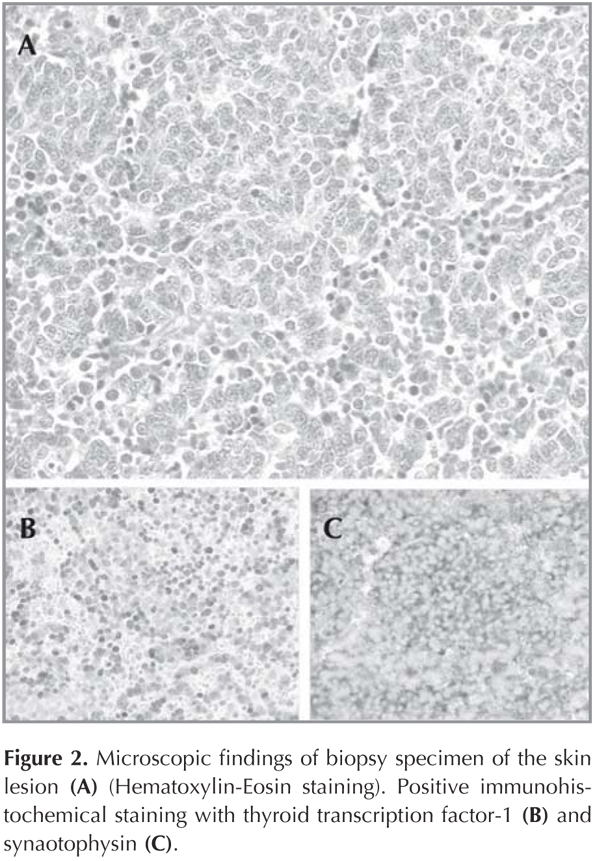
A 66-year-old woman with a 40-pack/year history of smoking presented with skin nodule on the back and lumbago. Physical examination revealed a painless, movable and round solitary nodule of approximately 15 mm in diameter on her right back. She had knock pain on lumbar spine. Chest radiography and CT scan revealed a mass of 25 mm in diameter in right middle lobe with ipsilateral mediastinal lymph node swelling (Figure 1). Bone scan showed lumbar spinal metastases. Biopsy specimen of the skin lesion was performed. Immunohistochemical staining with thyroid transcription factor-1 and synaotophysin were positive (Figure 2). Together with histopathological findings, the patient was diagnosed as having skin metastasis from SCLC. A transbronchial curetting cytology from the mass in right lung was done and it was confirmed same histopathological findings (Figure 3). The diagnosis of SCLC with bone and skin metastases was established. She was started on chemotherapy using carboplatin and etoposide and irradiation to the lumbar spine. The response to the chemotherapy was evaluated as partial response (Figure 4). The patient had slowly progressive disease and died of SCLC 16 months after the diagnosis of the diseases.


Discussion
In the PubMed database, we found 20 cases with skin metastasis from SCLC (1,2,3,4,5,6,7,8,9,10,11,12). Among them, precise clinical courses were described in 15 cases (2,3,4,5,6,7,8,9,10,11). Table 1 showed the clinical features of SCLC patients with skin metastasis. Same as the other internal cancers, most common sites of the skin metastasis from SCLC are the trunk of the body such as chest and back but we found a case with arm and facial skin metastasis (1,2,3,4,5). Size of skin metastasis was 5-50 mm in diameter (1,2,3,4,5). Most of them were less than 20 mm in diameter (2,3,5,6,9,10,11). Various shapes were found in skin metastasis such as nodular, inflammatory, and the most lesions were firm, raised, and hemispherical, covered by an intact epidermis, while some patients had ulcerated lesions (2,3,6,8,9). In our patient, it was a painless, movable and round solitary nodule of approximately 15 mm in diameter. Upper lobe of the lung on either side was the most common primary site of SCLC (2,4,9,10). There were only four patients whose primary site of SCLC was lower lobe of the lung (2,3,6,11). There was no patient whose primary site was middle lobe of the lung as observed in our case.
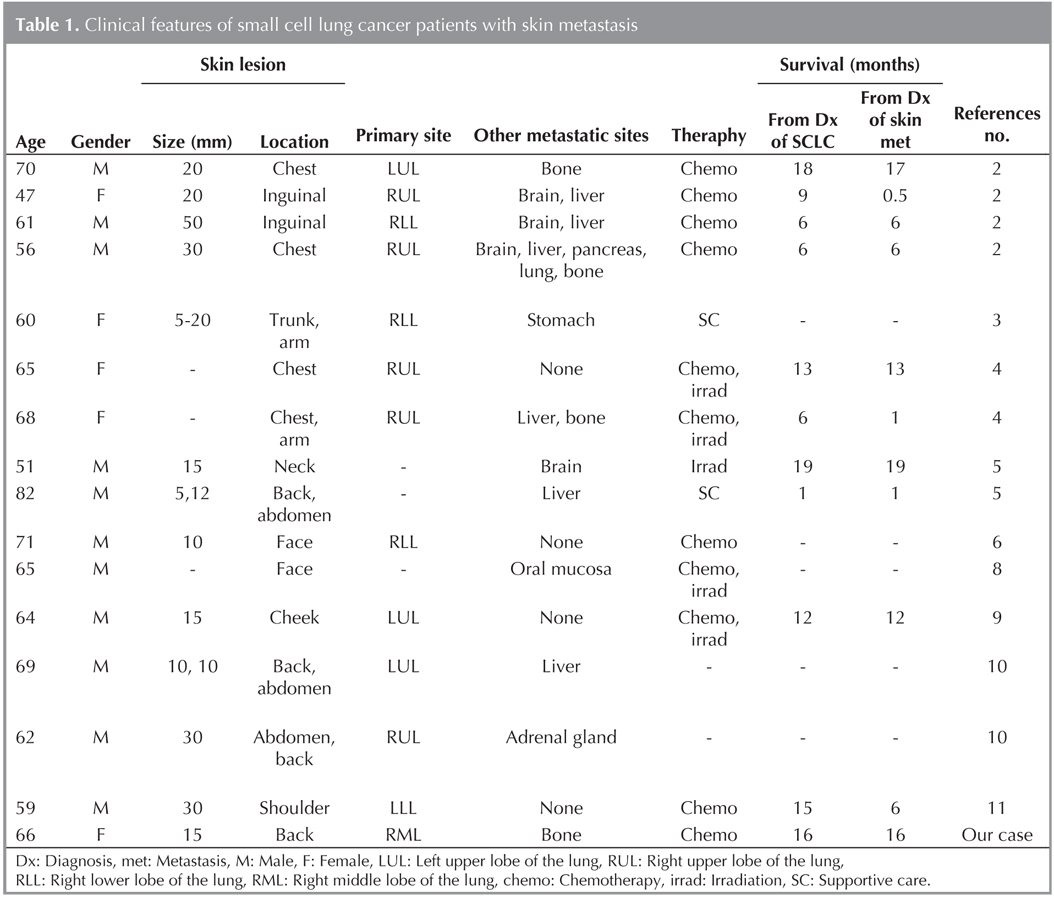
Among the 15 SCLC patients, skin metastasis was found only one site in 12 patients (2,6,9,10,11). The rest of the three patients had skin metastases at two or more sites (3,5,10). Interestingly, 11 (73.3%) of the 15 patients had other metastatic sites than skin. The three of the commonest sites were liver, bone, and brain (2,4,5,10). However, four patients had skin metastasis without any metastatic sites (2,6,9,11). The explanation why distant metastasis was defined by skin lesion in these patients was beyond our knowledge. This might imply that sub-centimeter skin metastatic lesions cannot found in physical examination even cancer cells may reach many sites of the whole body via the bloodstream and the lymphatic system, or that specific mechanism may be exist to develop such a rare metastasis even the progression of the primary malignancy. In our patient, skin metastasis was found in the back, which was the most common site of skin metastasis, but it developed in only one site, and there was not found any additional skin metastasis in her clinical course.
With regard to the treatment for the skin lesion, surgical resection of the lesion and systemic chemotherapy were the common and irradiation to the skin metastasis was performed in one patient (2,4,5,6,8,9). In our patient, we performed surgical resection of the lesion and systemic chemotherapy, and there was no recurrence in the skin lesion. Survival time after the diagnosis of skin metastasis was short because patients with skin metastasis always had disseminated metastases in many organs. However, four of them survived more than a year, and our patient had slowly progressive disease and died 16 months after the diagnosis of skin metastasis (1,2,3,4,5). There may be some slowly progressive SCLC patients or some chemotherapy sensitive SCLC patients among those with skin metastasis.
As shown in Table 1, skin metastasis was found at the time of initial diagnosis of SCLC in 6 patients including our case (2,4,5,9). Skin metastasis developed 1 to 9 months after the diagnosis of SCLC during their clinical courses in 4 patients (2,4,11). Taking these results into consideration, chest physicians should recognize and be alert on the development of skin metastasis not only at the time of diagnosis and in their clinical courses, although it is very rare. If skin lesions, whether it may be typical or not, are found in SCLC patients, biopsy from the lesion would be considered to perform. It is important to suspect such metastasis occurs in patients with SCLC not only in the trunk, the most common site, but also in others sites.
CONFLICT of INTEREST
None declared.
REFERENCES
- Matsukawa A, Furusugi Y. A case of skin metastasis of lung carcinoma associated with superior vena cava syndrome. J Dermatol 1989;16:508-10.
- Coslett LM, Katlic MR. Lung cancer with skin metastasis. Chest 1990;97:757-9.
- Maeda J, Miyake M, Tokita K, Iwahashi N, Nakano T, Tamura S, et al. Small cell lung cancer with extensive cutaneous and gastric metastases. Intern Med 1992;31:1325-8.
- Terashima T, Kanazawa M. Lung cancer with skin metastasis. Chest 1994;106:1448-50.
- Hidaka T, Ishii Y, Kitamura S. Clinical features of skin metastasis from lung cancer. Intern Med 1996;35:459-62.
- De Argila D, Bureo JC, M?rquez FL, Pimentel JJ. Small-cell carcinoma of the lung presenting as a cutaneous metastasis of the lip mimicking a Merkel cell carcinoma. Clin Exp Dermatol 1999;24:170-2.
- D'Aniello C, Brandi C, Grimaldi L. Cutaneous metastasis from small cell lung carcinoma. Case report. Scand J Plast Reconstr Surg Hand Surg 2001;35:103-5.
- Senen D, Adanali G, Tuncel A, Erdo?an B. Oat cell lung cancer diagnosed following metastasis to the skin. Plast Reconstr Surg 2003;111:510-1.
- Barbetakis N, Samanidis G, Paliouras D, Samanidou E, Tzimorota Z, Asteriou C, et al. Facial skin metastasis due to small-cell lung cancer: a case report. J Med Case Rep 2009;3:32.
- Dhambri S, Zendah I, Ayadi-Kaddour A, Adouni O, El Mezni F. Cutaneous metastasis of lung carcinoma: a retrospective study of 12 cases. J Eur Acad Dermatol Venereol 2011;25:722-6.
- Simsek GG, Karadag AS, Turksen Z. Cutaneous metastasis of the small cell lung cancer. Indian J Dermatol Venereol Leprol 2011;77:537.
- Marcoval J, Pen?n RM, Llatj?s R, Mart?nez-Ballar?n I. Cutaneous metastasis from lung cancer: Retrospective analysis of 30 patients. Australas J Dermatol 2012;53:288-90.
Yaz??ma Adresi (Address for Correspondence)
Dr. Hiroaki Satoh
Tsukuba ?niversitesi Mito T?p Merkezi,
?? Hastal?klar? Anabilim Dal?,
Miya-machi 3-2-7, Mito, 310-0015,
IBARAKI - JAPAN
e-mail: hirosato@md.tsukuba.ac.jp