LETTER TO THE EDITOR
Doi: 10.5578/tt.5721
Tuberk Toraks 2014;62(1):98-99

Osteoporoz: Silikozisle ?li?kili Olabilir mi?
Mustafa Turgut YILDIZG?REN1, Timur EK?Z2, T?rkan NAD?R ?Z??3, Ali Erdem BAK?1, Engin TUTKUN4,
Ne?e ?ZG?RG?N2
1 Ankara Meslek Hastal?klar? Hastanesi, Fiziksel T?p ve Rehabilitasyon B?l?m?, Ankara, T?rkiye
1 Department of Physical Medicine and Rehabilitation, Ankara Occupational Diseases Hospital, Ankara, Turkey
2 Ankara Fizik Tedavi ve Rehabilitasyon E?itim ve Ara?t?rma Hastanesi, Fiziksel T?p ve Rehabilitasyon B?l?m?,
Ankara, T?rkiye
2 Department of Physical Medicine and Rehabilitation, Ankara Physical Therapy and Rehabilitation Hospital, Ankara, Turkey
3 Ankara Meslek Hastal?klar? Hastanesi, G???s Hastal?klar? B?l?m?, Ankara, T?rkiye
3 Department of Chest Diseases, Ankara Occupational Diseases Hospital, Ankara, Turkey
4 Ankara Meslek Hastal?klar? Hastanesi, Toksikoloji B?l?m?, Ankara, T?rkiye
4 Department of Toxicology, Ankara Occupational Diseases Hospital, Ankara, Turkey
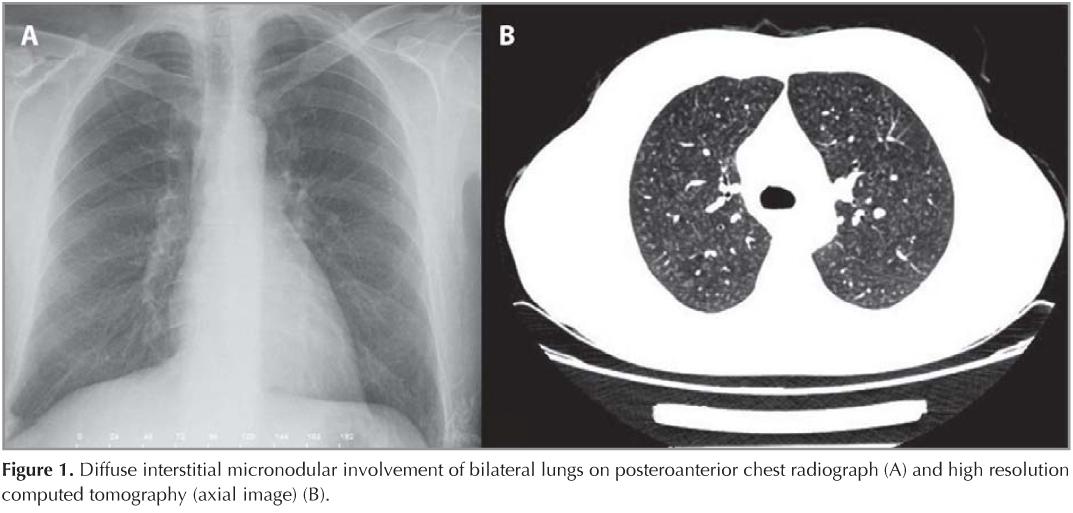
A 45-year-old male admitted to our clinic for cough and dyspnea. In his previous history, he worked at quartz mine eight hours per day for 15 years. Physical examination was not remarkable. Posteroanterior radiograph and chest computed tomography findings were consistent with pulmonary silicosis (Figure 1). Spirometry results (FEV1: 96%, FVC: 95%, FEV1/FVC: 82 MEF25-75: 94%) and the diffusing capacity for carbon monoxide (DLCO: 119 mmol/kPa/min) were normal. T-score of femoral neck was -2.99 (0.7338 g/cm2) and that of lumbar 2-4 vertebra was -3.17 (0.7186 g/cm2) in his bone mineral densitometry. He was 177 cm tall and weighed 70 kg. He had no history of osteoporosis risk factors (medical and drug history, smoking, coffee-alcohol consumption, immobility). Laboratory findings for secondary causes of osteoporosis including complete blood count, erythrocyte sedimentation rate, liver and renal function tests, thyroid and parathyroid hormone levels, prolactin, free testosterone, immunoglobulin-E and beta-2 microglobulin, calcium, phosphor, alkaline phosphatase, 25-OH vitamin D, plasma cortisol level, gonadotropins, parathyroid hormone levels and urine tests were all normal except for the high level of serum osteocalcin (24.99 ng/mL "N: 3.1-13.7 ng/mL"). Moreover, the patient did not reveal a history of malabsorption. Total protein and albumin levels were normal. After all, the patient was diagnosed as silicosis and secondary interstitial lung disease and secondary osteoporosis possibly due to silicosis intoxication. In addition to calcium rich diet and exercise, alendronate 70 mg/week and a daily calcium 600 mg plus vitamin D 400 IU were prescribed.
Silicosis is a type of pneumoconiosis characterized by fibrosis in lungs due to the reaction after inhalation of silicate dusts. It is seen as an occupational disease where silicate crystals are fractured into microcrystal forms (quartz mine, cement, ceramics industries, denim sendblasting) (1). While essential amount of silicon has favorable effects on bone and connective tissue formation and bone mineral density, the increased amount of silicone has inhibitive and toxic effects (2). Whereas osteoporosis was shown in silicotic horses, there is limited data and this relationship was not clearly shown (3). As far as we know, our paper is the first paper reporting osteoporosis in silicosis. Herein presenting our case, we would like to draw attention to the fact that osteoporosis can be seen in patients with silicosis. Inflammatory reaction in the lungs and other organs, immobility due to impairment, corticosteroid treatment (for acute silicosis and autoimmunity) and increased immunologic reactions can be the underlying mechanisms for osteoporosis in silicosis (1,4,5). In this regard, osteoporosis must be kept in mind in relevant patients with silicosis as well and clinicians should be careful for medical planning. However, further studies are required to show exact relationship. Besides, silicosis is irreversible and there is no effective treatment; on the other hand it is completely preventable (1). For this reason, we once again emphasize the importance of prevention strategies (dust control measures, use of protective mask) to decrease silicosis incidence.
CONFLICT of INTEREST
None declared.
REFERENCES
- Thomas CR, Kelley TR. A brief review of silicosis in the United States. Environ Health Insights 2010;4:21-6.
- Arens AM, Barr B, Puchalski SM, Poppenga R, Kulin RM, Anderson J, et al. Osteoporosis associated with pulmonary silicosis in an equine bone fragility syndrome. Vet Pathol 2011;48:593-615.
- Jugdaohsingh R. Silicon and bone health. J Nutr Health Aging 2007;11:99-110.
- Liu HB, Yan B, Han B, Sun JK, Yang Y, Chen J. Determination of ameliorable health impairment influencing health-related quality of life among patients with silicosis in China: a cross-sectional study. J Int Med Res 2011;39:1448-55.
- Steenland K, Goldsmith DF. Silica exposure and autoimmune diseases. Am J Ind Med 1995;28:603-8.
Yaz??ma Adresi (Address for Correspondence)
Dr. Timur EK?Z
Ankara Fizik Tedavi ve
Rehabilitasyon E?itim ve Ara?t?rma Hastanesi,
Fiziksel T?p ve Rehabilitasyon B?l?m?,?
ANKARA - TURKEY
e-mail: timurekiz@gmail.com