?ntratorasik benign hastal??a minimal invaziv yakla??mlar
Hussein ELKHAYAT1, Mahmoud KHAIRY1, Ahmed ELMINSHAWY1, Dalia BADARI2
1 Department of Cardiothoracic Surgery, Assiut University Hospital, Assiut, Egypt,
2 Department of Pathology, Assiut University Hospital, Assiut, Egypt
Tuberk Toraks 2013; 61(3): 260-262 • doi:10.5578/tt.5539
Geli? Tarihi/Received: 25/06/2013 - Kabul Edili? Tarihi/Accepted: 09/07/2013
Benign lesions should preferably be approached through minimal invasive approach, although many surgeons still believe that minimal invasive surgery is not suitable in some benign intrathoracic pathologies due to size wise or adhesions from inflammatory process. We believe that every patient with a benign intrathoracic disease should be offered a minimal invasive approach as most of these patients are young, healthy with minimal or no symptoms so it is important to minimize chest trauma and its consequences. We would like to thank the authors of the letter to the editor "An incidental unique mediastinal mass in anasymptomatic young patient: thymolipoma "[1] for their wonderful results but we just represent our case with nearly similar pathology, mediastinal lipoma, which was successfully managed by VATS approach.
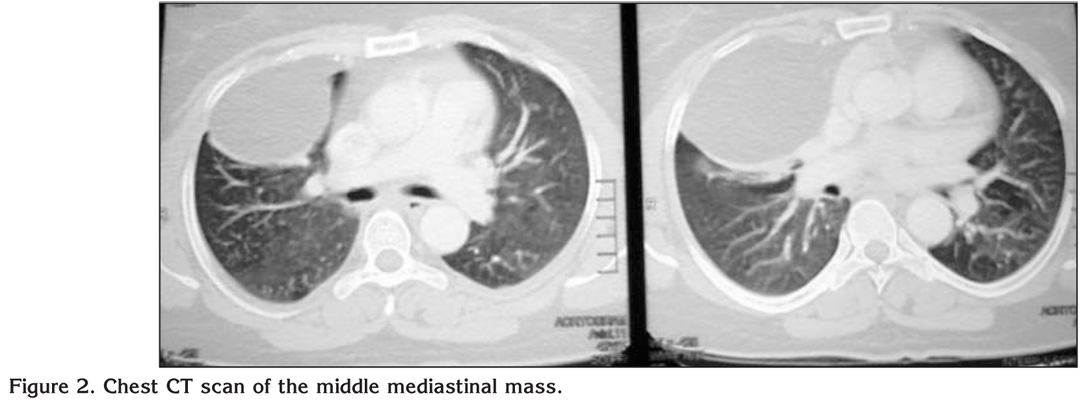
Forty three years old female patient complain from dry irritant cough, examination was free except for slight diminished air entry on the right middle lung zone. chest X-ray showed well circumscribed homogenous mass confirmed with chest CT scan to be middle mediastinal benign featuring mass (Figure 1,2). Preoperative work up were normal lab investigation and cardiac function with echocardiography.

Decision was to explore the chest with thoracoscope first to assess the mass and it relation and adherence to the neighboring structures and try to deal with it using VATS technique if proven to be benign mass.
Under general anaesthesia using double lumen endotracheal tube. Camera port were inserted in the 6th intercostal space mid axillary line intraoperative exporation revealed capsulated mass not infiltrating the surrounding structure.we proceed with VATS resection of the mass using 3 ports technique, the formal port for the camera on the 6th intercostals space midaxilary line , utility port on the 4th intercostals space on the anterior axillary line and a posterior instrument port on the 5th intercostals space posterior axillary line. Excision were conducted through opening the capsule and piece meal removal of the mass from inside then remove the capsule after evacuation of the mass from within (Figure 3).

Hemostasis, closure of the post sites and using the anterior utility port as a site for chest tube drainage (Figure 4). Postoperative course was smooth with removal of the tube on the 2nd postoperative day and patient discharge home on the 5th day (Figure 5). Routine follow up visits showed nicely healed wound and no recurrence detected on 1 year follow up (Figure 6).


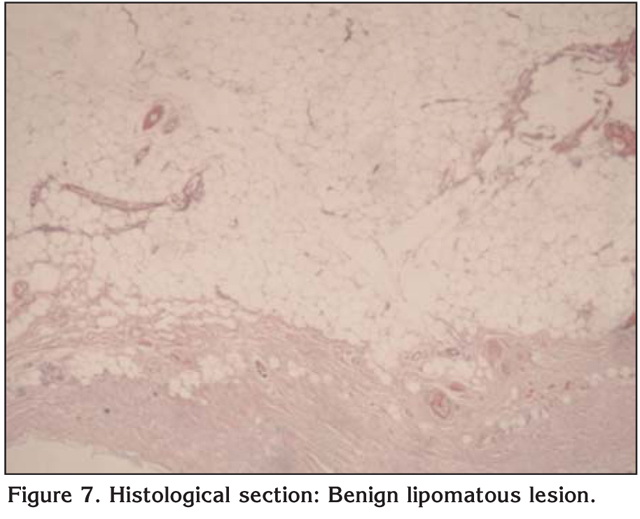
Pathology report revealed tumor tissue composed of mature adipocytes vary only slightly in size and shape and have small eccentric nuclei. No malignancy could be detected in sections examined. The histological picture is consistent with benign lipomatous lesion of mediastinal mass (Figure 7).
Again, pathology different in our case than your case but what they share is the benign character of both and the possibility of removal using piece meal technique without compromise of the surgical principles. We would like to thank the authors for their wonderful results but we just represent our case with near similar pathology, mediastinal lipoma, which was successfully managed by VATS approach.
CONFLICT of INTEREST
None declared.
REFERENCE
- U?ra? N, Aky?ld?z E?, ?nal N, Bayram AS. An incidental unique mediastinal mass in an asymptomatic young patient: thymolipoma. Tuberk Toraks 2013; 61: 78-80.
Yaz??ma Adresi (Address for Correspondence):
Dr. Hussein Elkhayat,
Department of Cardiothoracic Surgery,
Assiut University Hospitals, 71526
ASSIUT - EGYPT
e-mail: dr_khayat@hotmail.com