Bir yenido?anda A grubu beta-hemolitik streptokok ili?kili plevral ampiyem: Olgu sunumu
Sara EROL, Dilek D?LL?, Banu AYDIN, Nurdan D?NLEN, Ay?eg?l ZENC?RO?LU, Nurullah OKUMU?
Dr.
Sami Ulus Kad?n Do?um ?ocuk Sa?l??? ve Hastal?klar? E?itim ve Ara?t?rma Hastanesi,
Yenido?an Klini?i,
Ankara.
?ZET
Bir yenido?anda A grubu beta-hemolitik streptokok ili?kili plevral ampiyem: Olgu sunumu
Plevral ampiyem pn?moninin nadir ve ciddi bir komplikasyonudur. ?ocuklarda s?k g?r?lmesine ra?men yenido?anda plevral ampiyemle ilgili az say?da veri bulunmaktad?r. Bu yaz?da, erken ba?lang??l? neonatal pn?moniyi takiben geli?en bir plevral ampiyem olgusu sunuldu. Etken mikroorganizma olas?l?kla lohusal?k d?neminde infeksiyonu olan anneden kaynaklanan grup A beta-hemolitik streptokok (GAS veya Streptococcus pyogenes) idi. Annede do?umdan iki g?n sonra ba?layan ate?, pelvik a?r?, anormal vajinal ak?nt? ve serum antistreptolizin O titresi y?ksekli?i streptokokal infeksiyonu destekledi. Hasta plevral drenaj ve sinerjistik antibiyotik tedavisiyle ba?ar?l? bir ?ekilde tedavi edildi.
Anahtar Kelimeler: Streptococcus pyogenes, yenido?an, plevral ampiyem.
SUMMARY
Pleural empyema due to group A beta-hemolytic streptococci in a newborn: case report
Sara EROL, Dilek D?LL?, Banu AYDIN, Nurdan D?NLEN, Ay?eg?l ZENC?RO?LU, Nurullah OKUMU?
Clinic
of Neonatology, Dr. Sami Ulus Maternity and Children Health and Diseases
Training and
Research Hospital, Ankara, Turkey.
Pleural empyema is a rare and serious complication of pneumonia. Although it is frequently seen in children, there are only a few reports about pleural empyema in newborn infants. Here we report a case of early onset neonatal pneumonia complicated with pleural empyema. The causal microorganism was group A beta-hemolytic streptococci (GAS or Streptococcus pyogenes) presumably originating from the mother, who had a puerperal infection. The mother had fever, pelvic pain, and abnormal vaginal discharge two days after delivery and subsequent increase in the antistreptolysin O titer, suggesting streptococcus infection. The patient was successfully treated by pleural drainage in addition to synergistic antimicrobial therapy.
Key Words: Streptococcus pyogenes, newborn, pleural empyema.
Tuberk Toraks 2013; 61(2): 152-154 • doi: 10.5578/tt.5156
Geli? Tarihi/Received: 19.03.2013 - Kabul Edili? Tarihi/Accepted: 03.04.2013
INTRODUCTION
Pleural effusion is defined as fluid accumulation in the pleural space, which exists between the parietal pleura of the chest wall and the visceral pleura of the lung. In neonatal period, implicated pathogens are Staphylococcus aureus, group A streptococcus (GAS, or Streptococcus pyogenes), Bacteroides fragilis, Escherichia coli, Klebsiella species, Pseudomonas aeruginosa and Acinetobacter calcoaceticus (1). GAS is not considered to be a normal inhabitant of the female genital tract and perineum and is rarely cultured from asymptomatic women (2). The reported spectrum of infections with GAS in the newborn includes omphalitis, peritonitis, skin infection, necrotizing fasciitis, toxic shock syndrome, pneumonia, osteomyelitis, septic arthritis, septicemia and meningitis (1).
There are only a few reports on pleural empyema due to GAS in newborn infants (1,3). Therefore, we want to report a case of early onset neonatal pneumonia caused by GAS and complicated with pleural empyema.
Case report
A 72 hour-old boy was admitted to our unit because of respiratory distress and feeding difficulty. The mother had no previous history of premature rupture of membranes. However, fever, pelvic pain, and abnormal vaginal discharge developed two days after delivery and she was given antibiotic treatment with suspect of puerperal sepsis. On admission, the patient was lethargic, cyanotic and tachypneic. Body temperature was 37?C, breath rate 66 per minute, and hearth rate 166 per minute. Intercostal and subcostal retractions were noted. Breath sounds could not be heard on the left lung. Chest X-ray showed shift of the mediastinum to the right, atelectasis and pleural effusion on the left side (Figure 1). Laboratory investigation revealed a hemoglobin of 15.5 g/dL, a hematocrit of 52%, a leukocyte count of 12.900/mm3. Serum C-reactive protein (CRP) level was high (286 mg/L, N: < 10 mg/L). Arterial blood gases revealed the following means: pH 7.18, PaO2: 53 mmHg, PaCO2: 50 mmHg, HCO3: 18.5 mmol/L, with an SaO2 of 78%. In thoracic ultrasonography, air bronchogram, consolidation, pleural thickening, and hyperechoic pleural collection (35 mm) compatible with empyema were observed on the left lung. Ampicillin and cefotaxime were given for empiric treatment. Supplemental oxygen was needed by oxygen hood to keep SaO2 > 90%. After draining the 30 cc of purulent fluid by thoracentesis, a chest tube was inserted and a closed chest drainage system was attached to promote drainage of fluid. Pleural effusion was purulent in character; pH 6.6, undetectable levels of glucose, protein 4.2 g/dL, and LDH: 15.600 IU/L. The analysis of cerebrospinal fluid sample was not compatible with meningitis. GAS was isolated from blood and pleural fluid cultures. Mother's urine and vaginal cultures, which were taken after the third day of antimicrobial treatment, were negative. However, subsequent increase in the antistreptolysin O titer, suggested streptococcus infection.

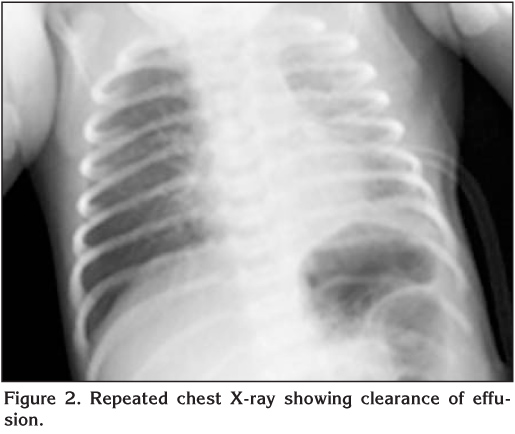
At follow-up, patient's respiratory distress gradually improved. Chest tube was removed on the sixth day of the treatment. Repeated chest X-ray showed that effusion disappeared (Figure 2). However, two days later, the patient's condition deteriorated. He had fever (38.2 ?C) and severe respiratory distress. Laboratory analyses showed leucocytosis (21.500/mm3) with neutrophilia (76%), and increase in serum CRP (138 mg/L). Large left sided pleural effusion was noted on the control chest X-ray. Thoracic ultrasonography showed pleural effusion not exceeding 20 mm in depth. Chest tube was re-placed. Antibiotic treatment was changed to meropenem and clindamycin with suspect of invasive GAS infection. Blood and pleural fluid cultures were taken after the third day of antibiotic revision were negative.? On the 4th day of the chest tube insertion, the patient's condition was well. Both chest X-ray and thoracic ultrasound confirmed decreased pleural effusion on the left lung, so chest tube was removed.? Antibiotic treatment was given for four weeks. The patient was discharged home after full recovery.? By three months of age, his physical and neuro-developmental examination were evaluated as normal.
Discussion
Invasive GAS diseases in neonates are categorized into an early or a late onset group. The major clinical expression of early onset disease is pneumonia or empyema, soft tissue infection, and toxic shock-like syndrome. Common characteristics of early onset disease include respiratory distress, rapid deterioration, and a high mortality rate regardless of the focus of infection. Vertical transmission accounted for the majority (75%) of invasive early onset GAS disease (4). Our patient was diagnosed to be early onset pneumonia caused by GAS and complicated with empyema.
Chest X-ray and ultrasound are helpful both in the diagnosis of pleural effusion and for monitoring the course of parapneumonic effusion. Pleural fluid culture is an important diagnostic tool leading to identification of the bacterial pathogen in 60-80% of cases, in contrast to blood culture, which is positive in 13-31% (5). In our patient, chest X-ray and ultrasound showed the existence or clearance of pleural effusion and guided us in chest drain management. GAS was isolated from blood and pleural fluid culture of the patient.
Chest drain placement is indicated in cases of enlarging effusion or respiratory compromise. If there is fibrin deposition and peel formation, fibrinolysis with urokinase can shorten the hospital stay (6). In the presented case, as chest tube drainage and antibiotic therapy we did perform fibrinolysis or surgical intervention.
Adequate antibiotic concentrations in pleural fluids are obtained during systemic antibiotic therapy. The duration of antibiotic therapy for GAS empyema is controversial: some authors treat with one antibiotic for 7-14 days, while others recommend longer duration and treatment with two antibiotics to obtain a synergistic effect (7,8). A synergistic effect has been described when combining penicillin and aminoglycoside in the treatment of streptococcal infections. Animal models and a retrospective review of treatment of 56 children with invasive GAS infection favor combination treatment with a beta-lactam plus clindamycin (9). In our patient, first line antimicrobial therapy (ampiciline plus cefotaxime) failed. Clinical and radiological improvement could be achieved after antibiotic revision (meropenem and clindamycin).
Mortality in childhood empyema has been reduced to 2.5% (10). However, in neonates, empyema is a potentially fatal condition if not recognized and treated early (3). By this case, we would like to express that GAS may cause pneumonia complicated with pleural empyema in the neonatal period. The mother should be carefully investigated for infection in newborns with severe respiratory distress. Early treatment with synergistic antibiotics and chest tube drainage would be life-saving.
CONFLICT of INTEREST
None declared.
REFERENCES
- Thaarup J, Ellermann-Eriksen S, Stjernholm J. Neonatal pleural empyema with group A streptococcus. Acta Paediatr 1997; 86: 769-71.
- Parson MT. Angel JL. Specific intra-amniotic bacterial infections. In: Pastorek JG (ed). Obstetric and gynecologic infectious disease. New York: Raven Press, 1994: 383-4.
- Gupta R, Faridi MM, Gupta P. Neonatal empyema thoracis. Indian J Pediatr 1996; 63: 704-6.
- Miyairi I, Berlingieri D, Protic J, Belko J. Neonatal invasive group A streptococcal disease: case report and review of the literature.? Pediatr Infect Dis J 2004; 23: 161-5.
- Brook I. Microbiology of empyema in children and adolescents. Pediatrics 1990; 85: 722-6.
- Proesmans M, Boeck KD. Clinical practice: treatment of childhood empyema. Eur J Pediatr 2009; 168: 639-45.
- Freij BJ, Kusmiesz H, Nelson JD, McCracken GH. Parapneumonic effusions and empyema in hospitalized children: a retrospective review of 227 cases. Pediatr Infect Dis 1984; 3: 578-91.
- Nathavitharana KA, Watkinson M. Neonatal pleural empycina caused by group A Streptococcus. Pediatr Infect Dis J 1994: 13: 671-2.
- Stevens DL, Gibbons AE, Bergstrom R, Winn V. The Eagle effect revisited. Efficacy of clindamycin, erytromycin, and penicillin in the treatment of streptococcal myositis. J Infect Dis 1988; 158: 23.
- Padmini R, Srinivasan S, Puri RK, Nalini P. Empyema in infancy and childhood. Ind Pediatr 1990; 27: 447-52.
Yaz??ma Adresi (Address for Correspondence):
Dr. Dilek D?LL?,
Dr. Sami Ulus Kad?n Do?um,
?ocuk Sa?l??? ve Hastal?klar? E?itim ve
Ara?t?rma Hastanesi Yenido?an Klini?i,
ANKARA - TURKEY
e-mail: dilekdilli2@yahoo.com