K???k h?creli d??? akci?er kanseri olan hastalarda
evrelere g?re ya?am kalitesi ve egzersiz kapasitesinin kar??la?t?r?lmas?
Elvan YILMAZ1, Sevgi ?ZALEVL?1, Hasan ERS?Z2, Ay?e YE??N3, Ahmet ?NEN2, Atilla AKKO?LU3
1 Dokuz Eyl?l ?niversitesi Fizik Tedavi ve Rehabilitasyon Y?ksekokulu, ?zmir,
2 Dokuz Eyl?l ?niversitesi T?p Fak?ltesi, G???s Cerrahisi Anabilim Dal?, ?zmir,
3 Dokuz Eyl?l ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, ?zmir.
?ZET
K???k h?creli d??? akci?er kanseri olan hastalarda evrelere g?re ya?am kalitesi ve egzersiz kapasitesinin kar??la?t?r?lmas?
Giri?: ?al??mam?z?n amac?; k???k h?creli d??? akci?er kanseri (KHDAK) hastalar?nda egzersiz kapasitesi ve sa?l?kla ilgili ya?am kalitesi parametrelerini evrelere g?re kar??la?t?rmakt?r.
Materyal ve Metod: Evre I-II (grup erken evre, n= 17) ve evre IIIA-IV olan (grup ileri evre, n= 35) 52 (ba??ms?z y?r?yebilen) KHDAK hastas? ?al??maya dahil edildi. Egzersiz kapasitesi (alt? dakika y?r?me testiyle), periferal kas kuvveti (s?rt ve bacak dinamometresiyle), performans d?zeyi (Karnofsky performans skalas?yla), sa?l?kla ilgili ya?am kalitesi [European Organization for Research and Treatment of Cancer Ya?am Kalitesi Anketi (EORTC QLQ-C30) ve Short Form-36 (SF-36) anketiyle], depresyon ve kayg? d?zeyi (Hastane Anksiyete ve Depresyon skalas?yla) de?erlendirildi.
Bulgular: ?ki grup aras?nda ya?, beden kitle indeksi, solunum semptomlar? ve h?cre tipi da??l?m? a??s?ndan fark bulunmad? (p> 0.05). ?leri evre grupta solunum fonksiyon testi de?erleri, periferal kas kuvveti, y?r?me mesafesi, ya?am kalitesinin ?zellikle fonksiyonel kapasite ve a?r? kategorileri skorlar? erken evre gruba g?re d???kt? (p≤ 0.05). Depresyon ve anksiyete sonu?lar? her iki grupta benzer bulundu (p> 0.05).
Sonu?: ?leri evre KHDAK hastalar?nda egzersiz kapasitesi; azalm?? solunum fonksiyonlar? ve periferal kas kuvveti nedeniyle erken evre KHDAK hastalar?na g?re daha fazla azalmaktad?r. Bu nedenlerle; KHDAK hastalar?nda azalm?? egzersiz kapasitesinin hastalar?n ya?am kalitesinin ?zellikle fonksiyonel kategorilerini olumsuz olarak etkiledi?ini d???nmekteyiz.
Anahtar Kelimeler: K???k h?creli d??? akci?er kanseri, egzersiz kapasitesi, ya?am kalitesi.
SUMMARY
Comparison of health-related quality of life and exercise capacity according to stages in patients with non-small cell lung cancer
Elvan YILMAZ1, Sevgi ?ZALEVL?1, Hasan ERS?Z2, Ay?e YE??N3, Ahmet ?NEN2, Atilla AKKO?LU3
1 Dokuz Eylul University School of Physical Therapy and Rehabilitation, Izmir, Turkey,
2 Department of Chest Surgery, Faculty of Medicine, Dokuz Eylul University, Izmir, Turkey,
3 Department of Chest Disease, Faculty of Medicine, Dokuz Eylul University, Izmir, Turkey.
Introduction: The aim of this study is to compare the exercise capacity and health-related quality of life parameters according to stages of patients with non-small cell lung cancer (NSCLC).
Materials and Methods: Fifty-two patients (who are able to ambulate independently) with stage I-II (group early-stage, n= 17) and stage IIIA-IV NSCLC (group advanced-stage, n= 35) were included. Exercise capacity (six minute walking test), strength of the peripheral muscle (Back and Leg Dynamometer), performance status (Karnofsky performance status scale), health-related quality of life- HRQOL (European Organization for Research and Treatment of Cancer Quality of life measure and Short Form-36 Health Survey), depression and anxiety (Hospital Anxiety and Depression Scale) were evaluated.
Results: No difference was found in age, body mass index, respiratory symptoms and the distribution of disease cell types between two groups (p> 0.05). In advanced-stage group, pulmonary function test values, peripheral muscle strength, walking distance and health-related quality of life scores especially the categories of functional capacity and pain were established significantly lower compared to early-stage group (p≤ 0.05). Depression and anxiety levels were confirmed to be similar between groups (p> 0.05).
Conclusion: The exercise capacity of patients with advanced-stage NSCLC is lower due to reduced pulmonary functions and peripheral muscle strength compared to patients with early-stage NSCLC. Therefore, we can conclude that reduced exercise capacity negatively impacts functional categories of health related quality of life of patients with advanced-stage NSCLC.
Key Words: Non-small cell lung cancer, exercise capacity, health-related quality of life.
Tuberk Toraks 2013; 61(2): 131-139 • doi:10.5578/tt.5396
Geli? Tarihi/Received: 25/01/2013 - Kabul Edili? Tarihi/Accepted: 13/05/2013
* Bu ?al??ma, 14. D?nya Akci?er Kanseri Kongresi (3-7 Temmuz 2011, Amsterdam, Hollanda)'nde poster olarak sunulmu?tur.
** This study was presented as a poster in 14th World Conference on Lung Cancer July 3-7 2011, Amsterdam, The Netherlands.
Introduction
Recently, lung cancer is one of the most serious diseases known as the second cause of death after cardiovascular disease in the world (1). Non-small cell lung cancer (NSCLC) comprises approximately 85% of the total lung cancers (2). Surgery, chemotherapy and/or radiotherapy are planned for treatment of NSCIC according to stages (3). Associated with disease and/or the treatments in lung cancer survivors, serious side effects occur and changes in their functional capacity and health related quality of life (HRQL) appear (4). Most of the lung cancer patients complain about symptoms which restrict their daily living activities such as dyspnea, fatigue, pain, cough, loss of appetite, and weight loss. In addition to these symptoms, stage of lung cancer, cell type, severity of disease and treatment side effects have destructive effects on the patients' exercise capacity and quality of life (5). From all reasons above, the success of medical treatment and pulmonary rehabilitation programmes also diminishes. Therefore, assessment of HRQL and exercise capacity is important to plan cancer therapy and follow patients with NSCLC during and after the treatment. Based on the aforementioned reasons, the aim of our study was to compare exercise capacity and HRQL parameters according to stages less than and equal to 2 (early-stage) and greater than 2 (advanced-stage) in patients with NSCLC and to discuss the results with clinical characteristics of patients.
MATERIALS and Methods
Setting and Participants
Between December 2010-November 2011, 52 patients diagnosed with NSCLC at a University Hospital, were included in this study. The inclusion criteria of patients were as follows: pathologically diagnosed NSCLC; being able to mobilize independently; not having assistive equipment for mobilization; not having cognitive impairment and accepting to participate in the study. The exclusion criteria of patients were as follows: chronic obstructive pulmonary disease exacerbation, pneumonia and other lung infections, uncontrolled hypertension and cardiac diseases, a neurological disease, severe mental or cognitive impairment and hearing problems.
The protocol of the study accepted by Clinical and Laboratory Researches Ethics Committee of our University and signed consents obtained from all patients of the study.
Outcome Measurements
The demographic and clinical characteristics of the patients were recorded. Pain (visual analog scale), pulmonary function (spirometry), exercise capacity [six minute walking test (6MWT)], severity of dyspnea and effect of daily activity on dyspnea (Medical Research Council Scale), performance status (Karnofsky Performance Status scale), HRQL (European Organization for Research and Treatment of Cancer Quality of life measure and Short Form-36 Health Survey), depression & anxiety (Hospital Anxiety and Depression Scale), strength of the back and leg muscles (with Back and Leg Dynamometer) and the quadriceps femoris (with manual muscle test) evaluated.
Pain severity evaluated using Visual Analog Scale (VAS), that uses a 100 mm long bar (0: no pain, 100: very severe pain). The patients pointed on the bar, which demonstrates the severity of the feeled pain. Between the starting point of the bar and the marked point measured and recorded as scoring (6).
The pulmonary function was evaluated by spirometry Sensor Medics Vmax 22 machine (SensorMedics Inc., Anaheim, CA, USA) appropriately based on the American Thoracic Society criteria's. Forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC ratio and their percentages according to the predicted values recorded (7).
6MWT is a simple, reliable and cost-effective measure to assess functional status. The test was performed according to the American Thoracic Society criteria in 30-meter corridor of hospital. Before and after the 6MWT; peripheral oxygen saturation, heart rate, severity of dyspnea and leg fatigue assessed. The severities of dyspnea and leg fatigue were recorded using the Modified Borg Scale (MBS). It is a 10 point scale with a non-linear scaling system using descriptive terms to receive the responses from the participants. The peripheral oxygen saturation (SpO2) and heart rate were recorded at a sitting position using the Pulse Oximeter (Model: MD 300 2x 1.5V AAA) (8,9).
Modified Medical Research Council Scale (MMRCS) is based on a variety of physical activities leading to dyspnea. The scale consists of five items. The patients indicate the best expression which demonstrates respiratory distress. The items are scored from 0 (no respiratory distress) to 4 (maximum respiratory distress) (10).
Karnofsky Performance Status scale (KPS) is used to assess functional capacity. KPS numerically describes ?the patient's ability to carry on his normal activity and work, or his need for a certain amount of custodial care, or his dependence on constant medical care?. Each ten-point increase on the 0-100 point scale describes performance status (100: normal, no complaints) (11).
European Organization for Research and Treatment of Cancer Quality of Life measure (EORTC QLQ-C30) version 3.0 is a 30-item questionnaire that measures cancer-specific quality of life in cancer patients. This self-administered questionnaire includes five functional scales [physical (PF), role (RF), cognitive (CF), emotional (EF) and social (SF) functioning scales] and three symptom scales (fatigue, pain and nausea/vomiting), a general health/quality of life scale, and several single items of additional symptoms commonly described by cancer patients (e.g. dyspnea, appetite loss, sleep disturbance, constipation and diarrhea), in addition to the cost-effect of the disease and treatment. Questionnaire scores calculated according to EORTC QLQ-C30 scoring system. The scores for each category were between 0 and 100. High scores indicate better health status, higher quality of life and decreased symptoms in functional, general health/quality of life and symptom scales (12). The validity and reliability of this survey for Turkish patients was ensured by Cankurtaran et al. (13).
Short Form-36 Health Survey (SF-36) was used to assess general health-related quality of life. This survey includes 36 questions in eight multi-item categories (physical functioning, role functioning-physical, role functioning-emotional, pain, vitality, social functioning, mental health and general health perception). Each category is scored from 0 to 100. Higher scores indicating better health related quality of life (14). The validity and reliability of SF-36 Health Survey for Turkish patients was completed (15).
Hospital Anxiety and Depression Scale (HADS) is one of the most commonly used questionnaires for evaulating clinically significant anxiety and depression in patients with physical disease. This self-administered scale includes seven items at two categories as evaluating anxiety (HADS-A) and assessing depression (HADS-D). Single numbers shows anxiety and double numbers shows depression. The items are scored from 0 (no distress) to 3 (maximum distress). Total score varies between 0 and 21 for each category. The validity and reliability of HADS in Turkish language was ensured by Aydemir et al. (16).
The peripheral muscle strength was examinated with evaluating strength of the back, leg and quadriceps femoris muscles. Extensor quadriceps femoris muscle strength was assessed with manual muscle test by the use of Daniels 0-5 Grading System. At sitting position, patients extend knee through range of motion. Physiotherapist resist above ankle joint (17). In addition, Back/leg dynamometer (TKK 5402 leg-D, TAKEI Scientific Instruments Lo, Ltd., Japan) was used to measure leg and back muscle strength. Leg muscle strength was recorded at standing position while both knees were flexed at an angle of 135?. They extend their knees for back muscle strength. The patients held a handle bar which was placed on the thigh level. Chain length was adjusted according to the above position. Using pronated grips, patients were asked to slowly straighten their legs up to their maximal level without using back or shoulder muscles for leg muscles strenght. And in the same position, patients were asked to pull of chain only with use to their back in knee extension position for back muscle strength evaluation. Every subject received consistent encouragement until the experimenters read no further changes on the scale. The test was performed for 3 times with 1-min rest intervals; the highest value was selected and recorded (18,19).
Statistical Analysis
The statistical analysis of obtained data was performed using SPSS 15.0 software package. Data are reported as mean ? standard deviation (mean ? SD) and percentages (%). Mann-Whitney U test and chi-square test were used in the determination of groups' outcome parameters differences. A p value < 0.05 was considered statistically significant.
Results
No difference was found in age, body mass index, smoking history and disease cell types between early-stage and advanced-stage groups (p> 0.05). The distribution of symptoms were similar in both groups except fatigue and pain history (p> 0.05). The demographic and clinical characteristics of the patients were presented in Table 1.

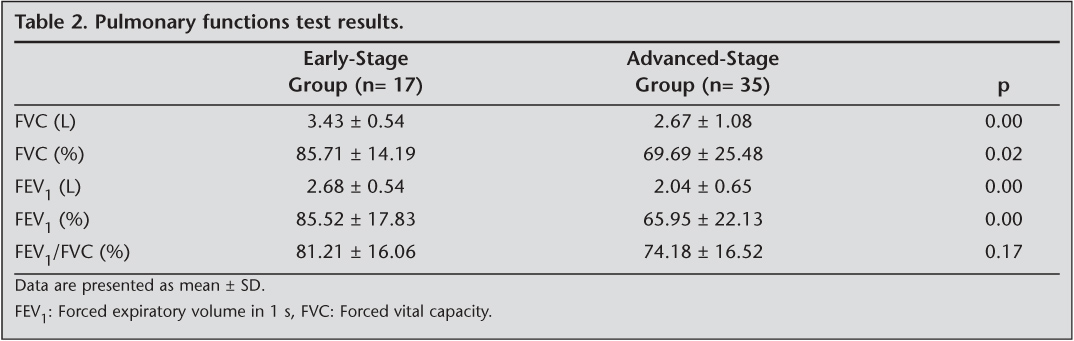
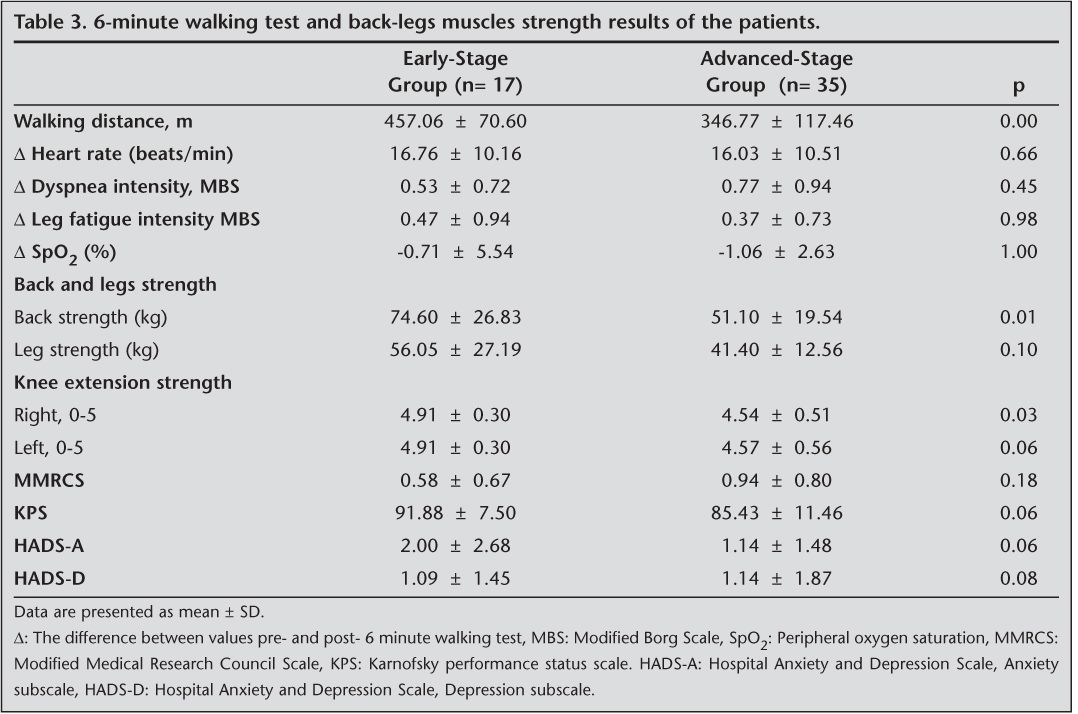
In advanced-stage group, pulmonary function test results and peripheral muscle strength were statistically and significantly lower compared to early-stage group (p≤ 0.05, Table 2). The mean walking distance was found 457.06 ? 70.60 m in early-stage group patients and 346.77 ? 117.46 m in advanced-stage group patients (Table 3). MMRCS results showed that the effect of dyspnea during activities of daily living was lower in early-stage group patients compared to advanced-stage group patients (p= 0.18). KPS scores were 91.88 ? 7.50 in group 1 and 85.43 ? 11.46 in group 2 (p= 0.06). In advanced-stage group patients, depression and anxiety levels were higher than early-stage group patients (p> 0.05, Table 3).
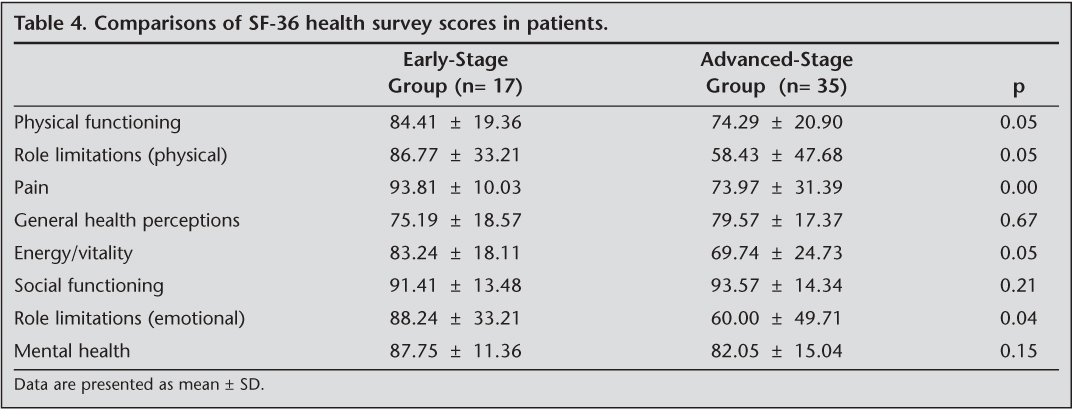
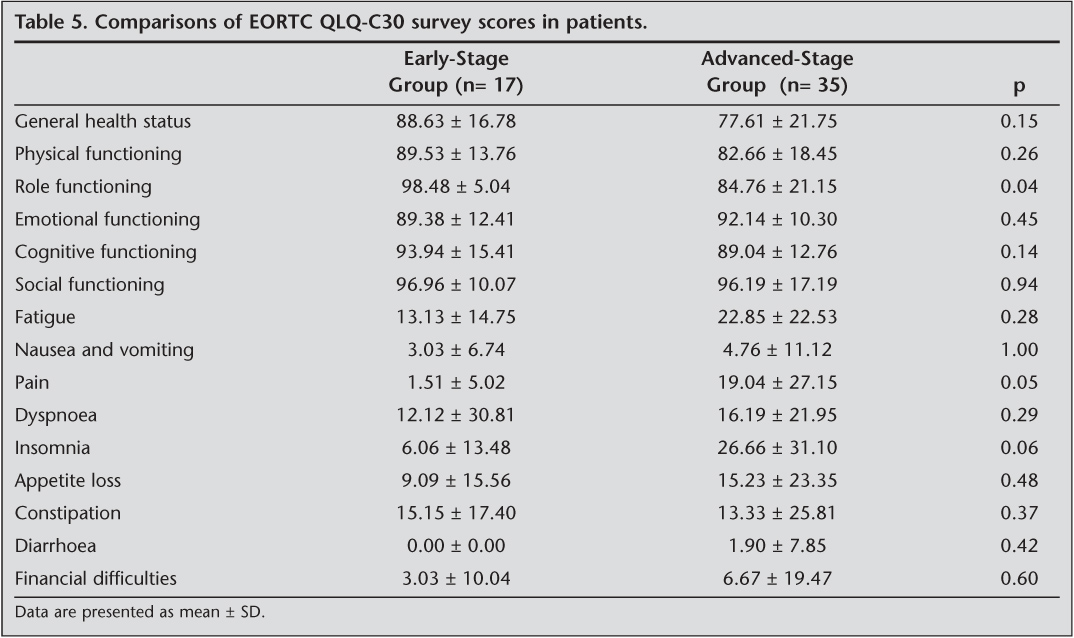
SF-36 Health Survey scores especially the categories of functional physical functioning, role functioning-physical, role functioning-emotional, bodily pain and vitality were significantly lower in advanced-stage group patients (p≤ 0.05). Scores of role functioning category of EORTC QLQ-C30 survey were significantly lower and pain categories scores were significantly greater in advanced-stage group (p≤ 0.05, Table 4,5).
Discussion
Our study results showed that exercise capacity and peripheral muscle strength were lower and health related quality of life categories especially functional categories were more affected in advanced-stage NSCLC patients compared to early-stages NSCLC patients.
Lung cancer patients have symptoms as breathlessness, cough, bronchial secretion, loss of appetite, pain and fatigue that restrict their daily life activities. The exercise capacity and quality of life are affected negatively related to the symptoms, lung cancer stage, cell type and treatment modalities such as chemotherapy and/or radiotherapy applications (20,21,22). The current literature indicates that the most common symptoms are breathlessness and cough (90%) and pain (80%) (23). In our study, while the most complained sytmptoms in early-stage patients were cough and breathlessness, in advanced-stage patients, cough, bronchial secretion and fatigue were defined as the most complained sytmptoms.Thus, we considered that the decrease in exercise capacity and quality of life in advanced-stage patients might be associated with the increase in the breathlessness, cough, secretion and fatigue symptoms.
Machado et al., investigated the effect of chemotherapy on the physical condition of stage IIIB and IV NSCLC with 6MWD. They found that chemotherapy had a beneficial effect on the exercise capacity of the patients (24). In our study walking distance in patients with advanced-stage lung cancer was lower than in patients with early-stage treated chemotherapy and/or radiotherapy. We think that the decrease in exercise capacity of advanced-stages patients might be associated with medical therapy, severe clinical course of disease, symptom burden, lower peripheral muscle strength and respiratory functions.
Medical therapies in lung cancer and other associated diseases adversely affect heart, pulmonary functions and oxygen circulation to deliver oxygen to skeletal muscles for adenosine triphosphate synthesis to drive muscular contraction, which reduces exercise capacity (25). In our study only ambulatory patients were evaulated and knee extensor muscle strength and back extensor muscle strength were found statistically significantly higher in early-stage patients. The advanced-stage patients' peripheral muscle strength was lower due to negatively affected pulmonary functions and reduced physical function.
Braun et al., found that general quality of life and physical function categories of EORTC-QLQ-C30 provide useful prognostic information in non-small cell lung cancer patients (26). We assessed EORTC-QLQ-C30 for all ambulatory NSCLC patients treated or not treated and compared according to stages. Results of EORTC-QLQ-C30 in advanced-stage NSCLC patients showed that the only role function and pain were significantly lower than early-stage NSCLC patients. We considered that the other categories were similar because our patients of NSCLC still have an active lifestyle and could ambulate independently.
Lee LJ et al., compared the HRQOL between patients with NSCLC and healthy controls with World Health Organization's Quality of Life instruments they found that more advanced-stages of NSCLC patients had poorer scores than did the healthy controls in the physical and psychological domains, also patients with IIIB-IV stages had lower quality of life than patients with I-IIIA stages (27). In our study, HRQOL of patients with NSCLC was assessed using SF-36 Health Survey and EORTC QLQ-C30. Physical function of quality of life was lower in stage IIIA-IV patients depending on lower muscle strength and exercise capacity. Impaired pulmonary functions, increased pain severity and decreased peripheral muscle strength of these patients might be caused by reduction of physical functions. In a study there was some improvement in some symptoms as hemoptysis, chest pain, arm/shoulder pain, and appetite loss; but breathlessness, cough, and fatigue were increased in NSCLC patients before radiotherapy and after the completion of radiotherapy. Health-related quality of life scores especially the categories of physical and role functioning and general health perceptions were established significantly lower after radiotherapy (28). In our study in early-stage patients who received radiotherapy alone had a high percentage so that their physical and role functioning and general health perceptions might be affected after radiotherapy.
We also think that the increase in anxiety and depression might be associated with HRQOL impairments and reduced physical function (29,30,31). Physical functions of patients with stage IA and IB NSCLC are affected moderately and pulmonary rehabilitation programs may be beneficial in management of distressed mood and improvement of physical functions (32). We found that scores of physical functions, general health perceptions and vitality categories of patients with stage I-IIB NSCLC were decreased. In addition, breathlessness and cough are the most complained symptoms in these patients and affect peripheral muscle strength, exercise capacity and quality of life.
There was reduction in all categories of EORTC QLQ-C30 and EORTC QLQ-LC13 especially vitality and physical function, compared before and after diagnosis of stage I-III NSCLC patients because of negative effects of medical therapy such as chemotherapy and radiotherapy in these patients (33). We also think that reduced exercise capacity and peripheral muscle strength are decreased in physical function categories of quality of life.
General health status and physical functions most affected HRQOL of NSCLC patients, also number and severity of symptoms, performance status, severity of dyspnea and pulmonary function tests results significantly affected HRQOL (34). In our study, the majority of EORTC QLQ-C30 and SF-36 Health Survey results were associated with KPS results in patients with advanced-stage NSCLC, but the clinics of patients with early-stage NSCLC were not supported by KPS. Thus, we considered that the decrease in exercise capacity and quality of life in our patients with advanced-stage might be associated with severe clinical course and decreased performance status.
In the current literature there were not so many studies about exercise capacity and HRQOL of lung cancer especially according to cell type and stages. We investigate the comparison of exercise capacity and health-related quality of life according to stages in patients with NSCLC who are able to ambulate and don't have a lung operation history. The most important limitations of our study were the small number of patients especially early-stage patients and participation of only male patients. In addition, we did not measure exercise capacity with cardiopulmonary test and quadriceps femoris extensor muscle strength with dynamometer. For this reason, further studies, including larger sample size and both of male and female patients and also objective exercise tests are needed to confirm these results.
The results of this study conclude that exercise capacity is decreased due to lower peripheral muscle strength and pulmonary functions and increased dyspnea severity and anxiety and depression levels in patients with advanced-stage (stages III-IV) NSCLC and hence HRQOL of these patients is impaired much more in relation to reduced exercise capacity compared to patients with early-stage (stages I-II) NSCLC. Although the number of patients was insufficient, the results are concluded that exercise capacity and HRQOL assessments for lung cancer patients should be assessed systematically and it is important that results should be considered according to stages and should be taken into consideration for following medical treatment protocol and pulmonary rehabilitation programme of these patients.
Acknowledgement
The authors are grateful to all patients who participated in this study and all physicians for referring to patients at the department of chest disease and thoracic surgery and paramedics Bar?s Ufuk Yucel for pulmonary function tests.
CONFLICT of INTEREST
None declared.
REFERENCES
- Ozturk A, Sarihan S, Ercan I, Karadag M. Evaluating quality of life and pulmonary function of long-term survivors of non-small cell lung cancer treated with radical or postoperative radiotherapy. Am J Clin Oncol 2009; 32: 65-72.
- Langer CJ, Besse B, Gualberto A, Brambilla E, Soria JC. The evolving role of histology in the management of advanced non-small cell lung cancer. J Clin Oncol 2010; 28: 5311-20.
- Yang P. Epidemiology of lung cancer prognosis: quantity and quality of life. Methods Mol Biol 2009; 471: 469-86.
- Akin S, Can G, Aydiner A, Ozdilli K, Durna Z. Quality of life, symptom experience and distress of lung cancer patients undergoing chemotherapy. Eur J Oncol Nurs 2010; 14: 400-9.
- Ozalevli S, Ilgin D, Karaali HK, Bulac S, Akkoclu A. The effect of in-patient chest physiotherapy in lung cancer patients. Support Care Cancer 2010; 18: 351-8.
- Price D, McGrath PA, Rafii A, Buckinham B. The validation of visual analogue scale as ratio scale measure for chronic and experimental pain. Pain 1983; 17: 45-56.
- American Thoracic Society: Standardization of spirometry, 1994 update. Am J Respir Crit Care Med 1995; 152: 1107-36.
- American Thoracic Society: ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002; 166: 111-7.
- Borg G. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982; 14: 377-81.
- Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Modified Medical Research Council (MMRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999; 54: 581-6.
- Karnofsky DA, Burchenal JH. The clinical evaluation of chemotherapeutic agents in cancer. In: MacLeod CM (ed). Evaluation of Chemotherapeutic Agents. New York: Columbia University Press, 1949: 191-205.
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993; 85: 365-76.
- Cankurtaran ES, Ozalp E, Soygur H, Ozer S, Akbiyik DI, Bottomley A. Understanding the reliability and validity of the EORTC QLQ-C30 in Turkish cancer patients. Eur J Cancer Care 2008; 17: 98-104.
- Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ 1992; 305: 160-4.
- Demiral Y, Ergor G, Unal B, Semin S , Akvardar Y, Kivircik B, et al. Normative data and discriminative properties of short form 36 (SF-36) in Turkish urban population. BMC Public Health 2006; 6: 247.
- Aydemir ?, G?venir T, K?ey L, K?lt?r S. The reliability and validity of Turkish form of Hospital Anxiety and Depression Scale. Journal of Turkish Psychiatry 1997; 8: 280-7.
- Clarkson HM, Giilewich GB. Musculoskeletal Assessment, Joint Range of Motion and Manual Muscle strength. Baltimore: Williams and Wilkins, 1989: 58-62.
- Coldwells A, Atkinson G, Reilly T. Sources of variation in back and leg dynamometry. Ergonomics 1994; 73: 79?86.
- Heyward V. Advanced Fitness Assessment Exercise Prescription. 3rd ed. Champaign: Human Kinetics, 1998.
- Benzo RP. Pulmonary rehabilitation in lung cancer: ascientific opportunity. J Cardiopulm Rehabil Prev 2007; 27: 61-4.
- Brown DJ, McMillan DC, Milroy R. The correlation between fatigue, physical function, the systemic inflammatory response, and psychological distress in patients with advanced lung cancer. Cancer 2005; 103: 377-82.
- Tanaka K, Akechi T, Okuyama T, Nishiwaki Y, Uchitomi Y. Impact of dyspnea, pain, and fatigue on daily life activities in ambulatory patients with advanced lung cancer. J Pain Symptom Manage 2002; 23: 417-23.
- Adamsen L, Stage M, Laursen J, Rorth M, Quist M. Exercise and relaxation intervention for patients with advanced lung cancer: a qualitative feasibility study. Scand J Med Sci Sports 2012; 22: 804-15.
- Machado L, Saad IA, Honma HN, Morcillo AM, Zambon L. Evolution of performance status, body mass index and six-minute walk distance in advanced lung cancer patients undergoing chemotherapy. J Bras Pneumol 2010; 36: 588-94.
- Jones LW, Eves ND, Peterson BL, Garst J,Crawford J, West MJ, et al. Safety and feasibility of aerobic training on cardiopulmonary function and quality of life in postsurgical nonsmall cell lung cancer patients: a pilot study. Cancer 2008; 113: 3430-9.
- Braun DP, Gupta D, Staren ED. Quality of life assessment as a predictor of survival in non-small cell lung cancer. BMC Cancer 2011; 11: 353.
- Lee LJ, Chung CW, Chang YY, Lee YC, Yang CH, Liou SH, et al. Comparison of the quality of life between patients with non-small cell lung cancer and healthy controls. Qual Life Res 2011; 20: 415-23.
- Langendijk JA, Aaronson NK, de Jong JM, ten Velde GP Muller MJ, Lamers RJ, Slotman BJ, et al. Prospective study on quality of life before and after radical radiotherapy in non-small cell lung cancer. J Clin Oncol 2001; 19: 2123-33.
- Carlsen K, Jensen AB, Jacobsen E, Krasnik M, Johansen C. Psychosocial aspects of lung cancer. Lung Cancer 2005; 47: 293-300.
- Smith EL, Hann DM, Ahles TA, Furstenberg CT, Mitchell TA, Meyer L, et al. Dyspnea, anxiety, body consciousness, and quality of life in patients with lung cancer. J Pain Symptom Manage 2001; 21: 323-9.
- Buchanan D, Milroy R, Baker L, Thompson AM, Levack PA. Perceptions of anxiety in lung cancer patients and their support network. Support Care Cancer 2010; 18: 29-36.
- Ostroff JS, Krebs P, Coups EJ, Burkhalter JE, Feinstein MB, Steingart RM, et al. Health-related quality of life among early-stage, non-small cell, lung cancer survivors. Lung Cancer 2011; 71: 103-8.
- Montazeri A, Milroy R, Hole D, McEwen J, Gillis CR. How quality of life data contribute to our understanding of cancer patients' experiences? A study of patients with lung cancer. Qual Life Res 2003; 12: 157-66.
- Mohan A, Singh P, Singh S, Goyal A, Pathak A, Mohan C, et al. Quality of life in lung cancer patients: impact of baseline clinical profile and respiratory status. Eur J Cancer Care 2007; 16: 268-76.
Yaz??ma Adresi (Address for Correspondence):
Dr. Sevgi ?ZALEVL?,
Dokuz Eyl?l Universitesi Fizik Tedavi ve
Rehabilitasyon Y?ksekokulu,
35340, ?nciralt? ?ZM?R - TURKEY
e-mail: sevgi.ozalevli@gmail.com