Asemptomatik gen? hastada bulunan mediastinal insidental nadir kitle: Timolipoma
Nesrin U?RA?1, Elif ?lker AKYILDIZ1, Nermin ?NAL1, Ahmet Sami BAYRAM2
1 Uluda? ?niversitesi T?p Fak?ltesi, Patoloji Anabilim Dal?, Bursa,
2 Uluda? ?niversitesi T?p Fak?ltesi, G???s Cerrahisi Anabilim Dal?, Bursa.
Tuberk Toraks 2013; 61(1): 78-80 • doi: 10.5578/tt.4724
Geli? Tarihi/Received: 10/01/2013 - Kabul Edili? Tarihi/Accepted: 31/01/2013
Dear Editor,
Thymolipoma, is an anterior mediastinal relatively uncommon benign tumor that consists of thymic and fatty tissue which is surrounded by a capsule. Lange, in 1916 first described a case with thymolipoma (1). Moreover, the term "thymolipoma" was first used by Hall in 1949 (2). Although thymolipoma can occur at any age, 80% of the tumors occur during the 4th decade of life. There appears to be no gender-related difference in the incidence (3). Herein, we present a 22 year-old female who had asymptomatic mediastinal mass. Histologic features in this patient were consistent with thymolipoma.
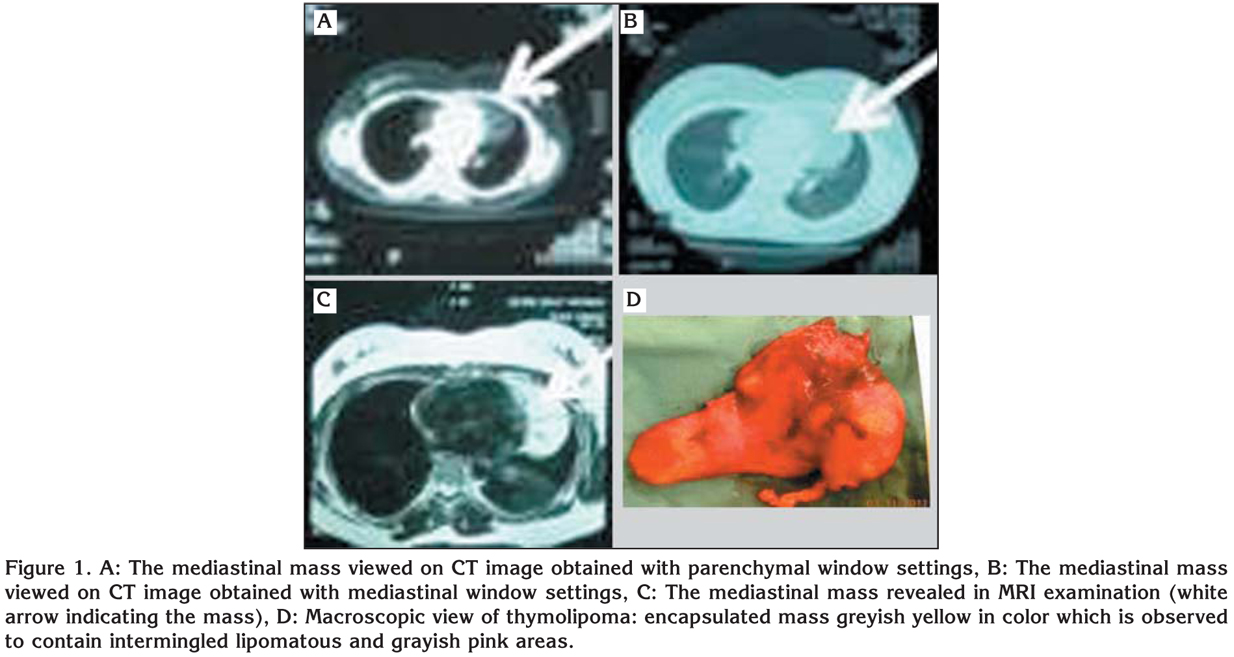
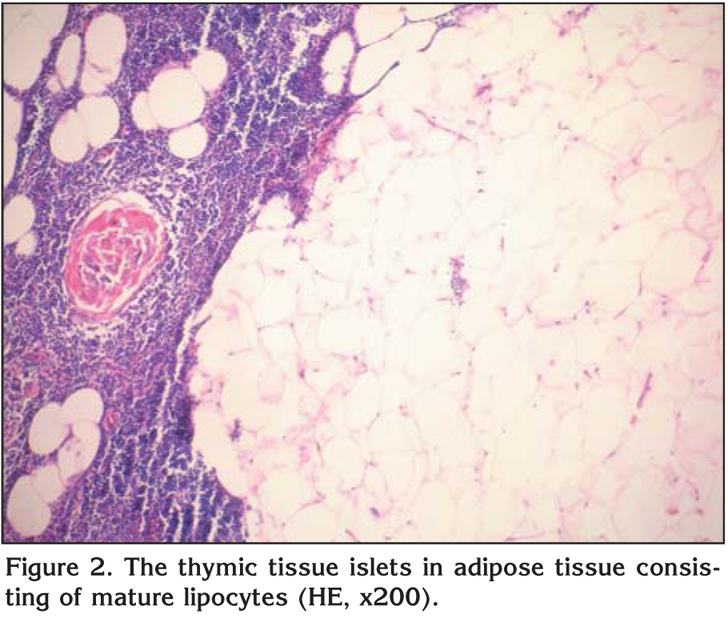
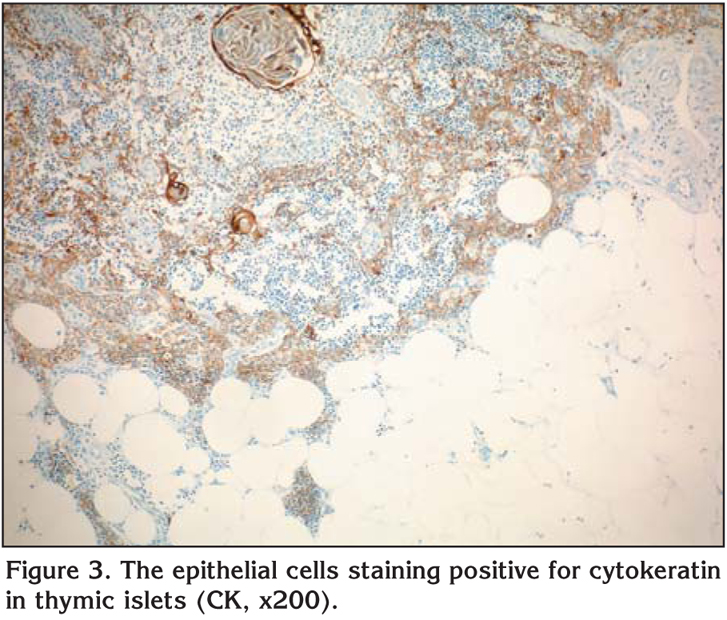
A twenty-year-old healty female was admitted with a mediastinal enlargement detected by routine radiological examination in general health screening performed in school. The patient had no symptom and her physical examination findings, laboratory tests were normal. Computed tomographic (CT) scan (Figure 1A,B) and magnetic resonance imaging (MRI) (Figure 1C) showed a lobulated, well-defined mass in anterior mediastinum. The mass was removed en bloc though a left submamarian anterior thoracotomy. Macroscopically, the resected specimen was encapsulated, grayish yellow in color, 15 x 12 x 3.5 cm in size, and 292 g in weight (Figure 1D). Macroscopic sections revealed intermingled grayish pink areas and yellow lipomatous areas. In microscopic examination, thymic tissue islets were detected within the adipose tissue. While the adipose tissue predominated in some areas, the thymic tissue was in the foreground in some others. The thymic islets were detected to contain epithelial cells, lymphocytes and Hassal's corpuscles some of which were cystically dilated (Figure 2). The immunohistochemical study revealed epithelial cells staining positive for cytokeratin (Figure 3) and lymphocytes staining positive for leucocyte common antigen (LCA). By these histopathological and immunohistochemical results, the case was diagnosed as thymolipoma. No complication occurred in the postoperative period. The patient was discharged from the hospital on the 3rd postoperative day. One year after the operation, a follow-up chest CT evaluation showed no specific complication or recurrence.
Thymolipomas are benign tumors constituting 2-9% of all thymic neoplasms. Fewer than 100 cases have been described in the literature. Small thymolipomas are generally asymptomatic and identified incidentally; those with greater dimensions, on the other hand, may give rise to respiratory and circulatory problems (4). Our patient was asymptomatic; moreover, the lesion had been detected incidentally during a general health screening performed in school. The pathogenesis of thymolipoma is still controversial, and distinct opinions have been put forth in this regard. One of those opinions advocates that thymolipomas develop as a result of replacement of thymic tissue with mature adipose tissue. While it is suggested by some authors that this tumor is a lipoma containing thymic adipose tissue and involuting thymic glands, another opinion proposes that it is a true thymic hyperplasia accompanied by fat involution. Moreover, there also appears to be some other ideas advocating that thymolipomas are mixed tumors of both mesenchymal and endodermal origin, or that thymomas occur as a result of adipose involution (5). Nevertheless, the exact pathogenesis underlying thymolipoma has still yet to be elucidated.
Thymomas are likely to accompany a number of diseases, such as myastenia gravis, aplastic anemia, hypogammaglobulinemia, lichen planus, Graves' disease. Rieker et al. reported nine thymolipoma cases accompanied by myastenia gravis. The cases with thymolipoma accompanied by myastenia gravis were reported to be at older age, and to have greater tumor size (6). Thymolipoma is depicted on plain chest X-ray, CT and MRI as an anterior mediastinal mass lesion of different densities depending on the adipose and thymic tissue contents. Radiological differential diagnosis should include many other lesions; mediastinal teratoma, lipoma, liposarcoma, thymic hyperplasia, cardiomegaly, thymic cyst and omental herniation can be mentioned among these (7). Not possible to be established in radiological evaluation, the definitive diagnosis requires pathological examination of the mass following its excision.
Thymolipomas are encapsulated, soft in consistency and yellow-colored masses which may be of varying sizes macroscopically. Microscopic evaluation reveals broad mature adipose tissue areas in conjunction with thymic tissues islets of varying amounts. Calcification and cystic degeneration are evident in Hassal's corpuscles in a majority of the cases (4,8). It should be differentiated histopathologically from lipoma, well-differentiated liposarcoma and thymic hyperplasia. Presence of thymic islets within the adipose tissue helps to differentiate thymolipoma from lipoma. Liposarcoma is characterized by nuclear atypia and lipoblasts, whereas thymic tissue islet is not an expected observation. As for thymic hyperplasia, the adipose tissue is not observed as extensively as that in thymolipoma (4,8).
In conclusion, if an anterior mediastinal mass is found, thymolipoma of the thymus should be considered during differential diagnosis. In the clinical management of thymolipoma of the thymus and recurrence isn't common.
CONFLICT of INTEREST
None declared.
REFERENCES
- Lange L. ?ber ein Lipom des Thymus. Zentralbl. Allg Pathol 1916; 27: 97.
- Hall GF. A case of thymolipoma with observations on a possible relationship to intrathoracic lipomata. Br J Surg 1949; 36: 321-4.
- Moran CA, Rosado-de Christenson M, Suster S. Thymolipoma: Clinicopathologic review of 33 cases. Mod Pathol 1995; 8: 741-4.
- Ringe B, Dragojevic D, Frank G, Borst HG. Thymolipoma, a rare, benign tumor of the thymus gland, two case reports and review of the literature. Thorac Cardiovasc Surg 1979; 27: 369-74.
- Toyama T, Mizuno T, Masaoka A, Shibata K, Yamakawa Y, Niwa H, et al. Pathogenesis of thymolipoma: report of three cases. Surg Today 1995; 25: 86-8.
- Rieker RJ, Schirmacher P, Schnabel PA, Moser K, Hoffmann H, Dienemann H, et al. Thymolipoma: a report of nine cases, with emphasis on its association with myastenia gravis. Surg Today 2010; 40: 132-6.
- Rosado-de-Christenson ML, Pugatch RD, Moran CA, Galobardes J. Thymolipoma: analysis of 27 cases. Radiology 1995; 194: 913-4.
- Pai RK, Irvine R. Pathologic quiz case: giant mediastinal mass in a 69-year-old man. Arch Pathol Med 2004; 128: 159-60.
Yaz??ma Adresi (Address for Correspondence):
Dr. Elif ?lker AKYILDIZ,
Uluda? ?niversitesi T?p Fak?ltesi,
Patoloji Anabilim Dal?, G?r?kle,
BURSA - TURKEY
e-mail: nesrin_ugras@yahoo.com