Akut apandisitte bakteriyel translokasyona ba?l? torasik ampiyem
Arif Osman TOKAT1, Sezgin KARASU1, Aziz Mutlu BARLAS2, Yusuf Akif AKG?N2
1 SB Ankara E?itim ve Ara?t?rma Hastanesi, G???s Cerrahisi Klini?i, Ankara,
2 SB Ankara E?itim ve Ara?t?rma Hastanesi, 2. Genel Cerrahi Klini?i, Ankara.
?ZET
Akut apandisitte bakteriyel translokasyona ba?l? torasik ampiyem
Apandisit ve torasik ampiyeme birlikte seyrek rastlan?r. Burada nonperfore apandisit nedeniyle opere edilen bir hastada, bakteriyel translokasyona ba?l? geli?en torasik ampiyem sunulmaktad?r. Hastada ampiyem, klinik ve radyolojik olarak postoperatif ???nc? g?n saptand?. T?p torakostomi ve antibiyotik tedavisi uyguland?. T?m bu tedaviye ra?men, semptomlar ilerledi ve abdominal ultrasonografide kar?n i?inde multilok?ler apse odalar? geli?ti?i saptand?. Kar?n i?indeki apseler nonvask?ler giri?imsel radyolojik tekniklerle bo?alt?ld?. ?nan?yoruz ki, bu olguda torasik ampiyem ve kar?nda multipl apse geli?iminin e? zamanl? olmas?n?n nedeni bakteriyel translokasyondur.
Anahtar Kelimeler: Apandisit, torasik ampiyem, bakteriyel translokasyon.
SUMMARY
Thoracic empyema due to bacterial translocation in acute appendicitis
Arif Osman TOKAT1, Sezgin KARASU1, Aziz Mutlu BARLAS2, Yusuf Akif AKG?N2
1 Clinic of Chest Surgery, Ankara Training and Research Hospital, Ankara, Turkey,
2 Clinic of 2nd General Surgery, Ankara Training and Research Hospital, Ankara, Turkey.
Appendicitis and thoracic empyema are rarely presented together. Herein, we present a thoracic empyema due to bacterial translocation in a patient, after she underwent appendicectomy for nonperforated acute appendicitis. Postoperative third day, thoracic empyema was revealed clinically and radiologically. Tube thoracostomy and antibiotherapy were performed. Despite all these therapy, her symptoms went on, and abdominal ultrasonography revealed multilocular collections and formations of abscess in the abdomen. All abscesses were drained by nonvascular interventional radiologic methods. We believe that simultaneous occurence of thoracic empyema and formations of abscess were occured due to bacterial translocation.
Key Words: Appendicitis, thoracic empyema, bacterial translocation.
Tuberk Toraks 2013; 61(1): 54-56 • doi: 10.5578/tt.2449
Geli? Tarihi/Received: 27/11/2012 - Kabul Edili? Tarihi/Accepted: 25/02/2013
INTRODUCTION
Appendicitis and thoracic empyema are common conditions, but they are rarely associated with each other. A few number of cases have previously been reported (1,2). In this case report, simultaneous occurrence of thoracic empyema due to bacterial translocation of Enterococcus avium and Escherichia coli was presented in a non-immunocompromised patient who had acute appendicitis.
Case report
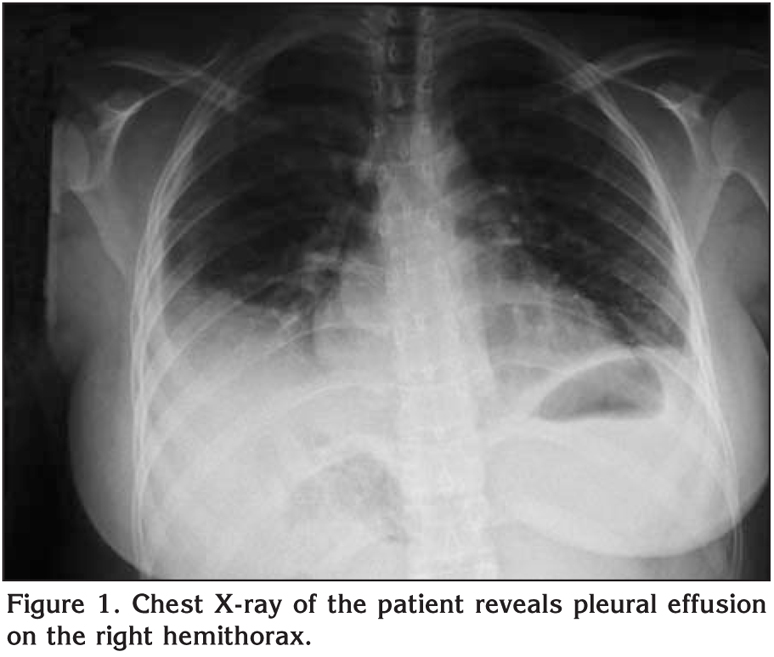
A 24-year-old female patient admitted to emergency service with abdominal pain, nausea and vomiting. She had white blood cell count of 7600 and a temperature of 36.7?C. Abdominal ultrasonography revealed immobile and noncomplicated appendix having an outer diameter of 13.4 mm. Exploratory laparotomy showed non-perforated appendicitis and appendicectomy was performed. At postoperative third day abdominal drains were pulled out. At the same day her body temperature increased to 38.5?C and leukocytosis of 12.100 was counted. On physical examination, laparotomy wound was clear, abdomen was mild tender without rebound. Ultrasonography showed no abnormal finding in the abdomen, but massive pleural effusion was detected in the right hemitorax. Physical examination revealed notable decrease in breath sounds on the right hemithorax and dullness in percussion. Chest X-ray showed a large right pleural effusion (Figure 1). Thoracentesis removed grossly purulent fluid with 90% polymorphonuclear leukocytes and 10% mononuclear leukocytes at microscopic evaluation. Tube thoracostomy was performed and 1500 mL of purulent material was immediately obtained.
The bacteriologic cultures of the pleural fluid grew E. coli and E. avium species. Effective antibiotics were administered according to the antibiogram. Full expansion of both lungs were revealed at control chest radiographs. However; although she had chest tube, she became febrile again. Abdominal ultrasonography revealed multilocular collections and formations of abscess, at the midline of the abdomen, near the mezo of the intestines with 60 x 30 mm in width, in the left psoas and iliopsoas muscle 90 x 55 mm in width, near the lateral of right psoas muscle 57 x 35 mm in width, right side of the caecum 25 x 20 mm in width and at the left posterolateral perirectal area 60 x 40 mm in width. Abscesses were drained by nonvascular interventional radiologic methods. Bacteriologic cultures of the abscesses grew the same with the thoracic ones, E. coli and E. avium. The patient did well and was dicharged home on the postoperative 32nd day.
Discussion
Thoracic empyema means the presence of pus in the pleural space from any cause. The definitive treatment of this suppurative process should be provided by complete drainage of loculated pus (3).
A few number of cases of acute appendicitis together with thoracic empyema have previously been reported (1,2). In all these cases, the diagnosis of thoracic empyema preceded by the diagnosis of perforated appendicitis. They could not be able to give an explanation for the association between acute appendicitis and thoracic empyema otherwise than abdominal infection.
Bacterial translocation is a description that include transition of viable bacteria from the gastrointestinal tract to bloodstream, across the intestinal wall (4,5,6,7). The definition may be broadened to include transmural passage of bacterial cell wall components such as lipopolysaccharide and peptidoglycan polysaccharide. After translocation, bacteria or their products reach the mesenteric lymph nodes, thereafter they both may disseminate throughout the body, causing sepsis or death of the host (6).
According to Berg, the three primary mechanisms promoting bacterial translocation in animal models were identified as: "(a) disruption of the ecologic GI equilibrium to allow intestinal bacterial overgrowth, (b) increased permeability of the intestinal mucosal barrier, and (c) deficiencies in host immune defenses". These mechanisms can play a synergistic role to support the systemic spread of enteric bacteria to cause lethal sepsis (4,7).
Lichtman stated that bacterial translocation and its complications had been shown clearly to occur in previous animal models, but its existence and importance in humans was difficult to ascertain (6). According to our knowledge, this case may be the first case with simultaneous occurence of thoracic empyema and acute appendicitis due to possible existance of bacterial translocation. Translocation of E. avium and E. coli through the compromised appendix mucosa leading in dissemination of the infection into the bloodstream was likely the main causative factor for the simultaneous presentation of both acute appendicitis and thoracic empyema. This is similar with bacteriel sepsis due to acute appendicitis which was described by Salamis (4). In this case, acute appendicitis was diagnosed on physical examination and abdominal ultrasonography. Since there was no chest X-ray before the appendicectomy we did not have objective feature about preoperative thoracic pathology. Symptoms of empyema presented at postoperative third day. Thus, it can be speculated that acute appendicitis and thoracic empyema appeared simultaneously. Bacterial growth in the empyema fluid consisted intestinal bacterial flora. Since the other abscess focuses in the abdomen had the same bacteries with those of empyema fluid and also were not connected to each other, bacteriel translocation and spreading through the bloodstream may be considered as an explanation for this case.
Both at the Law's cases and Herline's case, the diagnosis of the thoracic empyema was previous to acute appendicitis (1,2). Since the abdominal symptoms were mild, they could not be able to diagnose the appendicitis in time. We believe that between the period of appendicitis and perforation, bacteriel translocation occured for these cases, too.
Although quite rare, a thoracic empyema may accompany with an appendicitis. Multiple abdominal abscesses and thoracic empyema due to bacteriel translocation may be considered as an unexpected consequence of nonperforated acute appendicitis.
CONFLICT of INTEREST
None declared.
REFERENCES
- Law DK, Murr P, Bailey WC. Empyema, a rare presentation of perforated appendicitis. JAMA 1978; 240: 2566-7.
- Herline A, Burton EM, Hatley R. Thoracic empyema in a patient with acute appendicitis: a rare association. J Pediatr Surg 1994; 29: 1623-5.
- Lee SF, Lawrence D, Booth H, Morris-Jones S, Macrae B, Zumla A. Thoracic empyema: current opinions in medical and surgical management. Curr Opin Pulm Med 2010; 16: 194-200.
- Salemis NS. Acute appendicitis presenting with Klebsiella pneumoniae septicemia due to bacterial translocation. Am J Emerg Med 2009; 27: 1023.e3-4.
- Berg RD. Bacterial translocation from the gastrointestinal tract. Trends Microbiol 1995; 3: 149-54.
- Lichtman SM. Bacterial [correction of bacterial] translocation in humans. J Pediatr Gastroenterol Nutr 2001; 33: 1-10.
- Berg RD. Bacterial translocation from the gastrointestinal tract. Adv Exp Med Biol 1999; 473: 11-30.
Yaz??ma Adresi (Address for Correspondence):
Dr. Arif Osman Tokat,
SB Ankara E?itim ve Ara?t?rma Hastanesi,
G???s Cerrahisi Klini?i,
Cebeci, D?rtyol, ANKARA - TURKEY
e-mail: aostokat@hotmail.com