Akut izoniazid intoksikasyonu: konv?lziyon, koma ve asidozun nadir bir nedeni
Sinan UZMAN, T?may ULUDA? YANARAL, Mehmet TOPTA?, Alparslan KO?, Ayt?l TA?, G?l?en B?CAN
SB Haseki E?itim ve Ara?t?rma Hastanesi, Anesteziyoloji ve Reanimasyon Klini?i, ?stanbul.
?ZET
Akut izoniazid intoksikasyonu: konv?lziyon, koma ve asidozun nadir bir nedeni
Yayg?n kullan?m?na ra?men, izoniazidin intihar ama?l? al?m? T?rkiye'de nadir g?r?len bir durumdur. Konv?lziyon, koma ve metabolik asidoz ile kendini g?steren alkol al?m?yla birlikte olan bir akut izoniazid zehirlenmesi olgusu sunduk. Hasta intraven?z piridoksin uygulamas?yla ba?ar?l? bir ?ekilde tedavi edildi. Erken tan? ve yo?un bak?m ?nitesinde uygun tedavi akut izoniazid intoksikasyonu olan hastalarda mortalitenin ?nlenmesinde ?ok ?nemlidir.
Anahtar Kelimeler: Akut izoniazid intoksikasyonu, piridoksin, konv?lziyon, metabolik asidoz, koma.
SUMMARY
Acute isoniazid intoxication: an uncommon cause of convulzion, coma and acidosis
Sinan UZMAN, T?may ULUDA? YANARAL, Mehmet TOPTA?, Alparslan KO?, Ayt?l TA?, G?l?en B?CAN
Clinic of Anesthesiology and Reanimation, Haseki Training and Research Hospital, Istanbul, Turkey.???
Despite the widespread use, suicidal ingestion of isoniazid is a rare condition in Turkey. We reported a case of acute isoniazid intoxication associated with alcohol intake presenting with convulsion, coma and metabolic acidosis. The patient was treated successfully with intravenous pyridoxine administration. Early recognation and appropriate treatment in the intensive care unit is very important to prevent mortality in patients with acute isoniazid toxicity.
Key Words: Acute isoniazid intoxication, pyridoxine, convulsions, metabolic acidosis, coma.
Tuberk Toraks 2013; 61(1): 50-53 • doi: 10.5578/tt.1897
Geli? Tarihi/Received: 09/12/2012 - Kabul Edili? Tarihi/Accepted: 13/02/2013
INTRODUCTION
Isoniazid is the most widely used drug for the treatment and prophylaxis of tuberculosis. Acute isoniazid intoxication causes recurrent seizures, metabolic asidosis with a high anion gap, rhabdomyolysis, coma and even death (1). In adults, acute ingestion of as little as 1.5 grams can exhibit toxicity. Pyridoxine is the only effective antidote and should be administered in a dose equivalent to amount of isoniazid ingested (2). Isoniazid toxicity? should be considered in any patient who presents with unexplained refractory seizures and metabolic acidosis. In this report we presented a case of intoxication with ingestion of 1.2 g isoniazid.
CASE REPORT
A 21-years-old man was admitted to our emergency department with history of loss of consciousness that occurs suddenly and followed by seizure that were characterized as generalized tonic-clonic, lasted 5 to 6 minutes. On admission the patient was unconsciousness, his glaskow coma scale (GCS) score was 8, blood pressure was 100/60 mmHg, heart rate was 116 beats/minute. He had spontaneous and regular respiration. The pupils were isocoric and respond to light, bilaterally. His plantar response and deep tendon reflexes were normal. Fundoscopic examination and remaining physical findings were normal.
Routine laboratory investigations were performed at arrival. Arterial blood gas (ABG) analysis revealed a high anion gap metabolic acidosis (Table 1). Leukocyte count was 20.600/mL, blood glucose was 180 mg/dL. Other investigations including blood count, serum electrolytes, coagulation tests and renal and liver function tests were within normal limits. Urinanalysis, chest radiograph and cranial computed tomography were unremarkable.
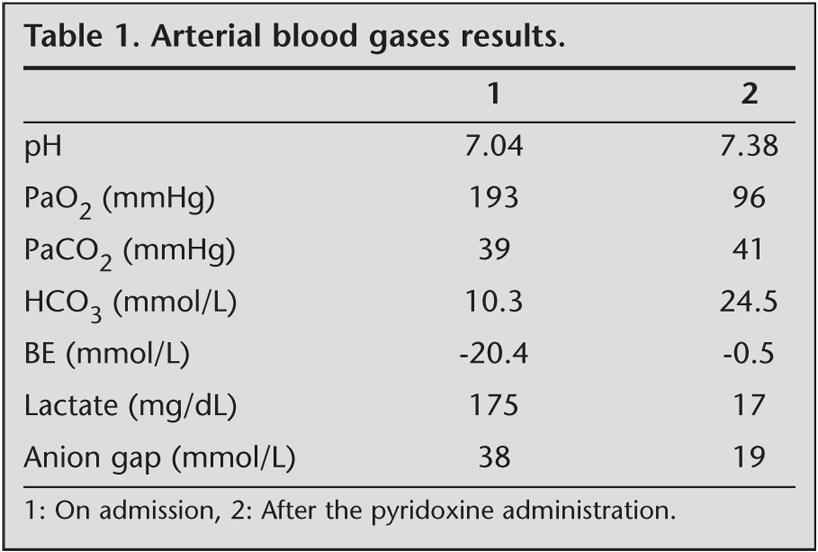
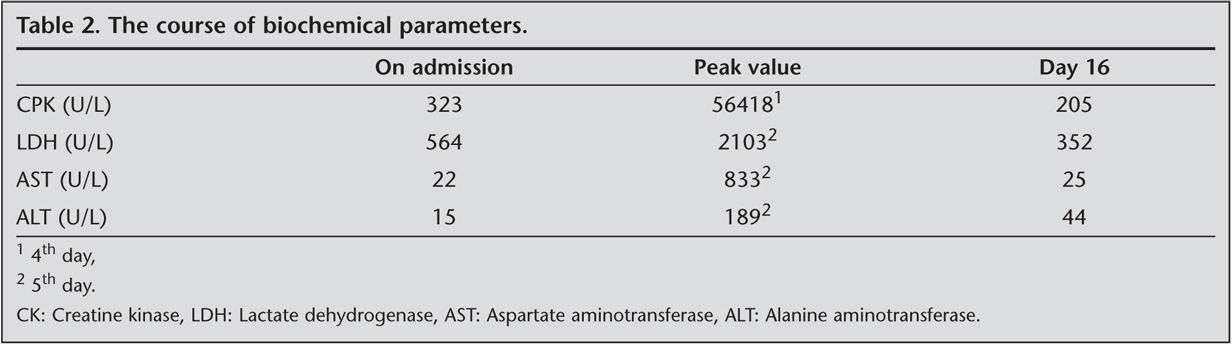
Two seizures occured within an hour after admission which subsided within five minutes after administration of 5 mg of diazepam intravenously. 50 mEq sodium bicarbonate was administered intravenously for the correction of metabolic acidosis. He was subsequently transferred to intensive care unit. At the admission of the patient to the intersive care unit his relatives said that he ingested some pills with beer about four hours ago but they haven't considered important. He had developed nausea and vomiting within half an hour. We learned that the patient was under tuberculosis treatment of isoniazid 300 mg + rifampicin 600 mg for two months. Isoniazid intoxication was suspected and a nasogastric catheter was administered and gastric lavage was performed followed by the administration of 60 g activated charcoal. Subsequently 5 g of pyridoxine were infused within the following 10 minutes. After the treatment was over, the patient regained consciousness and it was learned that the patient has taken four tablets of isoniazid for the purpose of suicide. ABG values on room air were returned to within normal values. Increasing levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), creatine phosphokinase (CPK) that were at their peak on the 4th-5th day and gradually decreased to its normal values on the 16th day (Table 2). Then the patient was discharged from hospital and was called back for control. At the control no hepatic and renal insufficiency was found.
DISCUSSION
Isoniazid is a popular suicide agent in populations with a high prevalence rate of tuberculosis. Previous studies showed that the patients who attempt suicide using isoniazid usually were under tuberculosis treatment with isoniazid or someone around them was (3,4,5). Although the incidence of tuberculosis is high in Turkey, suicide attempt with ingestion of isoniazid is rare (6,7). He was the first case of acute isoniazid intoxication that we experienced.
Depression may occur during isoniazid treatment and death of a relative may increase the suicide risk (5,8). Our patient was under isoniazid treatment for tuberculosis over the last two months and his grandfather was died a few days ago. After this event because of the behavioral changes that observed by his family members we speculated that he could be in depression. Screening for depression periodically of patients receiving isoniazid may be helpful for determination and prevention suicidal attempt.
Manifestations of acute isoniazid intoxication appear within 20 minutes to six hours after ingestion related to amount of ingestion (9,10). The earliest symptoms include nausea, vomiting, dizziness, blurred vision, slurring of speech and clinical triad of acute toxicity include repetitive seizures resistant to standart anticonvulsant therapy, metabolic acidosis with a high anion gap and coma (2).
Pyridoxal-5-phosphate, the active form of pyridoxine is a cofactor for glutamic acid decarboxylase in the gamma amino butyric acid (GABA) synthesis. Isoniazid inhibits this enzymatic pathway by binding to pyrdoxine and causes to decrease level of GABA in the brain, which is the major inhibitory neurotransmitter in the central nervous system. Reduction in GABA level increases the susceptibility to seizures. Although doses larger than 30 mg per kg often produce seizures even preventive doses of isoniazid may also cause seizures. When ingested in amounts of 80 to 150 mg per kg or more, isoniazid can be rapidly fatal (2,11,12). The ingested isoniazid dose was 20 mg/kg (totaly 1200 mg) in our patient. It was seen the clinical triad of isoniazid overdose? in our case and first seizure was seen four hours after ingestion.
Seizures are treated with diazepam and pyridoxine. Intravenous administration of diazepam 5-10 mg is the initial approach to seizure control and the dose repeated if necessary. Intravenous pyridoxine administration is spesific treatment of isoniazid-induced seizures. Pyridoxine should be given in a dose equivalent to the suspected amount of isoniazid ingested.? If the amount of isoniazid ingested is unknown 5 g of pyridoxine should be administered intravenously within 5-10 minutes (2,9,10,11,12,13).
In a recent study it has been showed that acute ethanol intake doesn't effect pharmacokinetics of isoniazid in therapeutic doses (14). But in an animal study it has been reported that ethanol pretreatment not only did not enhance the toxicity of isoniazid but, in fact, it reduced the severity of convulsions, although it did not change the mortality rate (15). Our patient was received a bottle of beer (500 mL, 5% ethanol) with isoniazid. No seizure is observed after the pyridoxine treatment. It may be related to potentiation of pyridoxine by ethanol partially.
Production of lactic acid secondary to seizures cause acute metabolic acidosis in isoniazid intoxication and seizure control is essential to prevent metabolic acidosis (2). A transient increase in base deficit occurs after the pyridoxine treatment (16). Intravenous sodium bicarbonete infusion before the administration of pyridoxine may be useful to prevent increasing severity of acidosis.??
Elevation of CPK occured in 59.6% of cases and it was associated with increasing doses of isoniazid, beginning with 2.4 g. It has been showed a significant correlation between the duration of seizure but not the number of seizure and the elevation of CPK (17). In our case we concluded that long lasting seizures were responsinle significant increase in CPK levels.
Isoniazid is one of the cause of drug induced seizures in the emergency department and it should be considered in any patient presenting with generalize convulsions and metabolic acidosis. Early recognition and spesific treatment with pyridoxine will prevent the mortality.
CONFLICT of INTEREST
None declared.
REFERENCES
- Shannon MW, Lovejoy FH Jr. Isoniazid. In: Haddad LM, Winchester JF (eds). Clinical Management of Poisoning and Drug Overdose. 2nd ed. Philadelphia: Saunders, 1990: 970-5.
- Romero JA, Kuczler FJ. Isoniazid overdose. Recognition and management. Am Fam Physician 1998; 57: 749-52.
- Cameron WM. Isoniazid overdose. Can Med Assoc J 1978; 118: 1413-5.
- Sullivan EA, Geofffroy P, Weisman R, Hoffman R, Frieden TR. Isoniazid poisonings in New York City. J Emerg Med 1998; 16: 57-9.
- De Lara ACF, Moral PGL, Cuison RJ. Isoniazid overdose at the Santo Tomas University Hospital-Clinical Division: a seven year review. Phil J Internal Med 1997; 35: 195-200.
- Ozbay B, Sezgi C, Altinoz O, Sertogullar?ndan B, Tokgoz N. Evaluation of tuberculosis cases detected in our region between 1999 and 2003. Tuberk Toraks 2008; 56: 396-404.
- Topcu I, Yentur EA, Kefi A, Ekici NZ, Sakarya M. Seizures, metabolic acidosis and coma resulting from acute isoniazid intoxication. Anaesth Intensive Care 2005; 33: 518-20.
- Nolan CM, Elarth AM, Barr HW. Intentional isoniazid overdosage in young Southeast Asian refugee women. Chest 1998; 93: 803-6.
- Tai DY, Yeo JK, Eng PC, Wang YT. Intentional overdosage with isoniazid: case report and review of literature.? Singapore Med J 1996; 37: 222-5.
- Agrawal RL, Dwivedi NC, Agrawal M, Jain S, Agrawal A. Accidental isoniazid poisoning-a report. Indian J Tuberc 2008; 55: 94-6.
- Tajender V, Saluja J. INH induced status epilepticus: response to pyridoxine. Indian J Chest Dis Allied Sci 2006; 48: 205-6.
- Martinjak-Dvorsek I, Gorjup V, Horvat M, Noc M. Acute isoniazid neurotoxicity during preventive therapy. Crit Care Med 2000; 28: 567-8.
- Santucci KA, Shah BR, Linakis JG. Acute isoniazid exposures and antidote availability. Pediatr Emerg Care 1999; 15: 99-101.
- Dattani RG, Harry F, Hutchings AD, Routledge PA. The effects of acute ethanol intake on isoniazid pharmacokinetics. Eur J Clin Pharmacol 2004; 60: 679-82.
- Chin L, Sievers ML, Herrier RN, Picchioni AL. Potentiation of pyridoxine by depressants and anticonvulsants in the treatment of acute isoniazid intoxication in dogs. Toxicol Appl Pharmacol 1981; 58: 504-9.
- Lovecchio F, Curry SC, Graeme KA, Wallace KL, Suchard J. Intravenous pyridoxine-induced metabolic acidosis. Ann Emerg Med 2001; 38: 62-4.
- Panganiban LR, Makalinao IR, Corte-Maramba NP. Rhabdomyolysis in isoniazid poisoning. J Toxicol Clin Toxicol 2001; 39: 143-51.
Yaz??ma Adresi (Address for Correspondence):
Dr. Sinan UZMAN,
SB Haseki E?itim ve Ara?t?rma Hastanesi,
Anesteziyoloji ve Reanimasyon Klini?i,
Fatih, ?STANBUL - TURKEY
e-mail: drsinanuzman@yahoo.com