T?rkiye'deki cezaevlerinde akci?er t?berk?lozu insidans?:
Olgu bulma ve tarama stratejilerinin ?nemi
G?l ?NGEN1, ?ermin B?REK??1, ?zlem Saniye ??MEL?2, Nur B?RGEN2, G?ls?m KARAG?L3,
Salih AKG?N3, Zeki KILI?ASLAN4, Sema UMUT1
1 ?stanbul ?niversitesi Cerrahpa?a T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, ?stanbul,
2 Adli T?p Kurumu, ?stanbul,
3 ?stanbul Verem Sava? Dispanseri, ?stanbul.
4 ?stanbul?niversitesi ?stanbul T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, ?stanbul.
?ZET
T?rkiye'deki cezaevlerinde akci?er t?berk?lozu insidans?: Olgu bulma ve tarama stratejilerinin ?nemi
Giri?: Bu ?al??man?n amac?, T?rkiye'de Marmara B?lgesi'ndeki cezaevlerinde, akci?er t?berk?lozu insidans?n? ara?t?rmak ve T?rkiye'deki genel akci?er t?berk?lozu insidans?yla kar??la?t?rmakt?r.
Hastalar ve Metod: Marmara B?lgesi'nde d?rt ?ehirde bulunan toplam 10 cezaevindeki t?m h?k?ml?ler ?al??maya al?nd?. Taramalar Ocak 2006-Ocak 2007 tarihleri aras?nda yap?ld?. Radyolojik taramalar mobil-X ray cihaz?yla yap?ld?. T?berk?loz ??phesi olan olgulardan bakteriyolojik inceleme ama?l? balgam ?rne?i al?nd?. Akci?er grafileri birbirinden ba??ms?z d?rt hekim taraf?ndan ayr? ayr? de?erlendirildi.
Bulgular: Radyolojik olarak toplam 4615 h?k?ml? tarand?. ?? y?z bir (%7)'i kad?n, 4314 (%93)'? erkekti. Kad?nlar?n ya? da??l?m? 16-59 y?l, erkeklerin ya? da??l?m? 14-72 y?l idi. T?m h?k?ml?lerin 398/4615 (%8.6)'ini, ya? da??l?m? 14-18 y?l olan gen?ler olu?turmaktayd?. Radyolojik olarak t?berk?loz d???n?len 130 olgudan bakteriyolojik inceleme ama?l? ?? kez balgam ?rne?i al?nd?. Y?z otuz olgunun tamam? erkek ve ya? ortalamas? 33 ? 10 y?l idi, be?ine yayma ya da k?lt?r pozitif akci?er t?berk?lozu tan?s? koyuldu. ?al??mam?zda cezaevlerindeki t?berk?loz prevalans? 108/100.000 olarak bulundu. Bu de?er, ?al??mam?z?n yap?ld??? tarihteki T?rkiye'deki genel t?berk?loz prevalans?n?n d?rt kat? y?ksekliktedir.
Sonu?: T?rkiye'de cezaevlerindeki h?k?ml?ler, t?berk?loz a??s?ndan ?nemli risk gruplar?ndand?r. ?al??mam?z, cezaevlerinde uygun olgu bulma ve tarama stratejilerine duyulan ihtiyac? vurgulamaktad?r.
Anahtar Kelimeler: T?berk?loz, cezaevi, aktif t?berk?loz tarama.
SUMMARY
Pulmonary tuberculosis incidence in Turkish prisons: importance of screening and case finding strategies
G?l ?NGEN1, ?ermin B?REK??1, ?zlem Saniye ??MEL?2, Nur B?RGEN2, G?ls?m KARAG?L3,
Salih AKG?N3, Zeki KILI?ASLAN4, Sema UMUT1
1 Department of Chest Diseases, Faculty of Cerrahpasa Medicine, Istanbul University, Istanbul, Turkey,
2 Forensic Medicine Institute, Istanbul, Turkey,
3 Istanbul Tuberculosis Control Dispensary, Istanbul, Turkey,
4 Department of Chest Diseases, Faculty of Istanbul Medicine, Istanbul University, Istanbul, Turkey.
Introduction: The purpose of this study was to evaluate the burden of pulmonary tuberculosis in 10 prisons mostly located in the Marmara Region of Turkey, and to compare them with the country incidence.
Patients and Methods: All the inmates in ten prisons mostly located in the four cities in the Marmara Region of Turkey were enrolled in this study. Tuberculosis screening was done between January 2006-January 2007. Radiological screening for tuberculosis was performed by the mobile X-ray system and it was followed by bacteriological analysis of sputum for tuberculosis suspects. Four physicians evaluated the X-rays independently.
Results: Four thousand six hundred and fifteen prisoners were detected by radiological screening. Three hundred and one (7%) of them were female and 4314 (93%) were male, age range was between 14-72 years. Age ranges of female and male prisoners were 16-59 and 14-72 respectively. 398/4615 (8.6%) were young adults inmates with an age range of 14-18. Radiological abnormalities consistent with tuberculosis were found in 130 chest X-rays and followed by sputum bacteriology. Smear and culture positive pulmonary tuberculosis diagnosed in five out of 130, were all male with mean age 33 ? 10 years. Tuberculosis prevalence in the prisons was found to be 108/100.000 which was four times higher than the overall incidence of tuberculosis in Turkey in the year which the present study was conducted.
Conclusion: Prisoners are one of the most important risk groups with high burden of tuberculosis in Turkey. This result highlights the need for adequate case- finding strategies in prisons.
Key Words: Tuberculosis, prisoners, active tuberculosis screening.
Tuberk Toraks 2013; 61(1): 21-27 • doi: 10.5578/tt.2773
Geli? Tarihi/Received: 17/08/2011 - Kabul Edili? Tarihi/Accepted: 04/07/2012
INTRODUCTION
Approximately 10 million people around the world are incarcerated, mostly in prisons. Occurrence of active tuberculosis in prisons is usually reported to be much higher than average levels reported for the corresponding general population (1,2,3). Late tuberculosis case finding and delays in treatment are common problems in many prisons (2). Conditions within prisons (poor health services, poor nutrition, poor physical condition, drug addiction and presence of other diseases) are conductive to the spread of TB (4,5). Moreover, prisons represent a reservoir for disease transmission; the tuberculosis infection may spread into the general population through prison staff, visitors, and close contacts of released prisoners (6,7).
In addition to the universal World Health Organization (WHO) Directly Observed Treatment Short-course strategy, several measures have been proposed by WHO and the Red Cross to control tuberculosis in prisons including mass screening of prisoners based on symptoms and the systematic detection of tuberculosis at entry point (2,8,9,10,11). In Turkey the administration of prisons is under the responsibility of three different authorities having different bureaucratic rules: Ministry of Health (MoH), Ministry of Justice (MoJ) and Ministry of Internal Affairs (MoIA). Although there is a protocol accepted by MoH and MoJ for control in prisons which highlights the necessity of annual tuberculosis screening, it is not well implanted or if done the outcomes are not well assessed due to the lack of coordination between these three authorities. That must be one of the reasons, to our knowledge why there are two published papers about the prevalence of tuberculosis in Turkish prisons (12,13). To start this study, we got permission from all the authorities mentioned above to assess and use outcomes. The aim of this study is to evaluate the burden of tuberculosis in ten prisons mostly located in the Marmara Region of Turkey, and to compare them with the country incidence.
PATIENTS and METHODS
Between January 2006-January 2007 all the inmates in 10 prisons mostly located in the four cities in the Marmara Region of Turkey were enrolled in this study. Each inmate was interviewed using a standardised questionnaire containing questions on demographic, clinical variables [including cough (> 3 weeks), sputum, fever, weakness, weight loss, loss of appetite, night sweats], history of tuberculosis treatment and smoking habits. Each inmate underwent for microfilm examination that is used in community based screening for tuberculosis by the mobile X-ray system in Turkey. All microfilms were evaluated by three physicians (two chest physicians, one dispensary physician) who were blinded to the subjects' sign and symptoms. Radiologically suspected tuberculosis lesions on microfilms were selected for standart posterior-anterior chest X-rays. Agreement were settled by concensus between the two specialists. Inmates with any pulmonary, mediastinal or pleural abnormality in standart posterior-anterior chest X-rays were selected for sputum examination. Three early morning sputum samples were collected from tuberculosis suspects on different days. Microscopic sputum smear examination for acid-fast bacilli (AFB) was performed after Ziehl-Neelsen staining. All sputum samples were cultured on L?wenstein-Jensen medium.
Diagnostic criteria for pulmonary tuberculosis cases were defined as (8);
Bacteriologically positive cases: Subjects with two smear positive results by direct microscopic examination, or one smear positive sample with chest X-ray abnormalities consistent with active pulmonary tuberculosis, or positive culture for Mycobacterium tuberculosis.
Bacteriologically negative cases: Patient with;
1. At least three sputum specimens negative for AFB, and
2. Radiographic abnormalities consistent with active pulmonary tuberculosis, and
3. No response to a course of broad spectrum antibiotics, and
4. Decision by a clinician to treat with a full course of anti-tuberculosis chemotherapy, is accepted as smear negative case.
Collected data were recorded using SPSS 13.0 version for Windows. The protocol was approved by Istanbul Health Directorate and by Republic of Turkey, Ministry of Justice.
RESULTS
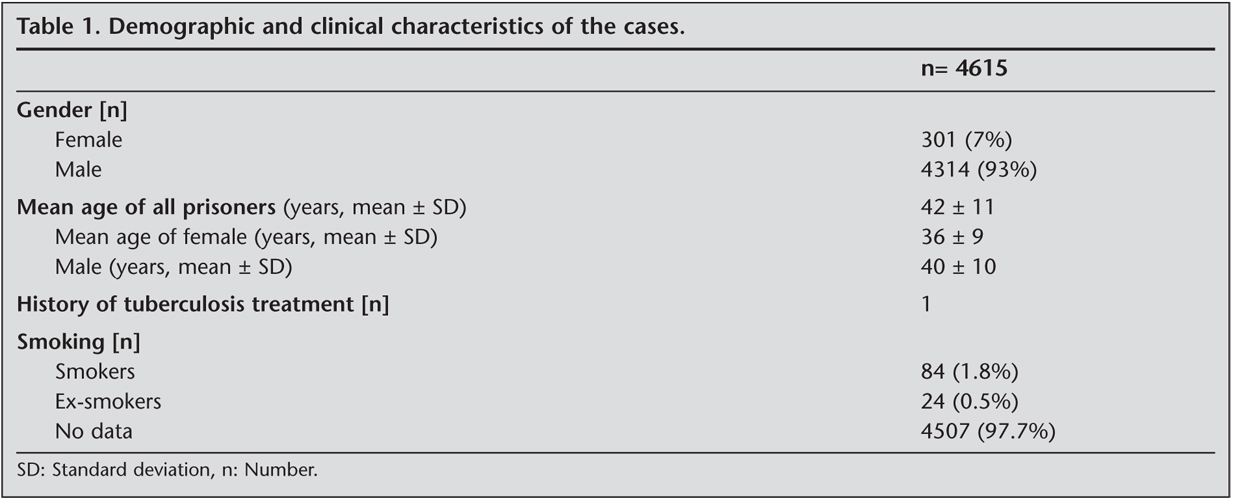
During the study period, a total of 4615 prisoners in 10 prisons, 301 (7%) female and 4314 (93%) male, were screened by microfilm. The mean age of all prisoners was 42 ? 11 years. The mean age of female and male prisoners were 36 ? 9 and 40 ? 10 years. 398/4615 (8.6%) were young adults inmates with an age range of 14-18 years. The demographic and clinical characteristics of the inmates are shown in Table 1.
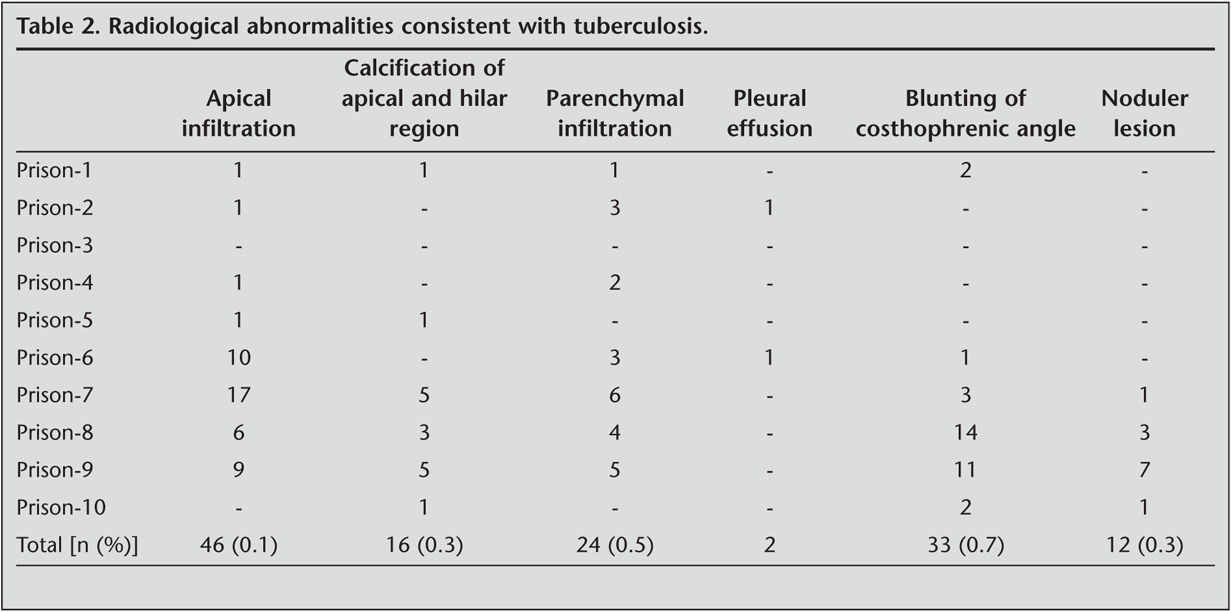
Radiological abnormalities consistent with tuberculosis were found in 130 microfilms and followed by sputum bacteriology. Radiological abnormalities were as follows: apical infiltration in 46 (0.1%), calcification of apical and hilar region in 16 (0.3%), parenchymal infiltration in 24 (0.5%), pleural effusion in 2, blunting of the costophrenic angle in 33 (0.7%) and noduler lesions in 12 (0.3%) prisoners, as shown in Table 2.
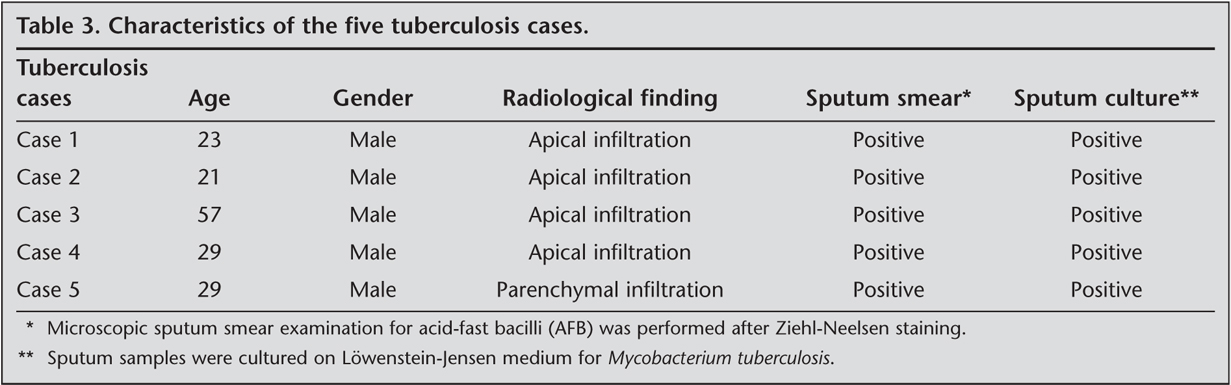
Smear and culture positive pulmonary tuberculosis diagnosed in 5 out of 130 , were all male with mean age 33 ? 10 years (Table 3).
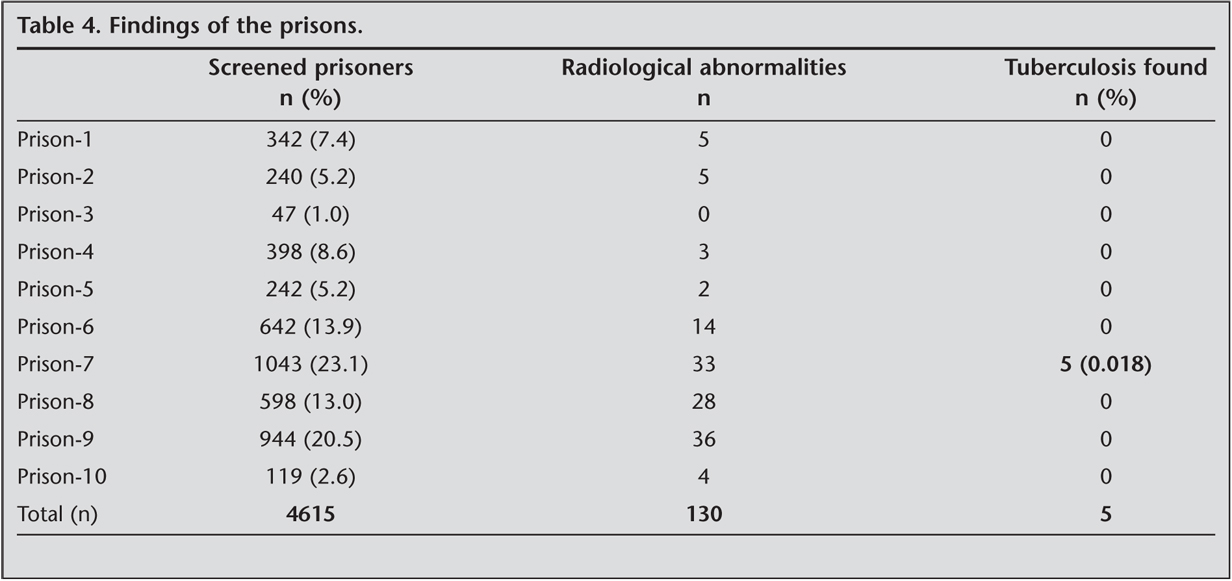
All of the tuberculosis cases were at the same prison (Prison 7) which was the biggest and most crowded of all. Findings of each prison were shown in Table 4.
The prevelance of tuberculosis was found to be 108/100.000 in the prisons which is four times higher than the country prevelance (29/100.000) in 2006 that present study was conducted (14).
DISCUSSION
Prisons represent dynamic communities where at-risk groups congregate in a setting that exacerbates disease and its transmission, including tuberculosis (3).
Although prisons are closed institutions, the prisoners are often mobile within various prisons, inside the prison and even between different institutions such as courts. At the end they are released into the community with insufficient, incomplete and interrupted treatment.
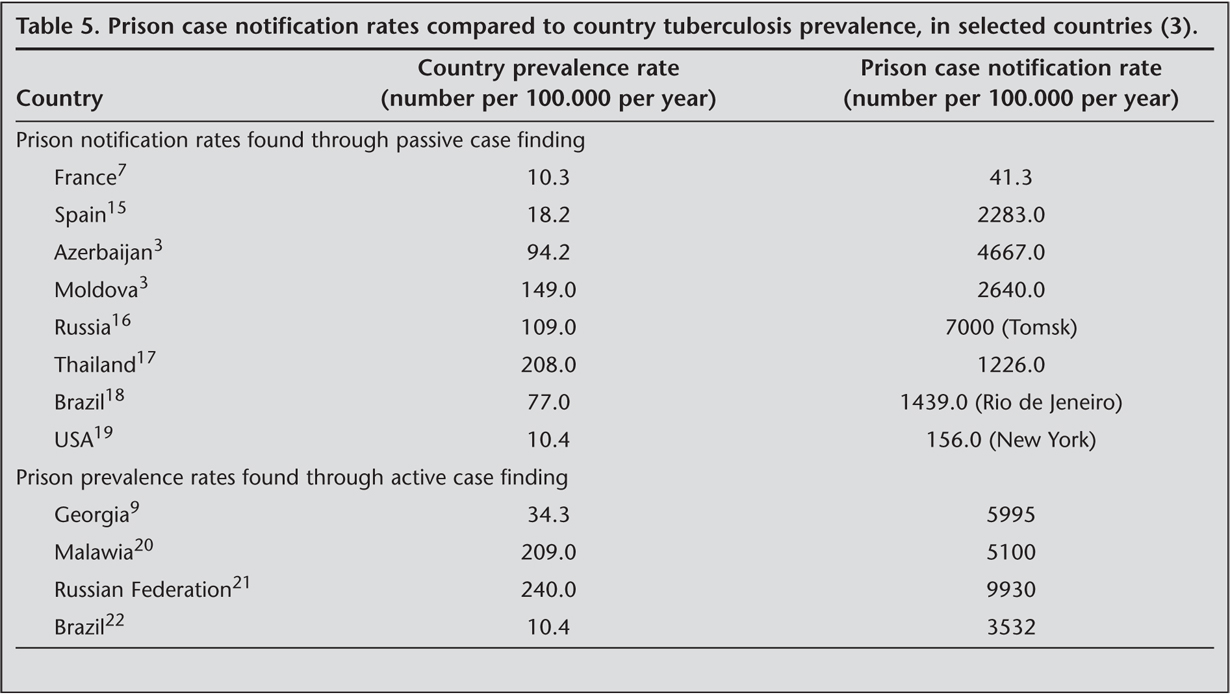
Other common issue is the administrative problems of the prisons in Turkey. Three different ministries (MoH, MoJ, MoIA) are responsible to report prison health data. This complex administrative structure often interferes routine screening protocol, data reporting system and the implementation of effective tuberculosis control, so delayed diagnosis, and inadequate treatment results in prolonged transmission. To obtain most reliable data we initially built a bridge between these three ministries and urged them to collaborate with each other. Our study has shown that active tuberculosis prevalence (108/100.000) among prisoners in Turkey was four times higher than the country prevalence (29/100.000) in 2006 (14). This result is smilar to worldwide. The prevalence rates of tuberculosis in prisons usually exceed prevalence rates in the specific country substantially. As shown in Table 5, tuberculosis rates of over 3000 per 100.000, as compared to the general population, are not unusual (3).
There are only two studies about prevalence of tuberculosis in prisons in Turkey (12,13). Kiter and colleagues obtained data from a systematic annual tuberculosis screening programme undertaken in Nazilli District Prison between 1997 and 2001, and found that the mean point prevalence of tuberculosis in prisons was 341 per 100.000 prisoners (12). Elbek and colleagues screened the 757 microfilms of 763 prisoners in Gaziantep E-type petientiary to investigate the prevalence of tuberculosis in prisons in Turkey, they found twenty cases who were suggested to have sequelae or active pulmonary tuberculosis on microfilm findings and were referred to Gaziantep dispensary for detailed examination for tuberculosis, but Elbek and colleagues didn't complete their study as most of the prisoners, including the 20 suspected cases, were discharged following new legislation (13).
Risk factors for tuberculosis transmission in prisons include overcrowding, inadeguate ventilation, poor hygiene, poor health services, poor nutrition, poor physical condition, drug addiction and presence of other diseases (4,5,12). One of the results of our study was that all active tuberculosis cases were belonging to the same prison (Prison 7) which was the biggest and the most crowded of all. Prison-7 that was built on system of wards with 50 or more prisoners in each ward. After this result, the conditions of Prison-7 were renovated, and type of Prison-7 was changed from ward type to the another type that was built on a system of cells constructed for one or three people.
Case finding and treatment of tuberculosis disease are currently the principal means of controlling transmission and reducing incidence (23). Case-finding strategies for tuberculosis can be divided into two: first, passive case finding (PCF) strategy is defined as detecting active tuberculosis disease among symptomatic patients who present to medical services for diagnosis of symptoms; second, active case finding (ACF) strategy is defined as detecting the people with tuberculosis who have not applied to a diagnostic service by themselves (23). PCF is widely used in developing countries based on the recommendation of World Health Organization (WHO) (24). Despite, ACF strategies are more costly due to need of manpower and budget, they have ability to find a large number of tuberculosis cases. As is seen in publications, targeted ACF has been effective for prisons, homeless and nursing homes (23). A combination of questionnaires and radiography is also suggested (2). In our study, we found that the most common radiological abnormalities among prisoners is apical infiltration (in 46 of 4615; 0.1%), also apical infiltration is present in 4 (80%) of five prisoners with diagnosed active tuberculosis. Similar with our result, Elbek and colleagues reported that the apical infiltration is the most common radiological abnormality among prisoners (in 16 of 757; 2.1%) in Gaziantep E type penitentiary (13).
Tuberculosis screening activities are not systematically performed in all Turkish prisons. With our study, there have been only three published papers that reported the prevalence of tuberculosis among prisoners in Turkey. We strongly recommend that targeted ACF screening protocols should be routinely performed for all prisons in Turkey.
Our study had several limitations: lack of incidence of extrapulmonary tuberculosis cases, and lack of the ratio of demographic and clinical characteristics, due to loss of the most of the files; it would be better to give the results of tuberculosis treatment of inmates with diagnosed active tuberculosis.
In conclusion, prisons are one of the most important risk groups with high burden of tuberculosis in Turkey. Results of our study highlights the need for adequate case-finding strategies in prisons. We strongly recommend that targeted ACF screening protocols should be routinely performed for all prisons in Turkey. The collaboration between different ministries and tuberculosis dispenseries is essential for application and success of such protocols for tuberculosis control in prisons.
Acknowledgements
The authors would like to thank to Fuat Demir, Chief Executive Officer of Istanbul Association Against Tuberculosis, for his help, cooperation and support.
CONFLICT of INTEREST
None declared.
REFERENCES
- Baussano I, Williams BG, Nunn P, Beggiato M, Fedeli U, Scano F. Tuberculosis incidence in prisons: a systematic review. PLoS Med 2010; 7: e1000381. doi: 10.1371/journal.pmed. 1000381.
- Bone A, Aerts A, Grzemska M, Kimerling M, Kluge H, Levy M, et al. Tuberculosis control in prisons: A Manual for Programme Managers. Geneva: World Health Organization, 2000.
- Dara M, Grzemska M, Kimerling ME, Reyes H, Zagorskiy A. Guidelines for control of tuberculosis in prisons. The Global Health Bureau, Office of Health, Infectious Disease and Nutrition (HIDN), US Agency for International Development, 2009.
- Coninx R, Maher D, Reyes H, Grzemska M. Tuberculosis in prisons in countries with high prevalence. BMJ 2000; 320: 440-2.
- PLoS Medicine Editors, Barbour V, Clark J, Jones S, Veitch E. The health crisis of tuberculosis in prisons extends beyond the prison walls. PLoS Med 2010; 7: e1000383
- Niveau G. Prevention of infectious disease transmission in correctional setting: a review. Public Health 2006; 120: 33-41.
- Aerts A, Hauer B, Wanlin M, Veen J. Tuberculosis and tuberculosis control in European prisons. Int J Tuberc Lung Dis 2006; 10: 1215-23.
- Revised international definitions in tuberculosis control. World Health Organization; International Union Against Tuberculosis and Lung Disease; Royal Netherlans Tuberculosis Association. Int J Tuberc Lung Dis 2001; 5: 213-5.
- Aerts A, Habouzit M, Mschiladze L, Malakmadze N, Sadradze N, Menteshashvili O, et al. Pulmonary tuberculosis in prisons of the ex-USSR state Georgia: results of a nation-wide prevalence survey among sentenced inmates. Int J Tuberc Lung Dis 2000; 4: 1104-10.
- Prevention and control of tuberculosis in correctional and detention facilities: recommendations from CDC. Endorsed by the Advisory Council for the Elimination of Tuberculosis, the National Commission on Correctional Health Care, and the American Correctional Association. MMWR Recomm Rep 2006; 55: 1-44.
- Layton MC, Henning KJ, Alexander TA, Gooding AL, Reid C, Heyman BM, et al. Universal radiographic screening for tuberculosis among inmates upon admission to jail. Am J Public Health 1997; 87: 1335-7.
- Kiter G, Arpaz S, Keskin S, Sezgin N, Budin D, Seref O. Tuberculosis in Nazilli District prison, Turkey, 1997-2001. Int J Tuberc Lung Dis 2003; 7: 133-8.
- Elbek O, B?rek?i S, T?l? M, Bayram H, Dikensoy O. Results of microfilm screening in gaziantep E-type penitentiary. Int J Tuberc Lung Dis 2006; 10: 1419-20.
- Republic of Turkey Ministry of of Health. Primary Health Care Directorate 2006, www.saglik.gov.tr
- Chaves F, Dronda F, Cave MD, Alonso-Sanz M, Gonzalez-Lopez A, Eisenach KD, et al. A longitudinal study of transmission of tuberculosis in a large prison population. Am J Respir Crit Care Med 1997; 155: 719-25.
- Wares DF, Clowes CI. Tuberculosis in Russia. Lancet 1997; 350: 957.
- Nateniyom S, Jittimanee SX, Ngamtrairai N, Jittimanee S, Boonpendetch R, Moongkhetklang V, et al. Implementation of the DOTS strategy in prisons at provincial level, Thailand. Int J Tuberc Lung Dis 2004; 8: 848-54.
- Sanchez A, Gerhardt G, Natal S, Capone D, Espinola A, Costa W, et al. Prevalence of pulmonary tuberculosis and comparative evaluation of screening strategies in a Brazilian prison. Int J Tuberc Lung Dis 2005; 9: 633-9.
- Valway SE, Greifinger RB, Papania M, Kilburn JO, Woodley C, DiFerdinando GT, et al. Multidrug-resistant tuberculosis in the New York State prison system, 1990-1991. J Infect Dis 1994; 170: 151-6.
- Nyangulu DS, Harries AD, Kang'ombe C, Yadidi AE, Chokani K, Cullinan T, et al. Tuberculosis in a prison population in Malawi. Lancet 1997; 350: 1284-7.
- Coker RJ, Dimitrova B, Drobniewski F, Samyshkin Y, Balabanova Y, Kuznetsov S, et al. Tuberculosis control in Samara Oblast, Russia: institutional and regulatory environment. Int J Tuberc Lung Dis 2003; 7: 920-32.
- Sanchez A, Larouze B, Espinola AB, Pires J, Capone D, Gerhardt G, et al. Screening for tuberculosis on admission to highly endemic prisons? The case of Rio de Janeiro State prisons. Int J Tuberc Lung Dis 2009; 13: 1247-52.
- Gloub JE, Mohan CI Comstock GW, Chaisson RE. Active case finding of tuberculosis: historical perspective and future prospects. Int J Tuberc Lung Dis 2005; 9: 1183-203.
- World Health Organization. Global Tuberculosis Control 2010. www.who.int/tb/publications/globalreport/
Yaz??ma Adresi (Address for Correspondence):
Dr. ?ermin B?REK??,
?stanbul ?niversitesi Cerrahpa?a T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
?STANBUL - TURKEY
e-mail: serminborekci@yahoo.com.tr