Massive hemoptysis, the etiology is aorto-bronchial fistula
Ey?p
Sabri U?AN1, Ahmet Yi?it G?KTAY2, Funda ULUORMAN1,
Canan KARAMAN1,
?evket Baran U?URLU3
1 Dokuz Eyl?l ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, ?zmir,
2 Dokuz Eyl?l ?niversitesi T?p Fak?ltesi, Radyoloji Anabilim Dal?, ?zmir,
3 Dokuz Eyl?l ?niversitesi T?p Fak?ltesi, Kalp ve Damar Cerrahisi Anabilim Dal?, ?zmir.
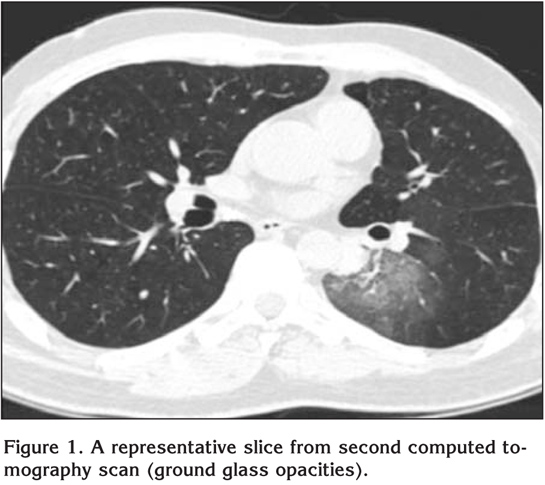
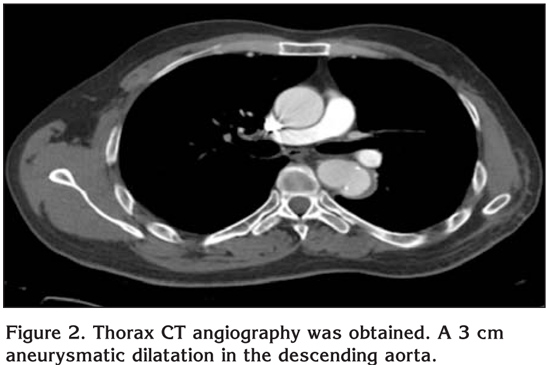
A 41-year-old man presented with massive hemoptysis. On physical examination, auscultation of the lung reveals inspiratory crackles, predominantly located in the lower posterior lung zones and auscultation of the heart reveals 2/6 systolic souffle in all of the cardiac zones. During the observation in emergency room, the patient's hemoglobin values decreased from 15.5 mg/dL to 11.7 mg/dL. Because of this reason, erytrocyte suspension transfusion had been processed. Bilateral diffuse infiltration could be seen in postero-anterior chest X-ray. In the computed tomography (CT) of thorax, there was bilateral parenchymal ground glass opacities and consolidations (Figure 1). During bronchoscopy, active bleeding from bilateral bronchial system was observed. Since intraalveolar hemorrhage was considered at the patient, etiology oriented examinations were evaluated. Patient was extubated after the hemopthysis had been controlled and then, he was transferred to the chest diseases clinique from the intensive care unit. Both in bronchoscopic samples and sputum samples of the patient, there was no acid resistant bacterium in direct microbiological examination and cultures for acid resistant bacterium were negative. In the evaluation of the patient in terms of vasculitic syndromes; anti-nuclear antibody, anti-neutrophilic cytoplasmic antibody and ENA panel were detected and they were all negative. In the medical consultation made with cardiothoracic surgery, there was no additional suggestion. In the control bronchoscopy for hemorrhage, only a former bleeding focal point on the left main bronchi has been observed. During bronchoscopy; bronchial lavage, bronchoalveolar lavage (from the right middle lobe bronchi) and transbronchial biopsy samples were obtained. However, those samples weren't useful for a specific diagnosis. Three months later, in the control CT of thorax of the case, ground glass opacities except the ones at the left lower lobe were all regressed. And, because of the relationship of this appearance with the vascular structures, a thorax CT angiography was obtained. A 3 cm aneurysmatic dilatation in the descending aorta is exposed (Figure 2). The patient asked for an angiography both for diagnosis and for treatment.
?In the story of the patient, there is an aorta coarctation operation. Because of this reason, massive hemoptysis from aortobronchial fistula (which is related with aorta aneurysm) should be considered in differential diagnosis. According to the high resolution computed tomography (HRCT) of thorax, ground glass opacities which spread out from the left side of aorta operation area to parenchyma, approves aorto-bronchial fistula (ABF).
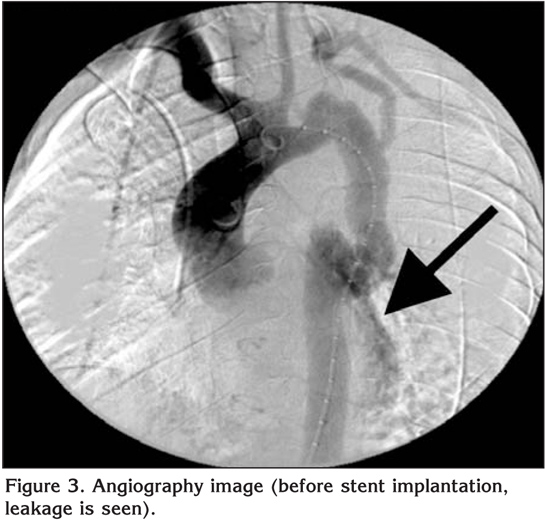
Surgical treatment can be considered as a treatment choice as well as intravascular stent implantation. In the HRCT of thorax and in the angiography, a blood leakage from graft to bronchial system can be seen. However, after the stent implantation, it's observed that the leakage completely stopped (Figure 3,4).

DISCUSSION
Aorta coarctation represents 3-5% of congenital cardiac malformations (1). Surgical techniques for repairment of coarctation, include Dacron patch plasty, left subclavian flap aortoplasty and coarctectomy with end-to-end anastomosis. The primary techniques seem to be successful but pseudo aneurysms occur in %9 of patients after surgery (2). For the surgical treatment of aorta coarctation, Vosschulte defined the patch aortoplasty technique in 1957 for the first time as an alternative for resection and anastomosis. However, in the later results of the patients, who had a surgery with this technique, an aneurysm formation is observed in anastomosis line (3). The traditional surgical methods of treating ABF involve thoracotomy with aortic repair and by-pass grafting (4). In the literature, there are different numbers given for the aneurysm frequency that occurs just after patch aortoplasty. Aneurysm frequency is expressed as 27% in a series of 68 adults. In some cases, cardiopulmonary by-pass and hypothermic circulatory arrest are required for repair (5). When treated electively without evidence of ABF, the perioperative mortality for these aneurysms is 13.8% (6,7). However, if they are treated urgently after fistula occurs; perioperative mortality rises to 24-41% (8).
ABF is an uncommon condition that causes massive hemoptysis and is generally fatal if surgical intervention is delayed. Chronic thoracic aneurysm and infection of the thoracic aortic graft are the most common causes of ABF (9). Although hemoptysis is a nonspecific symptom, its occurrence in a patient with previous surgery on the thoracic aorta should raise the suspicion of ABF (9).
Hemoptysis cases have been reported after the aort coarctation repairment operations as a result of the postoperative ABFs (5,10,11). As observed in the previous cases, aneurysm formation most often occurred in patients who had undergone synthetic patch aortoplasty (11,12).
Surgical intervention can be performed in most patients with a relatively low risk of death (9). In our case, intravascular stent implantation method was preferred instead of surgical methods. There was no complication after the stent implantation procedure and the treatment method was successful. The intravascular treatment methods, used for aort coarctation which occurs just after the surgery, are quite new. However, they are less invasive techniques.
The possibility of pseudoaneurysm and ABF should be kept in mind in the differential diagnosis of hemoptysis in patients with a history of patch repair of aortic coarctation (9). In the treatment of the ABFs, intravascular treatment methods can be used as well as surgical methods as in our case.
CONFLICT of INTEREST
None declared.
REFERENCES
- Reidy J. Endorgrafting in aneurysms associated with coarctation. In: Amor M, Bergeron P, Castriota F, Cremonesi A, Mathias K, Rathiel D (eds). Thoracic Aorta Endografting-a Multidisciplinary Approach. Marseille: Cam Co, 2004: 165-9.
-
Ince H, Petzch M, Rehders T, Kische S, K?rber T, Weber F, et al. Percutaneous
endovascular repair of aneurysm after previous coarctation surgery. Circulation
2003; 108: 2967-70.
[?zet] [Tam Metin] [PDF] - Backer CL, Mavroudis C. Coarctation of the aorta and interrupted aortic arch. In: Baue AE (ed). Glenn's Throracic and Cardiovascular Surgery. Connecticut: Appleton and Lange, 1996: 1243-69.
- Thompson CS, Ramaiah VG, Rodriguez-Lopez JA, Vranic M, Ravi R, DiMugno L, et al. Endoluminal stent graft repair of aortobronchial fistulas. J Vasc SURG 2002; 35: 387-91. [?zet]
- Kalkat MS, Bonser RS. Management of aortobronchial fistula following coarctation repair. Eur J Cardiothorac Surg 2003; 23: 116-8. [?zet] [Tam Metin] [PDF]
- Ala-Kulju K, Heikkinen L. Aneurysms after patch grat aortoplasty for the aorta: long-term results of surgical management. Ann Thorac Surg 1989; 47: 853-6. [?zet] [PDF]
- Knyshov GV, Sitar LL, Glagola MD, Atamanyuk MY. Aortic aneurysms at the site of the repair of coarctation of the aorta: a review of 48 patients. Ann Thorac Surg 1996; 61: 935-9. [?zet] [Tam Metin]
- Macintosh EL, Parrot JC, Unruh HW. Fistulas between the aorta and tracheobronchial tree. Ann Thorac Surg 1991; 51: 515-9. [?zet] [PDF]
- Posacioglu H, Apaydin AZ. Pseudoaneurysm and aortobronchial fistula after aortic coarctation repair by patch aortoplasty. Tex Heart Inst J 2004; 31: 319-21. [?zet] [Tam Metin] [PDF]
- Von Segesser LK, Tkebuchava T, Niederhauser U, K?nzli A, Lachat M, Genoni M, et al. Aortobronchial and aortoesophageal fistulae as risk factors in surgery of descending thoracic aortic aneurysms. Eur J Cardiothorac Surg 1997; 12: 195-201. [?zet] [PDF]
- Patel K, Ruttum DM, Olund TJ, Gandhi SD, Tisol WB, Nicolosi AC, et al. Sudden onset of sharp left-sided chest Pain and hemoptysis in a young man with a history of childhood aortic coarctation repair. J Cardiothorac Vasc Anesth 2009; 23: 256-8.
- Knyshov GV, Sitar LL, Glagoda MD, Atamanyuk MY. Aortic aneurysms at the site of repair of coarctation of the aorta: a review of 48 patients. Ann Thorac Surg 1996; 61: 935-9. [?zet] [Tam Metin]
Yaz??ma Adresi (Address for Correspondence):
Dr. Funda ULUORMAN,
Dokuz Eyl?l ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
35340, ?nciralt?
?ZM?R - TURKEY
e-mail: arslan_funda@mynet.com