T?rk sarkoidoz hastalar?nda ACE gen polimorfizmi ve sarkoidoz geli?me riski
Dilber YILMAZ1, Mutlu KARKUCAK2, Funda CO?KUN3, Tahsin YAKUT2, Esra KUNT UZASLAN3
1 ?orum G???s Hastal?klar? Hastanesi, G???s Hastal?klar? Klini?i, ?orum,
2 Uluda? ?niversitesi T?p Fak?ltesi, T?bbi Genetik Anabilim Dal?, Bursa,
3 Uluda? ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Bursa.
?ZET
T?rk sarkoidoz hastalar?nda ACE gen polimorfizmi ve sarkoidoz geli?me riski
Giri?: Sarkoidozun etyolojisi bilinmemektedir fakat farkl? etnik gruplar ve tek yumurta ikizlerindeki prevalans?, ailevi ?zelliklerine bak?ld???nda genetik predispozisyon olas? bir fakt?r olabilir. Sarkoidozun patofizyolojisinde anjiyotensin d?n??t?r?c? enzim (ACE) g?sterilmi?tir. Bu ara?t?rman?n amac?; ACE I/D (Insertion/Deletion) polimorfizminin sarkoidoz geli?imine olan etkisini ara?t?rmakt?r.
Hastalar ve Metod: ?al??mam?z 70 T?rk, histopatolojik olarak tan? konmu? sarkoidoz hastas? ve 69 sa?l?kl?, cinsiyet ve ya? a??s?ndan e?lenmi? kontrol i?eriyordu. ACE I/D polimorfizmini analiz etmek i?in polimeraz zincir reaksiyonu kullan?ld?. Agaroz jel elektroforezinde olu?an bantlara g?re genotip tayini yap?ld?. ?statistiksel analiz i?in ki-kare testi kullan?ld? ve anlaml?l?k de?eri p< 0.05 olarak kabul edildi.
Bulgular: Sarkoidoz grubunda D allelinin s?kl??? daha fazla olmas?na ra?men, D allelinin s?kl??? s?ras?yla sarkoidoz ve kontrol grubunda %67 ve %54 idi. Sarkoidoz ve kontrol grubu aras?nda I/I, I/D, D/D polimorfizmlerinin s?kl??? a??s?ndan anlaml? farkl?l?k saptanmad? (p> 0.05). Benzer olarak I/I, I/D, D/D polimorfizmlerinin s?kl??? a??s?ndan akci?er d??? organ tutulumu olan sarkoidoz hastalar?yla akci?er d??? organ tutulumu olmayan hastalar aras?nda farkl?l?k yoktu (p> 0.05).
Sonu?: Bizim bulgular?m?za g?re ACE gen polimorfizminin T?rk sarkoidoz hastalar?nda hastal???n geli?imine katk?s? sa?l?kl? kontrollerden farkl? de?ildi.
Anahtar Kelimeler: Sarkoidoz, polimorfizm, ACE geni.
SUMMARY
ACE gene I/D polymorphism and risk of sarcoidosis development in Turkish patients
Dilber YILMAZ1, Mutlu KARKUCAK2, Funda CO?KUN3, Tahsin YAKUT2, Esra KUNT UZASLAN3
1 Clinic of Chest Diseases, Corum Chest Diseases Hospital, Corum, Turkey,
2 Department of Medical Genetic, Faculty of Medicine, Uludag University, Bursa, Turkey,
3 Department of Chest Diseases, Faculty of Medicine, Uludag University, Bursa, Turkey.
Introduction: Etiology of sarcoidosis is unknown but the prevalence of disease in different ethnic groups and identical twins, family characteristics indicate that genetic predisposition is a possible factor. The angiotensin-converting enzyme (ACE) has been implicated in the pahophysiology of sarcoidosis. The aim of this study is to investigate the influence of a polymorphism in I/D (Insertion/Deletion) of the ACE gene on the susceptibility to sarcoidosis.
Patients and Methods: Our study included 70 Turkish patients who had histopathological diagnosis of sarcoidosis and 69 healthy age and sex matched control subjects. Polymerase chain reaction was used for analysing an I/D polymorphism in the gene coding for ACE. Genotyping was done according to bands that were formed on the agarose gel electrophoresis. Chi-square test was used for statistical analysis and p< 0.05 was accepted as significance.
Results: Although the D allele was more frequent in the sarcoidosis patients group, the frequency of the D allele was 67% and 54% respectively in the sarcoidosis and the control group. No significant difference in allele frequencies of I/I, I/D, D/D polymorphisms was observed between the sarcoidosis and control group (p> 0.05). Similarly allele frequencies of I/I, I/D, D/D polymorphisms was not different between sarcoidosis patients with extrapulmonary involvement and sarcoidosis patients without extrapulmonary involvement (p> 0.05).
Conclusion: Our findings have showed that contribution of ACE gene polymorphisms to susceptibility of disease development in Turkish sarcoidosis patients is not different from the healthy control subjects.
Key Words: Sarcoidosis, polymorphism, ACE gene.
Geli? Tarihi/Received: 23/04/2012 - Kabul Edili? Tarihi/Accepted: 16/07/2012
Introduction
Sarcoidosis is a chronic systemic granulomatous disease of unknown etiology characterized by accumulation of activated T-lymphocytes and mononuclear phagocytes forming non-caseating epitheloid granuloma in the affected organs (1,2). The recognition of race as an important risk factor clearly suggests a genetic predisposition to develop sarcoidosis. The underlying pathophysiology of the disorder could be explained as an antigen-driven process, which in genetically susceptible people leads to an exaggerated Th1 type immunological response (3).
One of the possible mechanisms is functional polymorphism of the angiotensin converting enzyme (ACE) gene. The ACE gene, located on chromosome 17q23, contains many polymorphisms. The insertion/deletion (I/D) polymorphism in intron 16 is the most studied polymorphism (4). The genotype is classified into three types: deletion homozygotes (D/D), insertion homozygotes (I/I) and heterozygotes (I/D). Serum ACE levels corresponding to ACE I/D genotypes in the order I/I < I/D < D/D encouraged investigating the influence of this variation on sarcoidosis susceptibility (5,6). Some studies have not found association between ACE I/D polymorphism and the incidence of sarcoidosis (4,7,8,9). By contrast D/D genotype conferred a threefold increased in risk for sarcoidosis in African-Americans though lack of association between ACE gene polymorphism and sarcoidosis in Caucasians in the same study (10). Also D allele is a possible risk factor for development of sarcoidosis in Japanese women (11). Additionally a striking over-representation of the D/D genotype in sarcoidosis patients and in unaffected relatives has established in Germans (12).
The aim of our study was to examine the distribution of the ACE I/D genotypes in Turkish patients with sarcoidosis and healthy controls to identify a whether it is genetic risk factor for sarcoidosis.
PATIENTS and METHODS
Study Subjects
Between September 2010 and December 2010, 70 sarcoidosis patients were enrolled from the outpatient clinic of Chest Diseases Department, Uludag University Medical Faculty. Diagnosis of sarcoidosis was based on histological evidence. Skin and lymph node involvement was attributed to sarcoidosis only if it was proven histologically. Spleen involvement was based on radiological findings. All patients had received the appropriate treatment for care of the disease. As a control group we studied 69 healthy age and sex matched subjects. All patients and control subjects were Turkish and unrelated to each other. All participated (patients and control subjects) in the study after they had given their full informed and written consent. The study was approved by the Ethics Committee of the Uludag University Medical School.
DNA Extraction and Genotyping
Blood samples were obtained in EDTA tubes both from the patients and controls. DNA was isolated according to the Dr. Zeydanl? (DZ) DNA isolation kit procedure and then stored at -20?C. The ACE gene I/D polymorphism was determined using the polymerase chain reaction (PCR) method. The primers used to determine ACE I/D polymorphism were F: 5'-CTG GAG ACC ACT CCC ATC CTT TCT 3' and R: 5' GAT GTG GCC ATC ACA TTC GTC AGA T-3', and the D/D genotype insertion area specific primer: F: 5'-TGG GAC CAC AGC GCC CGC CCG CCA CTA C-3' and R: 5'-TCG CCA GCC CTC CCA TGC CCA TAA-3'. To prevent incorrect D/D genotyping in samples of ACE D/D genotype, the results were confirmed with a second PCR analysis. PCR conditions were as follows: after the first denaturation for 5 min at 94?C, denaturation continued for 1 min at 94?C, which continued with 35 cycles of annealing for 1 min at 57?C (for verification of D/D genotype, at 63?C), and extension for 1 min at 72?C, which ended with final extension for 10 min at 72?C (13).
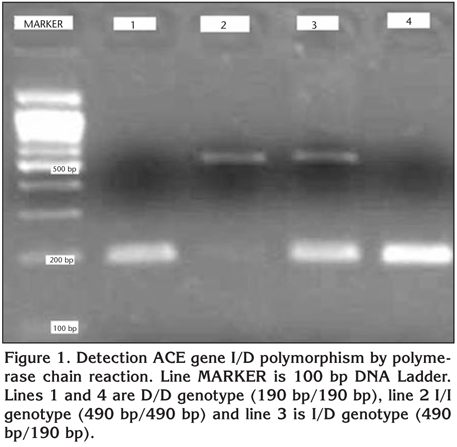
After PCR, the samples were separated by 2% agarose gel electrophoresis, stained with ethidium bromide and photographed for the amplification study. As a result of the amplification study, the agarose gel showed an amplification band of 190 bp in samples with the DD genotype, bands of 490 and 190 bp in samples with the ID genotype and a band of 490 bp in samples with the II genotype (Figure 1). In the second PCR analysis conducted for DD confirmation, an amplification band of 335 bp was observed with samples that had the insertion band.
Statistical Analysis
The SPSS 13.0 program was used for the analysis. All data were reported in terms of mean ? standard deviation (SD). A chi-squared test was used to compare genotypes and also genotypes/extrapulmonary involvement. P value less than 0.05 was accepted as statistical significance.
Results
The mean age was 46.64 ? 10.5 years and 44.86 ? 10.83 for the patient group (15 males and 55 females) and the control group (24 males and 45 females) respectively. There was no significant difference in terms of age and gender between the two groups (Table 1). Nine patients had skin involvement, one patient had lymph node involvement and one patient had spleen involvement.
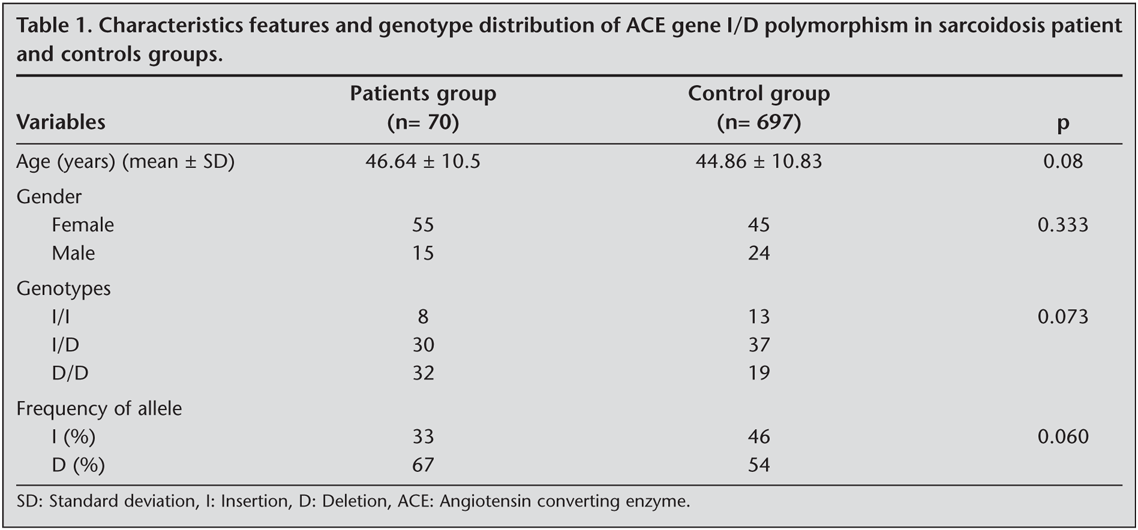
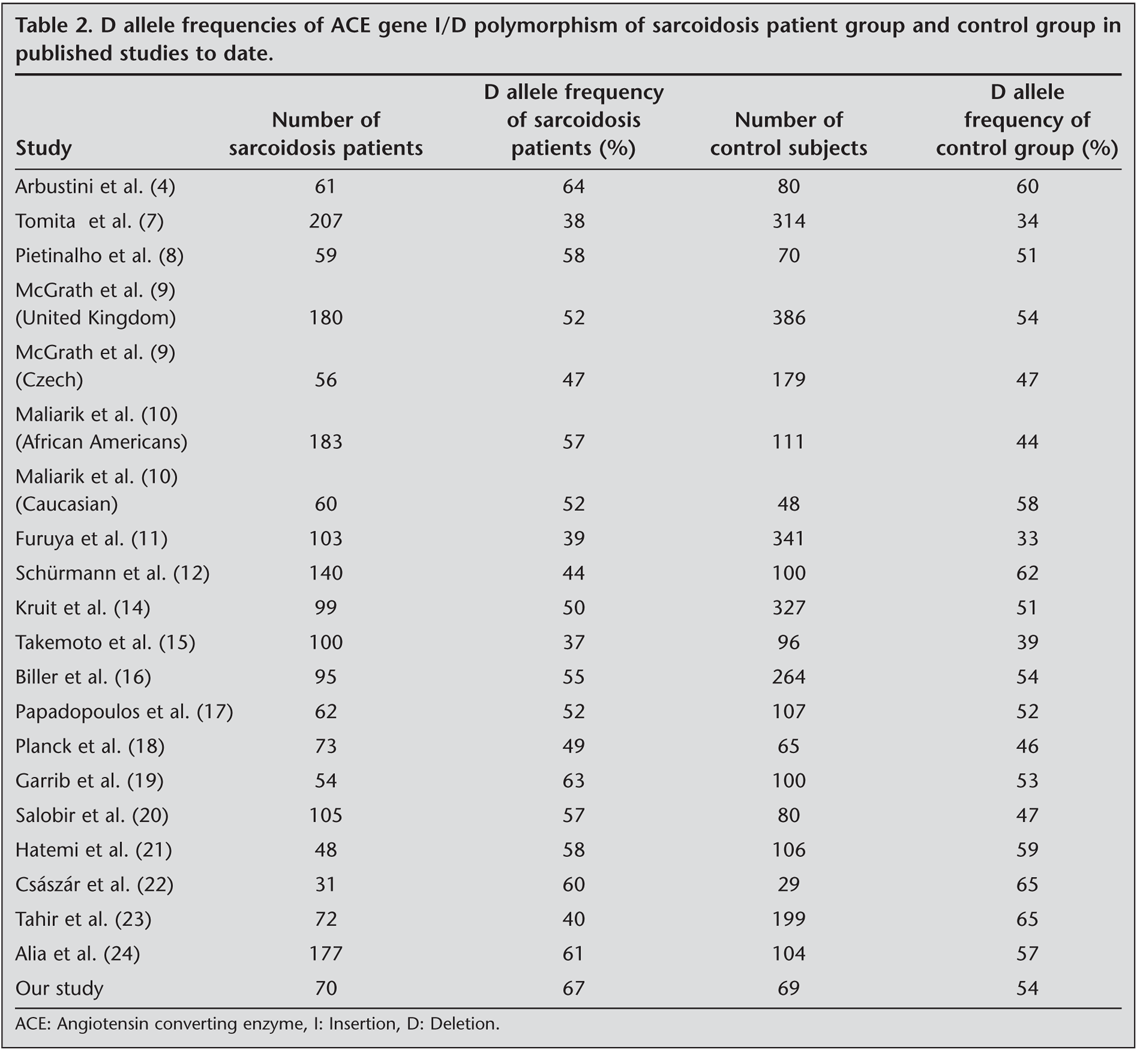
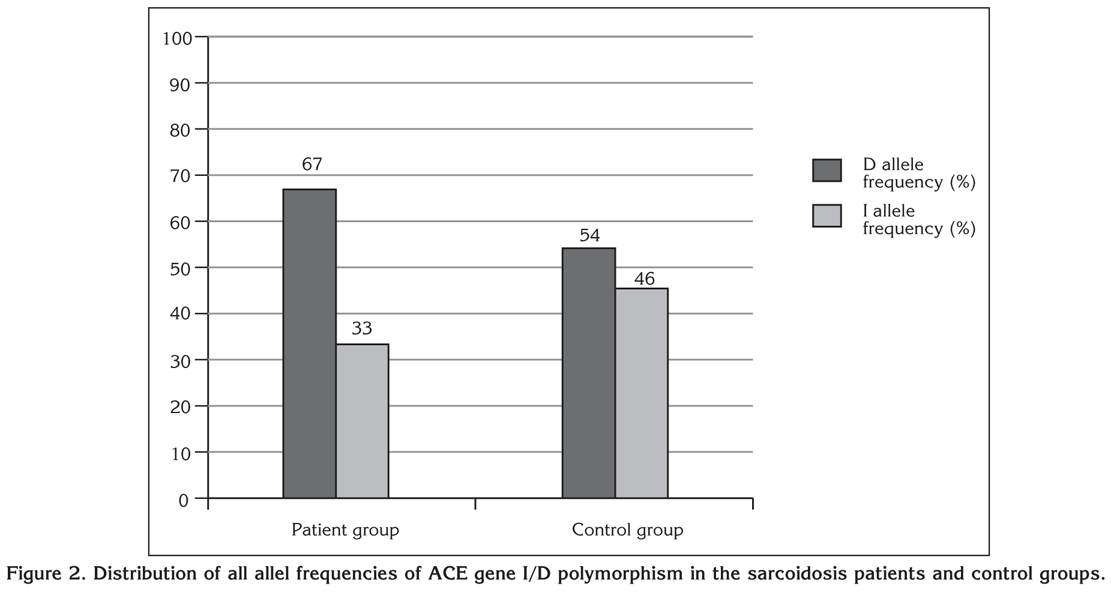
Characteristics and genotype distributions of ACE gene I/D polymorphism for both groups are tabulated (Table 1). No significant difference in allele frequencies for all polymorphisms was observed between sarcoidosis and control groups, although the D allele was more frequent in the sarcoidosis group (p> 0.05) (Table 1, Figure 2). The D allele frequencies of ACE gene I/D polymorphism in sarcoidosis in published studies before are summarized (Table 2). Out of nine patients with skin involvement, three patients had D/D, four patients had I/D and two patients had I/I allele. One patient with spleen involvement had I/D allele and one patient with lymph node involvement had I/D allele. Similarly there was not significant difference between sarcoidosis patients with extrapulmonary involvement and sarcoidosis patients without extrapulmonary involvement in terms of D/D, I/D and I/I allele frequencies (p> 0.05). Further analysis showed that also ACE genotype was not associated with skin involvement. However due to low numbers of sarcoidosis patients with extrapulmonary involvement, we can not exclude type II error.
Discussion
The discovery that an I/D polymorphism in intron 16 of the ACE gene contributes to the ACE activity in a healthy population was soon followed by studies of the role for this polymorphism in sarcoidosis patients (14). The D allele is reported to be a predisposing factor to high serum ACE levels both in normal subjects and in patients with sarcoidosis (15).
We have reported that there is no association between ACE gene I/D gene polymorphism and risk of sarcoidosis in Turkish people based on our prospective study. Although frequency of D allele was higher in the sarcoidosis patients group, significant difference was not observed between the D allele frequencies of two groups.
Many studies have investigated the relationship between ACE gene I/D polymorphism and sarcoidosis to date. As a result these studies have showed that frequency of genotypes can be different according to the population (4,7,8,9,10,11,12,14,15,16,17,18,19,20,21,22,23,24). While Biller et al. studied ACE gene I/D polymorphism in Caucasian sarcoidosis patients from Northern Germany, Tomita et al. studied patients from Japan (7,16). In both reports, distribution of ACE genotypes of patients with sarcoidosis and healthy controls were not different. Similar results were found among United Kingdom, Czech, Scandinavian and Caucasian sarcoidosis patients in Sweden (9,17,18). Arbustini et al. analyzed ACE genotyping of Italian Caucasian population and Garrib et al. analyzed the genotyping of Caucasian patients in United Kingdom (4,19). In the both studies, D/D was the most frequent genotype observed but this difference did not attain statistical significance. Similarly, Pietinalho et al. analyzed ACE gene I/D polymorphism in Finnish population (8). Although the frequency of the D allele was higher in control subjects and sarcoidosis patients, the difference was not statistically significant. However, Furuya et al. found an over-represantation of the allele D in Japanese sarcoidosis patients as compared with Japanese control (11). While this phenomenon was significant in female, there was no clear difference in male patients. Maliarik et al. studied African Americans and Caucasians (10). There was not significant difference in the distribution of ACE I/D genotypes in Caucasian cases and controls. But they found a three fold increase in sarcoidosis risk in African Americans with the D/D genotype. Additionally in the former population D/D genotype showed a marked increase in risk for cases with a positive family history compared with those who had a negative family history. Sch?rmann et al. studied German families with more than one member suffering from sarcoidosis (12). There was a striking over-representation of the D/D genotype in patients with sarcoidosis and their families compared to controls. Also Salobir et al. evaluated Slovenian sarcoidosis patients (20). In the sarcoidosis patient group a higher frequency of the D allele was detected, while in the control group the D allele frequency was lower. So ACE gene I/D polymorphism in Slovenian sarcoidosis patients, an increased risk of the disease susceptibility was demonstrated in homozygous carriers of the D allele. Hatemi et al. studied the ACE I/D gene polymorphism in 48 Turkish sarcoidosis patients (21). As a result frequency distribution was not different in patients and healthy control subjects. Frequency of D allele in our study was higher compared to Hatemi et al. (67% and 58%, respectively) (21). Additionally the number of sarcoidosis patients was much higher (70 and 48 respectively).
Data about extrathoracic involvement of sarcoidosis and ACE gene polymorphism is very limited in literature. Maliarik et al. showed that ACE genotype was not associated with extrathoracic involvement in sarcoidosis patients (10). Similarly we did not find any association between ACE gene polymorphism and extrathoracic involvement. But number of patients with extrapulmonary involvement so we could not exclude type II error.
In conclusion, while our study did not find a significant correlation between the ACE gene I/D polymorphism and sarcoidosis in Turkish population, we believe that a larger sample size and further elucidation of other single nucleotide polymorphisms are required to reach a definitive conclusion.
CONFLICT of INTEREST
None declared.
REFERENCES
- Medica I, Kastrin A, Maver A, Peterlin B. Role of genetic polymorphisms in ACE and TNF-alpha gene in sarcoidosis: a meta-analysis. J Hum Genet 2007; 52: 836-47. [?zet]
- Al-Khouzaie TH, Al-Tawfiq JA, Al Subhi FM. Sarcoidosis in the eastern region of Saudi Arabia. Ann Thorac Med 2011; 6: 22-4. [?zet] [Tam Metin]
- Costabel U, Hunninghake GW. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis Statement Committee. American Thoracic Society. European Respiratory Society. World Association of Sarcoidosis and other Granulomatous Disorders. Eur Respir J 1999; 14: 735-7. [PDF]
- Arbustini E, Grasso M, Leo G, Tinelli C, Fasani R, Diegoli M, et al. Polymorphism of angiotensin-converting enzyme gene in sarcoidosis. Am J Respir Crit Care Med 1996; 153: 851-4. [?zet]
- Rigat B, Hubert C, Gelas FA, Cambien F, Corvol P, Soubrier F. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Invest 1990; 86: 1343-6. [?zet] [PDF]
- Hubert C, Houot AM, Corvol P, Soubrier F. Structure of the angiotensin I-converting enzyme gene. J Biol Chem 1991; 266: 15377-83. [?zet] [PDF]
- Tomita H, Ina Y, Sugiura Y, Sato S, Kawaguchi H, Morishita M, et al. Polymorphism in the angiotensin-converting enzyme (ACE) gene and sarcoidosis. Am J Respir Crit Care Med 1997; 156: 255-9. [?zet] [Tam Metin] [PDF]
- Pietinalho A, Furuya K, Yamaguchi E, Kawakami Y, Selroos O. The angiotensin-converting enzyme DD gene is associated with poor prognosis in Finnish sarcoidosis patients. Eur Respir J 1999; 13: 723-6. [?zet] [PDF]
- McGrath DS, Foley PJ, Petrek M, Izakovicova-Holla L, Kolek V, Veeraraghavan S, et al. ACE gene I/D polymorphism and sarcoidosis pulmonary disease severity. Am J Respir Crit Care Med 2001; 164: 197-201. [?zet] [Tam Metin] [PDF]
- Maliarik MJ, Rybicki BA, Malvitz E, Sheffer RG, Major M, Popovich J Jr, et al. Angiotensin-converting enzyme gene polymorphism and risk of sarcoidosis. Am J Respir Crit Care Med 1998; 158: 1566-70. [?zet] [Tam Metin] [PDF]
- Furuya K, Yamaguchi E, Itoh A, Hizawa N, Ohnuma N, Kojima J, et al. Deletion polymorphism in the angiotensin converting enzyme (ACE) gene as a genetic risk factor for sarcoidosis. Thorax 1996; 51: 777-80. [?zet] [PDF]
- Sch?rmann M, Reichel P, M?ller-Myhsok B, Dieringer T, Wurm K, Schlaak M, et al. Angiotensin-converting enzyme (ACE) gene polymorphisms and familial occurrence of sarcoidosis. J Intern Med 2001; 249: 77-83. [?zet]
- Yakut T, Karkucak M, Ursavas A, Gulten T, Burgazlioglu B, Gorukmez O, et al. Lack of association of ACE gene I/D polymorphism with obstructive sleep apnea syndrome in Turkish patients. Genet Mol Res 2010; 9: 734-8. [?zet]
- Kruit A, Ruven HJ, Grutters JC, van den Bosch JM. Angiotensin II receptor type 1 1166 A/C and angiotensin converting enzyme I/D gene polymorphisms in a Dutch sarcoidosis cohort. Sarcoidosis Vasc Diffuse Lung Dis 2010; 27: 147-52. [?zet]
- Takemoto Y, Sakatani M, Takami S, Tachibana T, Higaki J, Ogihara T, et al. Association between angiotensin II receptor gene polymorphism and serum angiotensin converting enzyme (SACE) activity in patients with sarcoidosis. Thorax 1998; 53: 459-62. [?zet] [PDF]
- Biller H, Ruprecht B, Gaede KI, M?ller-Quernheim J, Zissel G. Gene polymorphisms of ACE and the angiotensin receptor AT2R1 influence serum ACE levels in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis 2009; 26: 139-46. [?zet]
- Papadopoulos KI, Melander O, Orho-Melander M, Groop LC, Carlsson M, Hallengren B. Angiotensin converting enzyme (ACE) gene polymorphism in sarcoidosis in relation to associated autoimmune diseases. J Intern Med 2000; 247: 71-7. [?zet] [Tam Metin] [PDF]
- Planck A, Eklund A, Yamaguchi E, Grunewald J. Angiotensin-converting enzyme gene polymorphism in relation to HLA-DR in sarcoidosis. J Intern Med 2002; 251: 217-22. [?zet] [Tam Metin] [PDF]
- Garrib A, Zhou W, Sherwood R, Peters TJ. Angiotensin converting enzyme (ACE) gene polymorphism in patients with sarcoidosis. Biochem Soc Trans 1998; 26: 137.
- Salobir B, Medica I, Tercelj M, Kastrin A, Sabovic M, Peterlin B. Association of angiotensin-converting enzyme/DD genotype with sarcoidosis susceptibility in Slovenian patients. Med Sci Monit 2007; 13: 538-42. [?zet]
- Hatemi AC, Cine N, Tabak L, Kiyan E, Erelel M, Cuhadaroglu C, et al. Angiotensin converting enzyme 1 Gene Insertion/Deletion polymorphism in patients with sarcoidosis. Turkish Respiratory Journal 2001; 2: 35-8. [?zet] [Tam Metin] [PDF]
- Cs?sz?r A, Halmos B, Palicz T, Szalai C, Romics L. Interpopulation effect of ACE I/D polymorphism on serum concentration of ACE in diagnosis of sarcoidosis. Lancet 1997; 350: 518.
- Tahir M, Sharma SK, Ashraf S, Mishra HK. Angiotensin converting enzyme genotype affects development and course of sarcoidosis in Asian Indians. Sarcoidosis Vasc Diffuse Lung Dis 2007; 24: 106-12. [?zet]
- Al?a P, Ma?? J, Capdevila O, Alvarez A, Navarro MA. Association between ACE gene I/D polymorphism and clinical presentation and prognosis of sarcoidosis. Scand J Clin Lab Invest 2005; 65: 691-7. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Dilber YILMAZ,
Ba?larba?? Mahallesi, Bozcaada Sokak
No: 17 Osmangazi,
BURSA - TURKEY
e-mail: drdilberyilmaz@gmail.com