Successfully treated eosinophilic pneumonia in an octogenarian
Koichi
KURISHIMA, Katsunori KAGOHASHI, Gen OHARA, Tomohiro TAMURA,
Mio KAWAGUCHI, Hiroaki SATOH
Tsukuba ?niversitesi Mito T?p Merkezi, ?? Hastal?klar?, Mito, Ibaraki, Japonya.
We report a case of an acute exacerbation of eosinophilic pneumonia (EP) in an octogenarian that was successfully treated with urgent medical management.
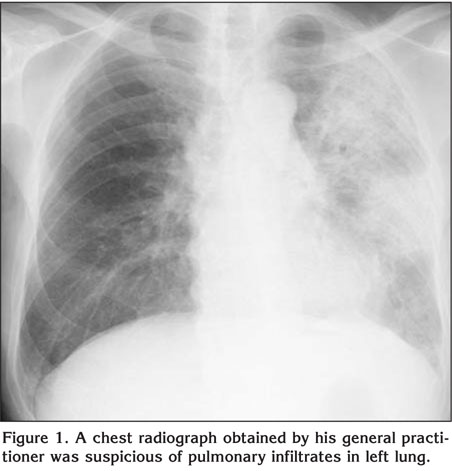
An 83-year-old man presented with a 10-day history of non-productive cough, fever, and general fatigue. The patient smoked for 67 year one pack a day but he was not exposed to toxins, tropical diseases and legal or illegal drugs. A chest radiograph obtained by his general practitioner was suspicious of pulmonary infiltrates in left lung (Figure 1). The physical examination was unremarkable. No lymphadenopathy was present. Laboratory data were remarkable for white cell count of 16.4 x 109/L with 18% eosinophils. No biliary parasite was identified by sonography. Egg of parasite was not found in the stools and serological tests were negative for parasites. The chest computerized tomography scan on showed a consolidation in upper and lower lobes of the left lung. The distribution of the infiltrates was nonsegmental. All tests for acid-fast bacilli including culture were negative. Serologic and microscopic testing for fungi was negative. Cytoplasmic and perinuclear antineutrophil antibodies were unremarkable. A bronchoalveolar lavage obtained from the left upper lobe showed total cell count 2.9 x 105/mL with 43% eosinophils; no pathogenic organism was found. Taken these results together, the diagnosis of EP was confirmed. The patient was started on 40 mg prednisolone per day. During the next 24 h he improved dramatically. After two weeks of treatment all laboratory tests and pulmonary infiltrates had normalized. He was successfully weaned off the prednisolone over a period of five months.
We present an octogenarian who was successfully treated for an acute exacerbation of EP. EP is a slowly progressive diffuse lung disease and known to be exacerbated by acute upper respiratory tract infection or heart failure in some instances. It can easily progress to acute respiratory distress syndrome-like condition, which is extremely difficult to manage. Corticosteroid therapy in older people can be associated with complications such as infection, worsening of diabetes, mineral imbalance, myopathy and psychosis. Complication from mechanical ventilation such as pneumothorax or ventilator-associated pneumonia might also occur more often in older people and we sometimes encounter the situation of being unable to extubate the patient. There have been only five octogenarians in four previous reports of successfully treated acute exacerbation of EP (1,2,3,4). Their report and our experience imply that an exacerbation of EP even in the oldest old is treatable. In four of them, EP developed by drugs such as daptomycin and mexiletine (2,3,4). In our patient, there was no medical history as for taking drugs related to developing of EP, and we suppose that preceding upper respiratory infection might be related to development of EP.
Although very rare, clinicians should be considered a possibility of EP when we observe diffuse infiltrates in peripheral lung zone. Although there was no eospinophilia in peripheral blood, bronchoalveolar lavage may sometimes be very important to establish correct diagnosis. If there is no contraindication, we would not hesitate the procedure even in the elderly.
CONFLICT of INTEREST
None declared.
Geli? Tarihi/Received: 28/11/2011 - Kabul Edili? Tarihi/Accepted: 05/12/2011
REFERENCES
- Michels G, Koch A, Kochanek M, Kvasnicka HM. 82-year-old patient with chronic cough, pulmonary infiltrations and eosinophilia. Dtsch Med Wochenschr 2010; 135: 2133-4.
-
Miller BA, Gray A, Leblanc TW, Sexton DJ, Martin AR, Slama TG. Acute eosinophilic
pneumonia secondary to daptomycin: a report of three cases. Clin Infect Dis
2010; 50: e63-8.
[?zet] [Tam Metin] [PDF] -
Lal Y, Assimacopoulos AP. Two cases of daptomycin-induced eosinophilic pneumonia
and chronic pneumonitis. Clin Infect Dis 2010; 50: 737-40.
[?zet] [Tam Metin] [PDF] -
Lee SP, Kim SH, Kim TH, Sohn JW, Shin DH, Park SS, et al. A case of
mexiletine-induced hypersensitivity syndrome presenting as eosinophilic
pneumonia. J Korean Med Sci 2010; 25: 148-51.
[?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Hiroaki SATOH,
Division of Internal Medicine,
Mito Medical Center, University of Tsukuba,
Miya-machi 3-2-7, Mito, 310-0015 IBARAKI - JAPAN
e-mail: hirosato@md.tsukuba.ac.jp