T?berk?loz ve meslek: T?berk?lozlu hastalarda tan?mlay?c? ?al??ma
Aylin
BABALIK1, Nadi BAKIRCI2, Korkmaz ORUC1, ?ule
KIZILTA?1, G?lg?n ?ET?NTA?1,
Sinem ALTUNBEY1, Haluk C. ?ALI?IR1
1 SB S?reyyapa?a G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi,
G???s Hastal?klar? Klini?i, ?stanbul,
2 Ac?badem ?niversitesi T?p Fak?ltesi, Halk Sa?l??? Anabilim Dal?, ?stanbul.
?ZET
T?berk?loz ve meslek: T?berk?lozlu hastalarda tan?mlay?c? ?al??ma
Giri?:Bu ?al??ma, T?rkiye'de t?berk?loz hastalar?n?n mesle?e g?re da??l?m?n? incelemek amac?yla tasarlanm??t?r.
Hastalar ve Metod: Bu retrospektif tan?mlay?c? ?al??maya, bakteriyolojik ve histopatolojik olarak kan?tlanm?? t?berk?lozu olup, t?berk?loz tedavisi almakta olan toplam 757 hasta dahil edildi. 2004-2007 y?llar? aras?nda SB S?reyyapa?a G???s Hastal?klar? veG???s Cerrahisi E?itim ve Ara?t?rma Hastanesine ba?vuran hastalar?n kay?tlar?, hastalar?n demografik ?zellikleri ve meslekleri a??s?ndan incelendi. Meslekler Uluslararas? Standart Meslek S?n?fland?rmas? [International Standardization Classification Occupation (ISCO-88)] listesine uygun ?ekilde 10 grupta topland?.
Bulgular: ?al??ma pop?lasyonunun %67'si erkek, ortalama ya? (SS) 41.3 (16.4) y?l idi. S?ras?yla hastalar?n %81 ve %19'u rek?rren ve yeni tan? t?berk?loz hastalar? idi. En s?k kar??la??lan meslek gruplar?; sanatkarlar ve ilgili i?lerde ?al??anlar (%32), tesis ve makine operat?rleri ve montajc?lar (%10), alt gruplar ise tekstil ve giyim e?yas? ile ilgili i?lerde ?al??anlar (%12.9), araba, kamyonet ve motosiklet s?r?c?leri (%5.8) idi. En pop?ler alt gruplar aras?nda en gen? olan?, 29.5 (11.1) y?l ortalama ya? (SS) ile tekstil ve giyim e?yas?yla ilgili i?lerde ?al??anlar iken, madencilik ve in?aat sekt?rlerinde nitelik gerektirmeyen i?lerde ?al??anlar en ya?l? alt gruptu [ortalama ya? (SS) 63.9 (7.9) y?l]. T?m meslek gruplar?nda, erkeklerin oran? kad?nlardan daha fazlayd?. Kad?n hastalar aras?nda en s?k g?r?len meslek alt grubu tekstil ve giyim e?yas?yla ilgili i?lerde ?al??anlar iken, madencilik ve in?aat sekt?rlerinde nitelik gerektirmeyen i?lerde ?al??anlar, araba, kamyonet ve motosiklet s?r?c?leri, in?aat? tamamlay?c? i?ler ve benzer i?lerde ?al??an sanatkarlar tamamen erkeklerden olu?mu?tu. T?m meslek alt gruplar? da yeni tan? alm?? hasta say?s? rek?rren hastalardan anlaml? derecede fazla idi.
Sonu?: ?zellikle tekstil end?strisinde, i? ortamlar?n?n ko?ullar?n?n iyile?tirilmesinin, yani uygun havaland?rma, uygun ya?am alanlar? ve ?al??anlar?n rutin sa?l?k kontrollerinin sa?lanmas?yla daha sa?l?kl? ko?ullar olu?turulmas?n?n hayati ?neme sahip oldu?u g?r?lmektedir.
Anahtar Kelimeler: Meslek, t?berk?loz, T?rkiye.
SUMMARY
Occupation and tuberculosis: a descriptive study in Turkish patients with tuberculosis
Aylin
BABALIK1, Nadi BAKIRCI2, Korkmaz ORUC1, ?ule
KIZILTA?1, G?lg?n ?ET?NTA?1,
Sinem ALTUNBEY1, Haluk C. ?ALI?IR1
1 Clinic of Chest Diseases, Sureyyapasa Chest Diseases and Chest Surgery Training and
Research Hospital, Istanbul, Turkey,
2 Department of Public Health, Faculty of Medicine, Acibadem University, Istanbul, Turkey.
Introduction: The present study was designed to determine the distribution of tuberculosis patients according to their occupations in Turkey.
Patients and Methods: A total of 757 patients with bacteriologically and histopathologically confirmed diagnosis of tuberculosis and under the tuberculosis treatment were included in this retrospective descriptive study. Medical records of patients admitted to the Ministry of Health Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital between the years of 2004 and 2007 were evaluated in terms of patient demographics and the occupations. Occupations were classified into 10 groups according to the International Standardization Classification Occupation (ISCO-88).
Results: Males composed 67% of the overall population [mean age (SD) was 41.3 (16.4) years]. Recurrent and newly diagnosed tuberculosis patients composed 81 and 19% of the patients, respectively. The most frequently identified major occupational groups were; craft and related workers (32%), plant and machine operators and assembler (10%), followed by the subgroups of textile, garment and related trades workers (12.9%), motor vehicle drivers (5.8%). The youngest subgroup among the most popular subgroups with a mean age (SD) of 29.5 (11.1) years, was textile, garment and related trades workers while the subgroup of mining and construction laborers was the oldest with a mean age (SD) of 63.9 (7.9) years. In all occupational subgroups, the frequency of males was higher than females. In female patients, the most frequently identified subgroup was, textile, garment and related trades workers while, mining and construction laborers, motor vehicle drives, building frame and related trades workers were composed solely of males. The frequency of newly diagnosed patients was significantly higher than former tuberculosis patients in the occupational subgroups.
Conclusion: It seems crucial to improve conditions of workplaces with arrangements enabling healthier environment such as adequate ventilation, appropriate living space as well as routine health controls of employees especially for the textile industry.
Key Words: Occupation, tuberculosis, Turkey.
Geli? Tarihi/Received: 12/10/2011 - Kabul Edili? Tarihi/Accepted: 15/12/2011
INTRODUCTION
Tuberculosis is a chronic pulmonary disease associated with high morbidity and mortality. The estimates of the global burden of disease caused by tuberculosis in 2009 include 9.4 million incident cases and 14 million prevalent cases with 1.3 million deaths among human immunodeficiency virus (HIV)-negative people and 0.38 million deaths among HIV-positives (1).
According to the data from the Ministry of Health, 18452 cases have been diagnosed with tuberculosis in Turkey in 2008 and 90.8% (16.760 patients) were the newly diagnosed cases. The rate of patients with past history of tuberculosis treatment was 9.2% (1692 patients) (2).
Exposure to a potentially infectious case is a prerequisite for becoming infected while the risk of becoming infected, the probability that an infected individual will develop tuberculosis, and the probability that a diseased individual will die from tuberculosis depend on certain risk factors (3).
The major factors that determine the risk of becoming exposed to tubercle bacilli include the number of incident infectious cases in the community, the duration of their infectiousness, and the number and nature of interactions between a case and a susceptible contact per unit of time of infectiousness (3).
Certain conditions have been considered to impair the host defense against infection and lead to progression to disease such as HIV infection, malnutrition, tobacco smoke, indoor air pollution caused by the burning of solid fuels, alcoholism, diabetes, silicosis, malignancies and immunosuppressive treatment (3,4).
Although it has been reported that some workplaces may create higher risk for tuberculosis due to local environmental conditions and certain occupations pose a high risk for the tuberculosis development, the data on occupational risk for tuberculosis are limited apart from studies conducted with health care workers and miners (5,6,7,8,9).
Based on inclusion of patients from various occupational settings in our hospital which was run by The Ministry of Labor previously, the present study was designed to perform a descriptive analysis of occupations of tuberculosis patients admitted to our hospital.
PATIENTS and Methods
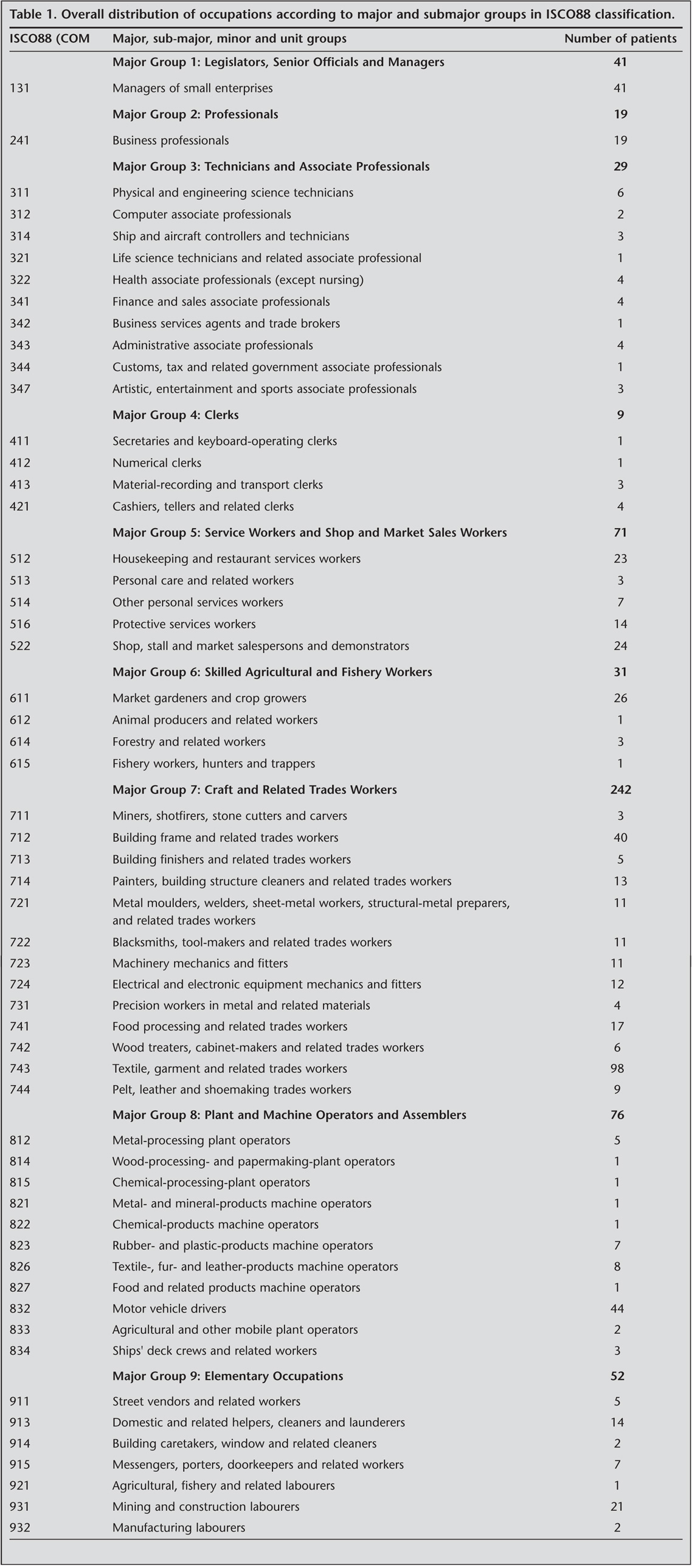
A total of 757 newly diagnosed and former patients with bacteriological and histopathological confirmation of tuberculosis diagnosis were included in this retrospective descriptive study. Medical records of patients admitting to Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital from 2004 to 2007 were evaluated in terms of patient demographics, past history of tuberculosis treatment and the occupational distribution. Occupations were classified into 10 groups according to International Standardization Classification Occupation (ISCO-88) (Table 1).
Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital is a tertiary care hospital giving service to tuberculosis patients hospitalized according to certain criteria including:
a. Patients requiring clinical follow up for diseases concomitant to tuberculosis,
b. Patients with diffuse lung tuberculosis requiring support therapy additional to anti-tuberculosis treatment,
c. Patients who were unable to be identified with ARB positivity at secondary care centers, tuberculosis dispensaries and outpatient clinics of our hospital,
d. Patients with drug related adverse events, hepatotoxicity in particular,
e. Former tuberculosis patients and patients with HR resistance according to drug resistance tests.
Statistical Analysis
Descriptive Statistics were used. Continuous variables will be summarized using mean and standard deviation (SD) (for normally distributed variables) and median and quartiles (for non-normally distributed variables). Categorical variables will be summarized with percent in each category.
Results
Mean age (SD) of overall population was 38.7 (16.7) years and 51% of patients was at 15-35 years of age, while 49% was older than 35 years of age. Males composed 67% of population [mean age (SD) was 41.3 (16.4) years] and 33% of patients were females [mean age (SD) was 33.6 (16.4) years]. Former and newly diagnosed tuberculosis patients composed 81 and 19% of population, respectively.
Overall distribution of occupations according to major and submajor groups in ISCO88 classification is summarized in Table 1.
Out of 187 (24.7%), 143 (18.9%) of them were housewives, 44 (5.8%) of them were students. The remaining 570 (75.3%) patients were classified according to ISCO 88's ten major occupational groups and 57 subgroups. Considering 10 major occupational groups, the most frequently identified groups were "craft and related workers" (32%), "plant and machine operators and assembler" (10%), "service workers and shop and market sales workers" (9.4%) (Table 2).
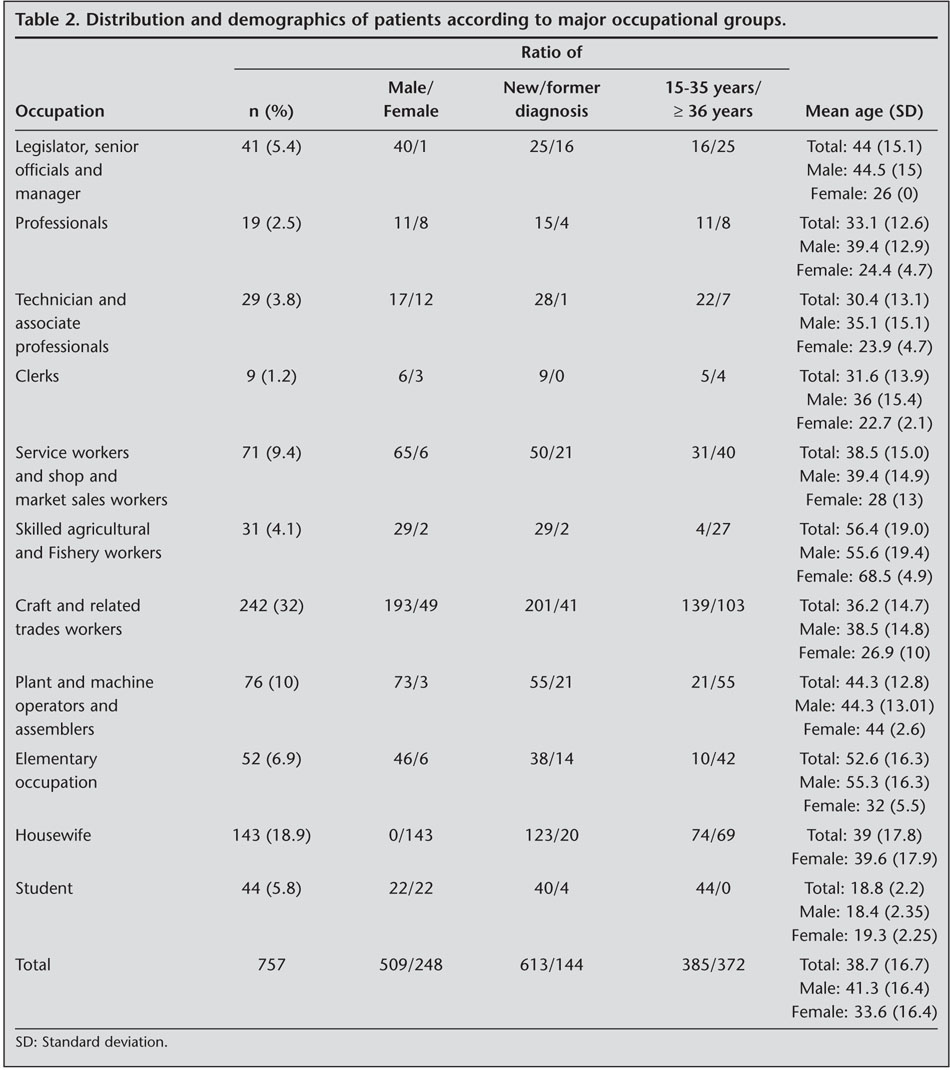
In 10 major occupational groups, patients identified to be employed as "skilled agricultural and fishery worker" [mean age (SD): 56.4 (19.0) years], "elementary occupation" [mean age (SD): 52.6 (16.3) years], "legislator, senior officials and manager" [mean (SD): 44.4 (15.1) years], "plant and machine operators and assemblers" [mean age (SD): 44.3 (12.8) years], and "service workers and shop and market sales workers" [mean age (SD): 38.5 (15.0) years] were older than the patients included in other major occupational groups (Table 2).
Additionally, there was significantly higher number of males in 10 major occupational groups compared with females, while the number of newly diagnosed tuberculosis patients was also higher than the former tuberculosis patients. Among female patients the most frequently identified major occupational group was "craft and related trades workers" (Table 2).
Considering 57 subgroups of occupational classification, the most frequently identified subgroups were "textile, garmet and related trades workers" (98; 12.9%), "motor vehicle drivers" (44; 5.8%), "manages of small enterpries" (41; 5.4%), "building frame and related trateds workers" (40; 5.3%), "market gardeners and crop growers (26; 3.4%), housekeeping and restaurant services workers (24; 3.2%), mining and construction laborers (21; 2.8%) (Table 3).
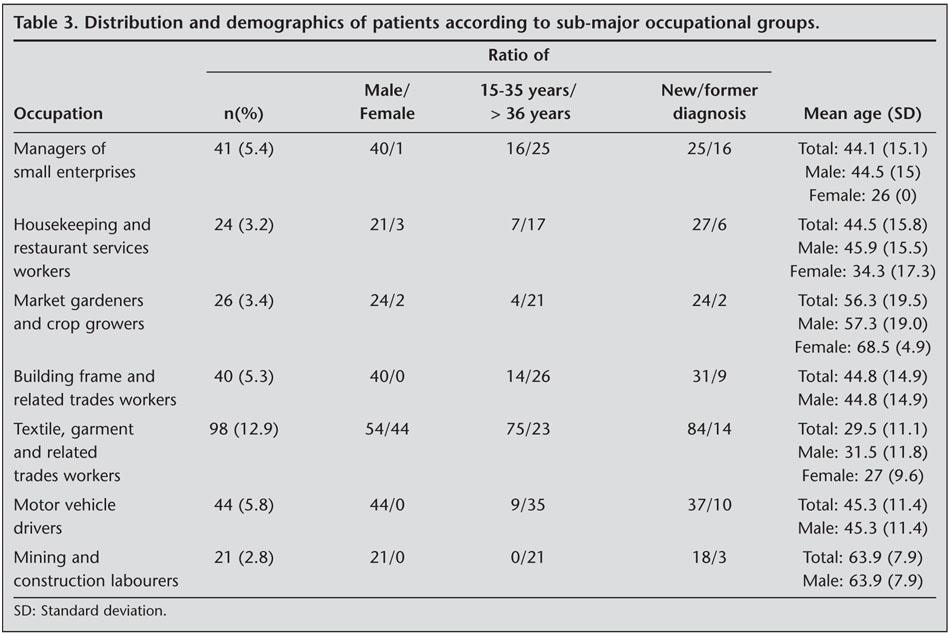
The youngest subgroup among the most popular subgroups was "textile, garment and related trades workers" [mean age (SD): 29.5 (11.1) years]. In the other subgroups, the percentage of patients over 35 years of age was higher than younger patients (Table 3).
The subgroups including oldest patients were "mining and construction laborers" [mean age (SD): 63.9 (7.9) years] and "market gardeners and crop growers" [mean age: (SD) 56.3 (19.5) years] (Table 3).
In all most popular occupational subgroups, the frequency of males was higher than females. In female patients, the most frequently identified subgroup was "textile, garment and related trades workers", while "mining and construction laborers", "motor vehicle drives", "building frame and related trades workers" were composed solely of males. The frequency of newly diagnosed patients was significantly higher than former tuberculosis patients in the occupational subgroups.
Discussion
Unfortunately, there is limited number of studies concerning the relation of tuberculosis as a significant socioeconomic public health issue to occupational and environmental factors. Tuberculosis cases are most commonly seen in people from lower socioeconomic levels while the workplace stands for the second order risk factor following household conditions. Accordingly, increase in disease prevalence has been expected in people employed in the workplaces lacking safety conditions as well as routine workplace examinations (10).
Tuberculosis has been considered as an important health issue among healthcare workers especially in low and middle-income countries (LMICs). When compared with general population, the risk attributable for tuberculosis was reported to be 25 to 5.361 per 100.000 per year amongst healthcare workers (5). Menzies et al. reviewed published literature regarding prevalence and incidence of tuberculosis infection and disease among HCWs in countries categorized by mean income and that stated that the median prevalence of latent tuberculosis infection (LTBI) in HCWs was 63% in LMICs and 24% in high income countries (HICs) (6). There are some studies in Turkey about HCW and tuberculosis. Relative Risk (RR) range was found for doctors (1.5-3.1), for nurses (1.5-6.7) and paramedics (1.5-3.9) (11,12,13).
Based on the consistently reported association between silicosis and tuberculosis rates for active tuberculosis in silicosis subjects was documented to be 2 to 30 fold when compared to the rate for the same workforce lacking silicosis. Exposure to silica, even without silicosis, may also predispose individuals to tuberculosis (9,14,15,16).
Bang et al. evaluated tuberculosis mortality by industry in the United States in 1990-1999. Industries and occupation involving potential contact with infected cases (e.g. health care workers), those with silica exposure and silicosis (e.g. mining and construction), and those associated with low socioeconomic status were identified to have significantly elevated tuberculosis mortality (17).
In our population, the most commonly identified major occupational group was "craft and related trades workers" (32.0%) of which "textile, garment and related trades workers" composed the 41%.
Past history of tuberculosis was reported to reach high prevalence rates in a past study investigating byssinosis prevalence in cotton textile industry workers in South Africa (18).
In retrospective analysis of 2774 people working in garment industry in Qatar, tuberculosis was determined to be positive in 43% based on identification of ≥ 15 mm tuberculin reaction (19).
A postal questionnaire study aiming to determine the incidence of pulmonary tuberculosis as well as the provision of health services in 557 industries located in the Western Cape, South Africa in 1987 revealed highest rates of tuberculosis in the textile, iron and steel industries whereas the lowest rates in the printing and paper industry, in trade and commerce, and in the transport sectors. Tuberculosis incidence was also reported to be varied by certain factors such as factory size, with the highest rates being reported in the smallest factories (20).
Tuberculosis was identified in 6% of cotton textile industry workers in Pakistan (21).
Latest data concerning incidence rate of tuberculosis with respect to age groups in Turkish tuberculosis patients revealed increase in the incidence starting from 15-24 years of age reaching its highest level at 55-64 years and beyond 65 years of age (2). While patients < 35 years and ≥ 35 years represented by similar numbers in our overall population composed of 757 patients, there was a significant age-dependent alteration in occupational groups. Accordingly, while textile, garment and related trades workers were younger [29.5 (11.1) years], mining and construction laborers [63.9 (7.9) years] as well as market gardeners and crop growers [56.3 (19.5) years] were identified to be composed of older people.
According to latest tuberculosis data from our country including 18.452 patients, the rate of newly diagnosed cases was reported to be 90.8% (16.760) while the frequency of patients with former anti-tuberculosis treatment was 9.2% (1692). In our study, newly diagnosed cases composed 81% of population while former tuberculosis patients were identified in 19%. Higher frequency of patients with past history of tuberculosis in our population might be related to working of our hospital as a reference hospital as well as priority given to patients with past tuberculosis treatment according to our hospitalization criteria.
Latest tuberculosis data from Turkey revealed male/female ratio of patients to be 1.6 (2). In our study, possibly in relation to higher numbers of hospital beds available for male patients in our hospital, this ratio was determined to be 2 (509/248). Indeed this also explains the identification of higher frequencies for male specific trade branches such as "building frame and related trades workers", "motor vehicle drivers" and "mining and construction laborers" in occupational distribution of our patients. Additionally, apart from identification of 58% of females to be housewives, the occupation most commonly associated with tuberculosis was textile industry among females.
According to our findings, textile industry workers who were significantly younger than other trade braches were identified to compose majority of our population. The higher incidence of tuberculosis in textile industry seems to be related to unfavorable workplace conditions causing working of patients in crowded small places with insufficient amount of ventilation and poor air condition.
In relation to inclusion of more frequent contact with other people, the second-most prevalent occupation among our tuberculosis patients was "motor vehicle drivers" who were also pose a significant risk for public contamination of the disease as carriers. In a study conducted by Horna-Campos et al., considering estimation of tuberculosis incidence rates in patients of a health micro-network, and the percentage of transport sector workers among tuberculosis and multi-drug-resistant tuberculosis (MDR-TB) patients, standardized incidence rates for transport sector workers were reported to be 2.7-4.5 times higher than those in the total working age male and global population of the micro-network studied. The association between tuberculosis and transport occupation and MDR-TB and transport occupation was documented to be high (OR: 3.06, 95% CI 2.2-4.2 and OR 3.14, 95% CI 1.1-1.9, respectively) (22). The later study showed an association between years of working and weekly work burden among minibus workers suggesting an occupational risk in service jobs in low-income countries with high tuberculosis prevalence (23).
Major limitation of the present study seems to be the exclusion of tuberculosis patients who do not meet the hospitalization criteria applied in our hospital which may consequently lead to inadequate representation of the overall cohort of tuberculosis patients across Turkey. Moreover, since there is no national database concerning distribution of insured and uninsured workers in different occupational groups, our study design included demonstration of descriptive data on occupational distribution of hospitalized tuberculosis patients in Turkey. Finally, based on retrospective design of the present study, only the latest occupation of patients was recorded to be included in corresponding analysis.
In conclusion, based on data concerning the relation of occupation and tuberculosis obtained from hospitalized tuberculosis patients in Turkey, it seems crucial to improve conditions of workplaces with arrangements enabling healthier environment such as adequate ventilation, appropriate living space as well as routine health controls of employees especially for the textile industry. Further analysis of the association between tuberculosis and the occupation in large scale studies is needed.
Acknowledgements
Authors would like to thank to KAPPA Training, Consultancy & Research Company for editing written article.
CONFLICT of INTEREST
None declared.
REFERENCES
- Global Tuberculosis Control. WHO Report 2010. WHO/HTM/TB/2010.7
- T.R. Ministry of Health, Department of Struggle Against Tuberculosis. The Struggle Against Tuberculosis in Turkey, 2010 report.
- Rieder HL. Epidemiologic basis of Tuberculosis control. International Union Against Tuberculosis and Lung Disease 68, Paris,1999.
- L?nnroth K, Holtz TH, Cobelens F, Chua J, van Leth F, Tupasi T, et al. Inclusion of information on risk factors, socio-economic status and health seeking in a tuberculosis prevalence survey. Int J Tuberc Lung Dis 2009; 13: 171-6. [?zet]
- Joshi R, Reingold AL, Menzies D, Pai M. Tuberculosis among health-care workers in low-and middle-income countries: a systematic review. PLoS Med 2006; 3: e494. [?zet] [Tam Metin] [PDF]
- Menzies D, Joshi R, Pai M. Risk of tuberculosis infection and disease associated with work in health care settings. Int J Tuberc Lung Dis 2007; 11: 593-605. [?zet]
- Seidler A, Nienhaus A, Diel R. Review of epidemiological studies on the occupational risk of tuberculosis in low-incidence areas. Respiration 2005; 72: 431-46. [?zet]
- Ross
MH, Murray J. Occupational respiratory disease in mining. Occup Med 2004; 54:
304-10.
[?zet] [PDF] - teWaternaude
JM, Ehrlich RI, Churchyard GJ, Pemba L, Dekker K, Vermeis M, et al.
Tuberculosis and silica exposure in South African gold miners. Occup Environ
Med 2006; 63: 187-92.
[?zet] [Tam Metin] [PDF] - Muniyandi M, Ramachandran R, Gopi PG, Chandrasekaran V, Subramani R, Sadacharam K, et al. The prevalence of tuberculosis in different economic strata: a community survey from South India. Int J Tuberc Lung Dis 2007; 11: 1042-5. [?zet]
- Hosoglu S, Tanrikulu AC, Dagli C, Akalin S. Tuberculosis among health care workers in a short working period. Am J Infect Control 2005; 33: 23-6. [?zet]
- Keskiner R, Erg?n?l O, Demiroglu Z, Eren S, Baykam N, Dokuzoguz B. Risk of tuberculous infection among healthcare workers in a tertiary-care hospital in Ankara, Turkey. Infect Control Hosp Epidemiol 2004; 25: 1067-71. [?zet]
- Kilinc O, Ucan ES, Cakan MD, Ellidokuz MD, Ozol MD, Sayiner A, et al. Risk of tuberculosis among healthcare workers: can tuberculosis be considered as an occupational disease? Respir Med 2002; 96: 506-10. [?zet]
- Cowie RL. The epidemiology of tuberculosis in gold miners with silicosis. Am J Respir Crit Care Med 1994; 150: 1460-2. [?zet]
- Hnizdo E, Murray J. Risk of pulmonary tuberculosis relative to silicosis and exposure to silica dust in South African gold miners. Occup Environ Med 1998; 55: 496-502. [?zet] [PDF]
- Girdler-Brown BV, White NW, Ehrlich RI, Churchyard GJ. The burden of silicosis, pulmonary tuberculosis and COPD among former Basotho goldminers. Am J Ind Med 2008; 51: 640-7. [?zet]
- Bang KM, Weissman DN, Wood JM, Attfield MD. Tuberculosis mortality by industry in the United States, 1990-1999. Int J Tuberc Lung Dis 2005; 9: 437-42. [?zet]
- White NW. Byssinosis in South Africa. A survey of 2411 textile workers. S Afr Med J 1989; 75: 435-42. [?zet]
- Al-Khal AL, Bener A, Enarson DA. Tuberculosis among garment workers in an Arabian developing country: State of Qatar. Arch Environ Occup Health 2005; 60: 295-8. [?zet]
- Kistnasamy B, Yach D. Tuberculosis in commerce and industry in a Western Cape suburb, South Africa, 1987. Am J Ind Med 1990; 18: 87-93. [?zet]
- Anjum A, Mann AA, Anjum MA. Health concerns among workers in weaving industry: a case study of tehsil Faialabad Pakistan. J Agric Soc Sci 2009; 5: 106-8.
- Horna-Campos OJ, Bedoya-Lama A, Romero-Sandoval NC, Mart?n-Mateo M. Risk of tuberculosis in public transport sector workers, Lima, Peru. Int J Tuberc Lung Dis 2010; 14: 714-9. [?zet]
- Horna-Campos OJ, Consiglio E, Sanchez-Perez HJ, Navarro A, Cayla JA, Martin-Mateo M. Pulmonary tuberculosis infection among workers in the informal public transport sector in Lima, Peru. Occup Environ Med 2011; 68: 163-5. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Aylin BABALIK,
SB S?reyyapa?a G???s Hastal?klar? ve
G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi,
G???s Hastal?klar? Klini?i,
?STANBUL - TURKEY
e-mail: aylinbabalik@gmail.com