Akci?erde t?berk?loz d??? mikobakteri infeksiyonu: 75 olgu
Aylin BABALIK1, T?lin KUYUCU1, Emine N. ORDU1, Dilek ERNAM1, Mualla PARTAL1, Kaya K?KSALAN2
1 SB S?reyyapa?a G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi,
G???s Hastal?klar? Klini?i, ?stanbul,
2 ?stanbul ?niversitesi Deneysel T?p Ara?t?rma Enstit?s?, ?stanbul.
?ZET
Akci?erde t?berk?loz d??? mikobakteri infeksiyonu: 75 olgu
Giri?: T?berk?loz d??? mikobakteri ?zellikle AIDS ve imm?ns?presif hastalarda yayg?n olarak g?zlenmektedir. Bu ?al??ma, klinik ?nemi a??s?ndan hastalar?n balgam ?rneklerinde MOTT i?eri?inin ara?t?r?lmas? amac?yla tasarlanm??t?r.
Hastalar ve Metod: 2009-2010 y?llar?nda, S?reyyapa?a G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi kliniklerinde t?berk?loz d??? mikobakteri tan?s? alan toplam 75 hastada [30 kad?n (%40), 45 erkek (%69); ortalama ya? (SS): 48.7 (15.9) y?l] h?zl? test ve NAP testi kullan?larak MGIT y?ntemiyle L?wenstein-Jensen (LJ) de (51.864 LJ) atipik b?y?me tespit edildi. Tespit i?lemleri 31 (%43) hastada, Hsp65PCRREA y?ntemlerine g?re yap?ld?. Tedavi y?netimi, radyoloji, bakteriyoloji, e?lik eden hastal?klar ve tedavi sonu?lar? t?bbi kay?tlar?n incelenmesi, hastalar?n do?rudan aranmas? ve t?berk?loz dispanserlerin verilerine ula??lmas? yolu ile elde edildi.?
Bulgular: Mycobacterium abscessus 9 (%28) hastada, Mycobacterium avium kompleks 8 (%25) hastada, Mycobacterium kansasii 5 (%16) hastada Hsp65PCRREA y?ntemleriyle tespit edildi. "American Thoracic Society" tan?m ve tedavi kriterlerine sahip 18 (%24) hastada, tedavi min?r ve maj?r ila?larla y?r?t?ld?. Standart t?berk?loz tedavisi 75 olgunun 25 (%33)'inde uyguland?. T?berk?loz d??? mikobakteri tespiti 25 olgudan 8 (%32)'inde g?zlendi. Takip d?nemi 75 olgunun 32'sinde tedavisiz y?r?t?ld?. Tek bir pozitif atipik b?y?me 43 (%72) olguda saptand?. Toplamda 43 olguya uygulanan tedavi, 25 (%58) olguda iyile?me, 3 (%7) olguda ba?ar?s?zl?k ve 3 (%7) olguda ?l?mle sonu?land?. ?la? direnci 36 olguda saptand?. Herhangi bir ila? direnci 31 (%86) olguda, HR ila? direnci ise 27 (%75) olguda tespit edildi. T?berk?loz tedavi ?yk?s? 20 (%40) olguda mevcuttu. Respiratuar ve nonrespiratuar hastal?klar e?it ?ekilde olgular?n 18 (%38)'inde tespit edildi. Radyolojik konsolidasyon 28 (%65) olguda, kavite ise 16 (%37) olguda tespit edildi.
Sonu?: K?lt?r y?ntemleri arac?l???yla t?berk?loz d??? mikobakteri tespiti, uygun tedavi ve epidemiyolojik de?erlendirme yapabilmek ad?na ?nemlidir.
Anahtar Kelimeler: T?berk?loz d??? mikobakteri, balgam k?lt?r?, h?zl? test ve NAP testi, MGIT.
SUMMARY
Non-tuberculous mycobacteria infection: 75 cases
Aylin BABALIK1, T?lin KUYUCU1, Emine N. ORDU1, Dilek ERNAM1, Mualla PARTAL1, Kaya K?KSALAN2
1 Clinic of Chest Diseases, Sureyyapasa Chest Diseases and Chest Surgery Training and
Research Hospital, Istanbul, Turkey,
2 Istanbul University Research Institute of Experimental Medicine, Istanbul, Turkey.
Introduction: Non-tuberculosis mycobacterium is especially seen in AIDS and non-immunosuppressant patients. This study was designed to evaluate data relating to non-tuberculosis mycobacterium content in patients' sputum for the clinical importance.
Patients and Methods: During 2009-2010 at Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital clinics, 75 patients [30 women (40%) and 45 men (69%); mean age (SD): 48.7 (15.9) years] with non-tuberculosis mycobacterium were determined by the rapid test and NAP test in Mycobacteria Growth Indicator Tube (MGIT), which had atypical growth in 51.864 Lowenstein-Jensen. Identification was done with Hsp65PCRREA methods in 32 (43%) cases. Treatment management, radiology, bacteriology, co-morbidity, treatment outcomes were evaluated from medical records, calling patients and from tuberculosis dispensaries.
Results: In 9 (28%) patients Mycobacterium abscessus, in 8 (25%) patients Mycobacterium avium complex (MAC), in 5 (16%) patients? Mycobacterium kansasii was found with identification Hsp65PCRREA methods. In 18 (24%) of 75 cases with American Thoracic Society definition and treatment criteria, treatment was administered using major and minor drugs. Standard tuberculosis treatment was administered in 25 (33%) of the 75 cases. In 8 of 25 (32%) cases identification of non-tuberculosis mycobacterium was evident. In 32 of 75 cases follow up was performed with no treatment. One positive atypical growth culture was identified in 23 (72%) of 32 patients.? Treatment was administered in 43 cases while 25 (58%) of 43 were cured, 3 (7%) of 43 were default and 3 (7%) died. Drug resistance was the outcome in 36 cases. While 31 (86%) had any drug resistance, 27 (75%) had HR drug resistance. Past history of tuberculosis treatment was evident in 20 (40%) cases. Respiratory and non-respiratory diseases were identified equally in 18 (38%) cases. Radiological consolidation in 28 (65%), and cavity in 16 (37%) cases were determined.
Conclusion:? In order to carry out the right treatment and epidemiologic evaluation, it is important to identify non-tuberculosis mycobacterium by culture methods.
Key Words: Non-tuberculosis mycobacterium, sputum culture, rapid test, NAP test, MGIT.
Geli? Tarihi/Received: 15/05/2011 - Kabul Edili? Tarihi/Accepted: 22/01/2012
Introduction
Non-tuberculosis mycobacterium (NTM) is generally referred to as mycobacterium rather than Mycobacterium tuberculosis complex or Mycobacterium leprae (1). It is thought that NTM is not transmitted from person-to-person (1). NTM are environmental organisms found in soil and water worldwide. They are considered opportunistic pathogens, and several species are associated with human disease, typically pulmonary, skin/soft tissue, lymphatic, or disseminated in presentation (2).
Mycobacterium avium complex (MAC), Mycobacterium kansasii and rapidly growing mycobacteria (RGM) such as Mycobacterium abscessus and Mycobacterium fortuitum constitute the main species associated with human pulmonary disease (1,3).
Epidemiology studies of pulmonary NTM infections are generally limited in several ways. Firstly, since NTM are often isolated from the environment, including potable water, specimen contamination is a significant concern. Secondly, the mere presence of NTM in the lungs does not necessarily imply significant or progressive pulmonary disease. Thirdly, because the isolation of NTM does not mandate informing a ?reportable disease' officially in many jurisdictions, surveys of the epidemiology of NTM often consist of incomplete samples (4,5).
In the past two decades, an increase in the prevalence of NTM infection/disease has been noted worldwide (3,4,6). Suggested reasons include a rise in prevalence of human immunodeficiency virus infection and other acquired immunocompromised states, an increased understanding of the clinico-pathological relationship between host and pathogen and awareness of these organisms as potential pathogens, advances in methods of detection and recovery of the organisms (1).
In our country, identification of NTM is not used in our country routine in laboratories. Generally wrongly treatment is administered to these patients. Firstly these patients are treated wrongly standard short course tuberculosis (TB) treatment for long time. These patients generally have major drug resistance especially for isoniazid and rifampicin and treatment failure are occurred after the treatment failure with standard short course TB treatment. Secondly, multi-drug resistance TB (MDR-TB) treatment is begun treatment with second-line drugs for a long time after the treatment failure with standard short course TB treatment. Generally, treatment of NTM is delayed several months. Importance of identification of NTM is thought for these reasons. And another important thing is differentiation of real disease between contaminations for true treatment.
PATIENTS and Methods
This study was designed as a retrospective descriptive study conducted with NTM patients being followed up at Sureyyapasa Chest Diseases and Chest surgery Training and Research Hospital including r-nitro-a-acetylamino-b-hydroxypropiophenone (NAP) and rapid testing that were carried out in comparison of the Mycobacteria Growth Indicator Tube (MGIT) and revealed an atypical growth in Lowenstein-Jensen (LJ) (2009-2010). Identification of NTM was established by using Hsp65PCRREA methods at Istanbul University Institute of Experimental Medicine laboratory. Diagnosis was done according to American Thoracic Society (ATS) guideline (7). After determined an atypical growth in LJ, NAP and rapid testing was carried out in MGIT.
According to ATS guideline, if the patients had treatment failure or delayed sputum and culture conversion under the standard short course TB treatment, identification was established by using hsp65 PCR-Restriction Enzyme Analysis (Hsp65PCRREA) methods. Furthermore, NTM was considered either clinically or radiologically, according to ATS guideline by clinician and identification was established by using Hsp65PCRREA methods. If the patients had sputum and culture conversion and clinically improvement under the standard short course TB treatment, standard TB treatment was continued and identification is not worked.
According to ATS guidelines generally for patients being followed up in outpatient clinics, if the patients had only one culture positive and atypical growth diseases were not thought by clinically and radiological and the patients were followed with no treatment. Identification of NTM is not worked for these patients. Some of identification could be done if their LJ culture were suitable in treated standard short course TB treatment and no treatment patients for evaluation in this research.
Definition of disease, administered drugs, radiology, bacteriology, co-morbidity, treatment outcomes were evaluated using medical records. Treatment outcome and treatment management were evaluated by calling patients and using information obtained from TB dispensaries' files.
Results
Basic demographic and clinical features are shown in Table 1. During 2009-2010 at Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital clinics, 75 patients [29 (39%) women, 46 (61%) men, mean age (SD): 48.7 (15.9) years] with MOTT were determined with rapid testing and NAP testing in MGIT in 51.864 LJ, which had atypical growth.
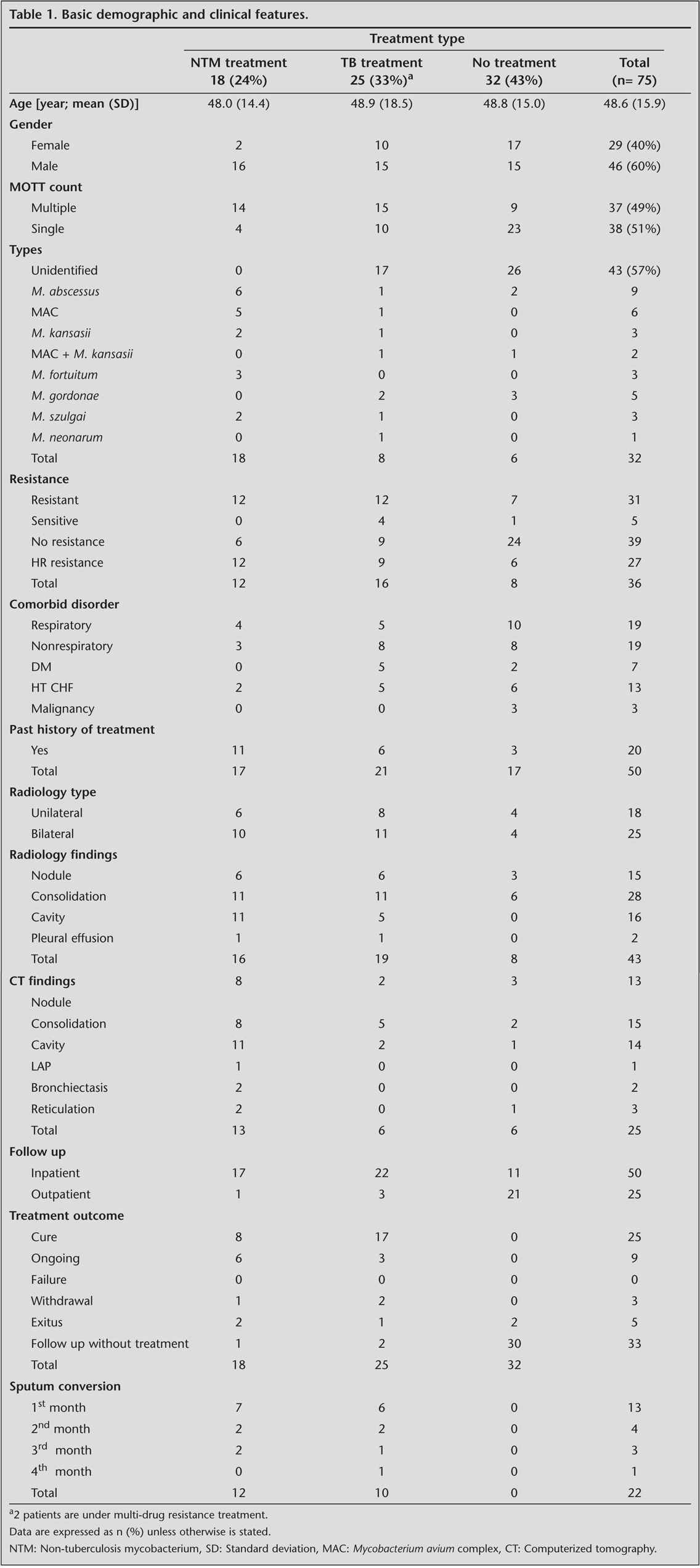
Identification was done with Hsp65PCRREA methods in 32 (43%) cases. Results of identification with Hsp65PCRREA methods included 9 (28%) M. abscessus, 6 (19%) MAC, 5 (16%) M. kansasii, 2 (6%) M. abscessus + M. kansasii, 3 (9%) M. fortuitum, 5 (16%) Mycobacterium gordonae, 3 (9%) Mycobacterium szulgai, 1 (3%) Mycobacterium neonarum.
In 18 (24%) of 75 cases with ATS definition and treatment criteria, treatment was administered using major and minor drugs. In 25 (33%) of the 75 cases standard TB treatment was administered while 32 (40%) of 75 cases were followed up with no treatment.
In 18 cases, all of cases had identification including 6 (33%) M. abscessus, 5 (28%) MAC, 2 (11%) M. kansasii, 3 (17%) M. fortuitum and 2 (11%) M. szulgai cases. In 25 cases, 8 cases had identification of NTM including 1 (12.5%) M. abscessus, 1 (12.5%) MAC, 1 (12.5%) MAC + M. kansasii, 2 (25%) M. gordanae, 1 (12.5%) M. szulgai and 1 (12.5%) M. neonarum. In 32 cases, 6 cases had identification of NTM. M. abscessus was evident in 2 (30%) while MAC + M. kansasii in 1 (17%).
A single positive culture was evident in 38 (51%) cases while 37 (49%) had more than one positive culture. Of 18 cases treated with NTM treatment, 14 (78%) had more than one culture and of 25 cases treated with standard short course treatment, 15 (60%) had more than one culture while 32 cases without treatment, 23 (72%) had one culture.
Of 18 cases, 14 were evaluated treatment regimes before NTM treatment. Mean (SD) duration of major TB drug treatment was 147.8 (125) days.
A drug susceptible test was done in 36 (48%) of 75 cases. 31 (86%) of 36 had no drug resistance; and 27 (87%) of 31 had HR drug resistance. Of 75 cases 50 were inpatient, hence their data files could not be evaluated. In 19 (38%) of 50 cases respiratory diseases and in 19 (38%) of 50 cases non-respiratory diseases were evident. Past history of treatment was evident in 20 (40%) of 50 cases.
Radiology findings were evaluated in 43 (57%) of 75 cases and 18 (42%) of 43 had unilateral radiology, 25 (58%) of 43 had bilateral radiology findings. In 15 (35%) of 43 cases nodule, 28 (65%) of 43 consolidation, 16 (37%) of 43 cases cavity and 2 (5%) of 43 cases pleural effusion were identified. In 25 (33%) of 75 cases Thorax computerized tomography (CT) findings were evident including diagnosis of a nodular lesion in 13 (52%) of 25, of a consolidation lesion in 15 (60%) of 25 and a cavity lesion in 14 (56%) of 25.
In 16 (89%) of 18 cases with the diagnosis and treatment of MOTT radiological findings were available including findings of consolidation in 11 (69%) and cavity in 11 (69%) of 16 cases. Thorax CT findings available in 13 (72%) of 18 cases revealed nodular lesion in 11 (85%), consolidation lesion in 8 (62%) while cavity lesion in 8 (62%) of 13 cases.
In 18 who had NTM treatment, 8 (44%) cases were cured, 6 (33%) cases were under treatment, 1 (5%) case was default, 2 (11%) case died, and 1 (5%) case was followed up with no drug treatment.
In 18 who had NTM treatment, 15 cases were sputum smear positive and 12 cases were evaluated sputum smear conversion, 7 (58%) of 12 had sputum smear conversion in the first month, 2 (17%) of 12 had sputum smear conversion in the second month, 2 (17%) of 12 had smear conversion in the third month. End of the third month smear conversion had been achieved in 11 (92%) of 12 cases.
In 25 who were treated with standard short course treatment, 17 (70%) cases were cured, 3 (12%) cases were under treatment, 2 (8%) cases were default, 1 (4%) case died, 2 (8%) cases were followed-up with no drug treatment.
In 25 who were treated standard short course treatment, 19 cases were sputum smear positive and 10 cases were evaluated sputum smear conversion, 6 (60%) of 10 had sputum smear positive in the first month, 2 (20%) of 10 had sputum smear positive in the second month, 1 (10%) of 10 had sputum smear positive in the third month, 1 (10%) of 10 had sputum smear positive in the fourth month. End of the third month smear conversion had been achieved 9 (90%) of 10 cases.
In 32 (40%) of 75 cases, follow up was performed without treatment. After calling the patients and the TB dispensaries, no patients needed any further treatment or visit to the dispensaries. However, two of 32 died because one of them had lymphoma, and one of them had lung cancer.
In Table 2, detail treatment regime, sputum and smear conversion time, treatment outcome, drug susceptibility and drug results are shown in 18 treated MOTT cases.
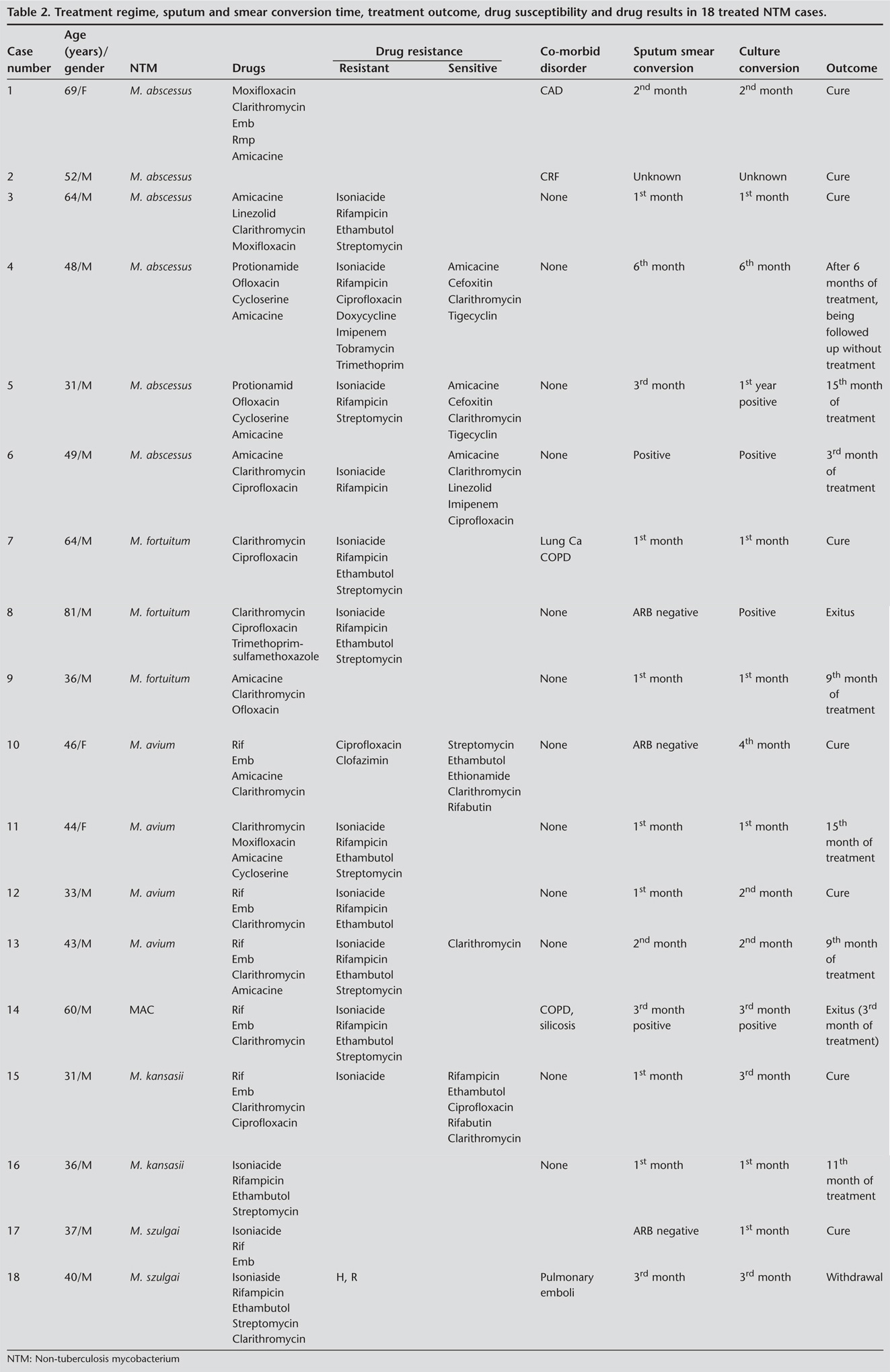
There were four M. avium, one MAC diseases, while two of five had clarithromycin susceptibility drug resistance. The diseases were treated with clarithromycin, ethambutol, amicacine, rifampin for at least 12 months after the culture conversion. Both of them had bilateral and cavitary diseases. One of them had culture conversion in the 4th month and was cured. The other one was under a 9th month treatment and had a culture conversion in the 2nd month. One of five patients was treated with clarithromycin, amicacine, moxifloxacin and cycloserine. These patients had bilateral radiologic and cavitary diseases and had culture conversion in 1st month of the treatment. Two of five patients had been treated with rifampin, ethambutol and clarithromycin. One of them had nodular radiological disease while culture conversion occurred in the 2nd month and cured. The other one who was treated with rifampin, ethambutol and clarithromycin had cavitary and bilateral diseases accompanied with chronic obstructive pulmonary disease (COPD) and Silicosis, while the culture and sputum smear were still positive in 3rd month when the patient died due to respiratory disease.
In 75 cases, there were two M. kansasii cases. They had no co-morbidity. One case had drug susceptibility test. This patient had culture conversion on the 3rd month. They had been treated according to drug susceptibility test (rifampin, ethambutol, clarithromycin, ciprofloxacin), after 12 months of culture conversion and the treatment resulted in cure. The other of M. kansasii case had been treated with rifampin, isoniazide, ethambutol and pyrazinamide (only two months). Their culture conversion was achieved after 1st month and under the treatment.
There were six M. abscessus diseases five of which were evaluated. Standard MDR treatment regime was administered in two of them with protionamide, ofloxacin, cycloserine and amicacine. They developed drug susceptibly for amicacine, cefoxitin and clarithromycin. One of them was found positive on the 5th month and treatment was stopped and the patients were followed up with no-drug treatment, because cefoxitin drug is not available in Turkey now. One of them was still culture positive in the 14th month of this treatment. Multidrug treatment regime with clarithromycin and parenteral treatment drug (amicacine and amicacine plus linezolid) was administered in two of six patients who were treated for 12 months after the culture conversion. Culture conversion occurred on 2nd and the patient was cured. One of six cases is still being treated with clarithromycin, amicacine and ciprofloxacin while the sputum and culture positivity is still continuing.
There were two M. fortuitum cases. One of them was treated and achieved sputum, culture conversion on the 1st month and was cured with clarithromycin, ciprofloxacin at least 12 months after the culture conversion. The other one was administered with clarithromycin, ciprofloxacin, trimethoprim-sulfamethoxazole (TMP-SMX) but he wasn't compliant with the treatment and died from respiratory dysfunction.
There were three M. szulgai. One of them was treated with isoniazid, rifampicin and ethambutol at least 12 month after culture conversion and had culture conversion on the 1st month. The other following sputum and culture conversion on the 3rd month was administered with isoniazid, rifampicin, ethambutol, pyrazinamide and clarithromycin but the treatment failed due to adverse side effects. There were five death patients in all 75 cases. Two of them in 18 cases accepted to be treated with MOTT. One of them was M. fortuitum and had hypertension co-morbidity disease and could not comply with the treatment and died from respiratory dysfunction in the 1st month. The other had co-morbid MAC disease, silicosis and COPD and developed respiratory insufficiency and died on the 3rd month. One patient in 25 cases who had been treated with standard short course TB treatment had hypertension, diabetes mellitus, and COPD and died on the 1st month of treatment. No treatment had been administered in two of five death cases. One of them had M. gordonae and had lymphoma while other one wasn't identified with NTM and had lung cancer.
Discussion
The first guideline of diagnosis was published by Wolinsky in 1979 and followed by ATS and British Thoracic Society (BTS) guidelines (8,9,10). As stated in the latest ATS guideline, patients who do not meet the diagnostic criteria should be followed until the diagnosis is firmly established or excluded. For all cases treatment advantages and non-advantages has to be considered. ATS recommend treatment is a decision based on potential risk and benefits of therapy for individuals (9).
In 18 (24%) of 75 cases with ATS definition and treatment criteria, treatment was administered with major and minor drugs. In 25 (33%) of the 75 cases standard TB treatment was administered while in 32 (40%) of 75 cases follow up was performed without treatment.
According to ATS diagnosis, appropriate clinical and radiologic evidence with more than one culture is significant. In 14 (78%) of 18 who were treated with NTM treatment, more than one positive atypical growth culture was identified and 8 (44%) cases were completed treatment with cure. End of the third month, smear conversion was achieved 92%. In 17 (70%) of 25 cases treatment was completed with cure. End of the third month, smear conversion was achieved in 90%. Treatment outcome was better in NTM treatment and standard TB treatment.
Achievement of high treatment success for standard short course TB treatment may be due to some reasons. First, these were real TB cases and NTM colonization while 40% of them had one atypical growth positive culture. Second, only 8 (32%) had identification of NTM. M. kansasii, M. szulgai, M. gordonae identification rate could be high as M. kansasii and M. szulgai were known to have good result with standard TB treatment (9). M. gordonae has been almost always considered non-pathogenic and most frequently isolated mycobacterial contamination (9).
In 23 (72%) of 32 cases without treatment, one positive growth culture was identified. In 32 cases, six cases had identification of NTM while 3 (50%) of them were identified to be M. gordonae by calling patients and TB dispensaries.
Wolingsky described three stages of interaction between the organism and host colonization, infection and disease. ATS have proposed criteria to differentiate between colononization/contamination and disease and encompass bacteriological, radiological and clinical criteria (9). Martin-Casabona et al. performed a multi-country respective survey leading number of patients reported with NTM to be 36.099 from 14 countries. M. avium complex, M. gordane, M. xenopi, M. kansasii and M. fortuitum were five species reported (3).
In 18 cases, all of cases had identification including 6 (33%) M. abscessus, 5 (28%) MAC, 2 (11%) M. kansasii, 3 (17%) M. fortuitum and 2 (11%) M. szulgai.
Some demographic characteristics have been described for NTM cases. The risk factors for NTM colonization are largely unknown. Hernandez et al. reported older age, female sex, being born in Canada, long residency in BC and White race to predict pulmonary NTM colonization (11).
Lung disease due to NTM occurs commonly in structural lung disease, such as COPD, bronchiectasis, cystic fibrosis, pneumoconiosis, prior TB, pulmonary alveolar proteionosis and esophageal motility disorders (12-15). Ye et al. evaluated 46 patients diagnosed with MAC pulmonary disease and reported that 31 (67%) of 46 patients had pre-existing lung diseases, including history of pulmonary tuberculosis (16). Winthrop et al. reported that cavitation (24.5%), bronchiectasis (16%), COPD (28%) and immunosuppressive therapy (25.5%) were common in NTM diseases indicating presence for respiratory and non-respiratory diseases among 19 (38%) of 50 inpatient cases (17). Additionally, 20 (40%) of 50 cases was reported to have past history of treatment.
The prevalent high-resolution CT scan (HRCT) findings were bilateral centrilobular nodules and cylindrical bronchiectasis. These changes correlate with bronchiolar/peribronchiolar inflammation due to tissue invasion by NTM like MAC and M. abscessus. It has been suggested that about 30% of patients with changes of bilateral bronchiectasis and bronchiolitis on HRCT had NTM disease; extensive radiographic abnormalities, cavitation or consolidation and female gender provided additional risks (1). Kuroishi evaluated prognostic implications of HRCT findings in assessing response to treatment MAC pulmonary disease. Atelectasis, cavites and pleural thickening on HRCT were significantly more frequently and extensive among patients in the sputum nonconverted group (18). Koh et al. found 52% nodular bronchiectasis form, 42% upper lobe cavity form in MAC lung disease (19). Contrast to known, in our 18 cases who had diagnosed and treated MOTT, 11 (69%) had consolidation and 11 (69%) had cavity. 11(85%) had nodular lesion, 8 (62%) cases had consolidation lesion, 8 (62%) cases had cavity lesion at computerized thorax tomography.
ATS and BTS recommend use of drug susceptibility test for treatment failure and relapse cases (9,10). Routine susceptibility testing of MAC isolates is recommended for clarithromycin only. Routine susceptibility testing of M. kansasii isolates is recommended for rifampin only. Routine susceptibility testing for RGM should be with amicacine, imipenem, doxycycline, quinolones, TMP-SMX, cefoxitin, clarithromycin, linezolid and tobramycin (9). In our study drug susceptibility test for first-line tuberculosis drugs was performed in 36 (48%) of 75 cases while 31 (86%) of 36 cases had no drug resistance. HR drug resistance was evident in 27 (87%) of 31 cases. After the identification of mycobacterium, drug susceptibility test for second-line drugs was done 6 (30%) of 18 patients.
Empiric therapy for suspected NTM lung disease is not recommended. Such cases should be followed up closely, until diagnosis is firmly established or excluded (9). Treatment recommendations for species like MAC and M. kansasii are generally more evidence based (1).
The recommended initial regimen for most patients with MAC lung disease is including clarithromycin, azithromycin, ethambutol, rifampicin. Aminoglycosides should be considered in initial phase and are recommended for patients with severe or previously treated disease. The primary microbiologic goal of therapy is 12 months of negative sputum cultures while pulmonary disease of MAC generally occurs in 40-50 years old men in apical fibrocavitary form. The other form shows nodularity and bronchiectasis form in older, non-smoking women (20). Ye et al. evaluated 46 retrospective cases. They found that multivariate analysis of risk factors for failure of sputum conversion was significant inappropriate treatment (16). Kim et al. reported that combined regime including clarithromycin was effective against MAC pulmonary diseases (21). Field et al. showed that empiric treatment with combination treatment was achieved sputum conversion 90% (22). We had 4 M. avium and 1 MAC diseases and two of five had claritromycin susceptibility drug resistant. All patients had been planned to be treated with multi-drug combination treatment with clarithromycin, three of them with amicacine and one of them with quinolone. One of them had co-morbid diseases including COPD and Silicosis, and still culture and sputum smear positive on 3rd month when the patient died.
M. kansasii lung disease has been treated with ATS recommended regimen including rifampin, ethambutol, isoniazide and pyridoxine. Treatment should include 12 months of negative sputum cultures. ATS recommended rifampin drug susceptibly test. For patients with rifampin-resistant M. kansasii disease, a three-drug regimen is recommended based on in vitro susceptibilities including clarithromycin or azithromycin, moxifloxacin, ethambutol, sulfamethoxazole, or streptomycin (9). Park investigated the clinical and radiological features and treatment outcomes of M. kansasii lung diseases in Korea, respectively. The most common radiographic findings were nodules, consolidation, cavitation. With appropriate treatment with isoniaside, rifampin and ethambutol, a good prognosis was evident (23). We had 2 M. kansasii cases. One case had drug susceptibility test. This M. kansasii patient had been administered treatment according to drug susceptibility test with clarithromycin and ciprofloxacin. The other of M. kansasii case had been planned to be treated with first-line drugs.
The three main species of RGM ausing pulmonary diseases are M. abscessus, M. chelonae and M. fortuitum. Treatment relies heavily on guidance from antimicrobial susceptibility testing as there are virtually no large-scale clinical studies. Most data emerge from case reports or small series (1).
For M. abscessus, at present, there is no reliable antibiotic regimen, even based on in vitro susceptibilities and including parenteral agents, to produce cure for M. abscessus lung disease. Periodic administration of multidrug therapy, including a macrolide and one or more parenteral agents (amicacine, cefoxitin, or imipenem) or a combination of parenteral agents over several months may help control symptoms and progression of M. abscessus lung disease (9). Treatment generally involved a combination of amicacine, and clarithromycin. The treatment of M. abscessus particularly can be quite difficult as it is highly resistant to antituberculous drugs. However, this is difficult to administer or tolerate for long periods (1). Some research showed that tigecycline is effective for treatment of M. abscessus (24). Leber et al. found that, in multivariable analysis, M. abscessus infection, intravenous therapy, and M. xenopi infection were all associated with increased monthly treatment cost (25). In our study six cases were accepted five M. abscessus. In two of them standard MDR treatment regime with second-line drugs including protionamide, ofloxacin, cycloserine and ecacine was administered resulting in treatment failure. Their treatment was changed according to susceptible drugs. In two of six patients cure was obtained with multidrug treatment regime with clarithromycin and parenteral treatment drug (amicacine and amicacine plus linezolid). One of six cases is being treated with clarithromycin, amicacine and ciprofloxacin.
M. fortuitum isolates are usually susceptible to multiple oral antimicrobial agents, including the newer macrolides and quinolones, doxycycline and minocycline, and sulphonamides. For M. fortuitum lung disease, therapy with at least two agents with in vitro activity against the clinical isolate should be given for at least 12 months of negative sputum cultures. The optimal choice of agents is unknown, and would likely be dictated by patient tolerance; however, any two-drug combination based on in vitro susceptibility should be successful (9). We had two M. fortuitum cases. One of them was with clarithromycine, ciprofloxacin. The other was initiated clarithromycin, ciprofloxacin, TMP-SMX but he could not compliance treatment and died from respiratory insufficiency.
M. szulgai is rarely recovered from the environment, cultures yielding M. szulgai almost always have a pathological significant. Susceptibility of M. szulgai to quinolones and to the newer macrolides has also been reported. Three to four drug regimens that includes 12 months of negative sputum cultures while on therapy is probably adequate (9). At least one patient has been reported to have been treated successfully with a standard 6-month TB regimen including isoniaside, rifampicin, and pyrazinamide. Treatment with rifampicin, ethambutol and a macrolide antibiotics leads to favorable outcomes (9). Ingen evaluated 21 patients in The Netherlands from M. szulgai that was isolated during 1999-2006. They found that clinical isolation of M. szulgai generally true disease and demands careful follow-up (26). We have three M. szulgai and two of them occurred at least 12 month after the culture conversion. One of them was cured with isoniaside, rifampin and ethambutol. Treatment failed in the other one after sputum and culture conversion on 3rd month with HZRE and clarithromycin. One of them was treated with re-treatment regime and treatment outcome was cure.
The significance of an isolate also varies with the species of mycobacteria. Isolation of mycobacteria like M. gordonae, M. mucogenicum, M. haemophilum, M. flavescens, M. gastri, M. terrae complex or M. triviale usually indicates transient colonization or contamination though disease has been reported (1). We have five M. gordonae cases, two of them were treated with standard tuberculosis treatment while three of them had not administered any drug treatment and they had no diseases.
The major limitation of our study is its retrospective design. Identification of NTM was not evident in all cases and later identification of NTM was also not possible in all of cases. Secondly, treatment outcome was achieved via calling patients and TB dispensaries. Treatment follow up was not performed every month in our hospital for all cases. Thirdly, most of cases had not drug susceptibility test. Treatment of NTM was not performed according to drug susceptibility. Fourth, there was not standard treatment approach for these NTM cases.
More fundamental information is needed to improve understanding in essentially all areas of NTM disease. There is little information about the incidence or prevalence of MOTT diseases. Differentiation of disease and contamination should be certain before the treatment. Identification is important for suitable treatment approach, prevention of wrong and long first-line and second-line tuberculosis treatment. Generally there is no standard treatment approach for NTM cases. According to ATS and BTS recommendation, treatment recommendations for species like MAC and M. kansasii are generally more evidence based compared to the other mycobacterium. So that standard treatment approach is very difficult. Randomized controlled trials in well-described patients would provide stronger evidence-based data to guide therapy of NTM lung diseases.
CONFLICT of INTEREST
None declared.
REFERENCES
- Thomson RM, Yew WW. When and how to treat pulmonary non-tuberculous mycobacterial diseases. Respirology 2009; 14: 12-26. [?zet] [Tam Metin] [PDF]
- Cassidy
PM, Hedberg K, Saulson A, McNelly E, Winthrop KL. Nontuberculous mycobacterial
disease prevalence and risk factors: a changing epidemiology. Clin Infect Dis
2009; 49: e124-9.
[?zet] [Tam Metin] [PDF] - Martin-Casabona N, Bahrmand AR, Bennedsen J, Thomsen VO, Curcio M, Fauville-Dufaux M, et al; Spanish Group for Non-Tuberculosis Mycobacteria. Non-tuberculous mycobacteria: patterns of isolation. A multi-country retrospective survey. Int J Tuberc Lung Dis 2004; 8: 1186-93. [?zet]
- Marras TK, Chedore P, Ying AM, Jamieson F. Isolation prevalence of pulmonary non-tuberculous mycobacteria in Ontario, 1997-2003. Thorax 2007; 62: 661-6. [?zet] [Tam Metin] [PDF]
- Hernandez-Garduno E, Rodrigues M, Elwood RK. The incidence of pulmonary non-tuberculous mycobacteria in British Columbia, Canada. Int J Tuberc Lung Dis 2009; 13: 1086-93. [?zet]
- Khan
K, Wang J, Marras TK. Nontuberculous mycobacterial sensitization in the United
States: national trends over three decades. Am J Respir Crit Care Med 2007;
176: 306-13.
[?zet] [Tam Metin] [PDF] - Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175: 367-416. [Tam Metin] [PDF]
- Horsburgh CR Jr, Caldwell MB, Simonds RJ. Epidemiology of disseminated nontuberculous mycobacterial disease in children with acquired immunodeficiency syndrome. Pediatr Infect Dis J 1993; 12: 219-22. [?zet]
- Medical
Section of the American Lung Association. Diagnosis and treatment of disease
caused by nontuberculous mycobacteria. This official statement of the American
Thoracic Society was approved by the Board of Directors, March 1997. Am J
Respir Crit Care Med 1997; 156: 1-25.
[?zet] [Tam Metin] - Subcommittee of the Joint Tuberculosis Committee of the British Thoracic Society. Management of opportunist mycobacterial infections: Joint Tuberculosis Committee Guidelines 1999. Thorax 2000; 55: 210-8. [PDF]
- Hernandez-Garduno E, Elwood RK. Demographic risk factors of pulmonary colonization by non-tuberculous mycobacteria. Int J Tuberc Lung Dis 2010; 14: 106-12. [?zet]
- Giron RM, Maiz L, Barrio I, Martinez MT, Salcedo A, Prados C. Nontuberculous mycobacterial infection in patients with cystic fibrosis: a multicenter prevalence study. Arch Bronconeumol 2008; 44: 679-84. [?zet]
- Hadjiliadis D, Adlakha A, Prakash UB. Rapidly growing mycobacterial lung infection in association with esophageal disorders. Mayo Clin Proc 1999; 74: 45-51. [?zet]
- Griffith DE, Girard WM, Wallace RJ Jr. Clinical features of pulmonary disease caused by rapidly growing mycobacteria. An analysis of 154 patients. Am Rev Respir Dis 1993; 147: 1271-8. [?zet]
- Kanathur N, Shantaveerapa HN, Byrd RP Jr, Mehta JB, Roy TM. Nontubercular mycobacterial pulmonary infection in immunocompetent men. South Med J 2001; 94: 719-23. [?zet]
- Ye JJ, Wu TS, Chiang PC, Lee MH. Factors that affect sputum conversion and treatment outcome in patients with Mycobacterium avium-intracellular complex pulmonary disease. J Microbiol Immunol Infect 2007; 40: 342-8. [?zet]
- Winthrop KL, McNelley E, Kendall B, Marshall-Olson A, Morris C, Cassidy M, et al. Pulmonary nontuberculous mycobacterial disease prevalence and clinical features: an emerging public health disease. Am J Respir Crit Care Med 2010; 182: 977-82. [?zet] [Tam Metin] [PDF]
- Kuroishi S, Nakamura Y, Hayakawa H, Shirai M, Nakano Y, Yasuda K, et al. Mycobacterium avium complex disease: prognostic implication of high-resolution computed tomography findings. Eur Respir J 2008; 32: 147-52. [?zet] [Tam Metin] [PDF]
- Koh
WJ, Kwon OJ, Jeon K, Kim TS, Lee KS, Park YK, et al. Clinical significance of
nontuberculous mycobacteria isolated from respiratory specimens in Korea. Chest
2006; 129: 341-8.
[?zet] [Tam Metin] [PDF] - Wittram C, Weisbrod GL. Mycobacterium avium complex lung disease in immunocompetent patients: radiography-CT correlation. Br J Radiol 2002; 75: 340-4. [?zet] [Tam Metin] [PDF]
- Kim EY, Chi SY, Oh IJ, Kim KS, Kim YI, Lim SC, et al. Treatment outcome of combination therapy including clarithromycin for Mycobacterium avium complex pulmonary disease. Korean J Intern Med 2011; 26: 54-9. [?zet] [Tam Metin] [PDF]
- Field SK, Cowie RL. Treatment of Mycobacterium avium-intracellulare complex lung disease with a macrolide, ethambutol, and clofazimine. Chest 2003; 124: 1482-6. [?zet] [Tam Metin] [PDF]
- Park HK, Koh WJ, Shim TS, Kwon OJ. Clinical characteristics and treatment outcomes of Mycobacterium kansasii lung disease in Korea. Yonsei Med J 2010; 51: 552-6. [?zet] [Tam Metin] [PDF]
- Wallace RJ Jr, Brown-Elliott BA, Crist CJ, Mann L, Wilson RW. Comparison of the in vitro activity of the glycylcycline tigecycline (formerly GAR-936) with those of tetracycline, minocycline, and doxycycline against isolates of nontuberculous mycobacteria. Antimicrob Agents Chemother 2002; 46: 3164-7. [?zet] [Tam Metin] [PDF]
- Leber A, Marras TK. The cost of medical management of pulmonary nontuberculous mycobacterial disease in Ontario, Canada. Eur Respir J 2011; 37: 1158-652. [?zet]
- van
Ingen J, Boeree MJ, de Lange WC, de Haas PE, Dekhuijzen PN, van Soolingen D.
Clinical relevance of Mycobacterium szulgai in the Netherlands. Clin Infect Dis
2008; 46: 1200-5.
[?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Aylin BABALIK,
SB S?reyyapa?a G???s Hastal?klar? ve
G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi,
G???s Hastal?klar? Klini?i,
?STANBUL - TURKEY
e-mail: aylinbabalik@gmail.com