Thorax as an extraintestinal target for inflammatory bowel disease
Evrim Eylem AKPINAR1, Meral G?LHAN1, Halil DE?ERTEK?N2, ?m?r ATAO?LU3
1 Ufuk ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Ankara,
2 Ufuk ?niversitesi T?p Fak?ltesi, Gastroenteroloji Bilim Dal?, Ankara,
3 Mikro-pat, Patoloji Laboratuvar?, Ankara.
Inflammatory bowel disease (IBD) is a chronic and relatively common disorder of uncertain etiology (1). IBD can be associated with a variety of respiratory disorders (2). A link between pulmonary disease and IBD was suggested nearly 40 years ago (3). Both screening studies and the cumulative volume of case reports suggest that respiratory system may be involved in IBD more frequently than it is generally appreciated (4).
The colonic and respiratory epithelia both share embryonic origin from the primitive foregut (5). Although, many of the reported pulmonary diseases associated with IBD have cryptic etiologies, the causes or mechanisms of respiratory tract involvement in IBD remain poorly understood (2).
A 51 years old female patient was admitted to our clinic with the complaints of cough, fever and sputum production for 10 days and abdominal pain, bloody stool and diarrhea for two days. The patient was a lifelong non-smoker and had no history of occupational or environmental exposure relevant to lung disease. Despite empirical antibiotic treatment, there was no clinical improvement.
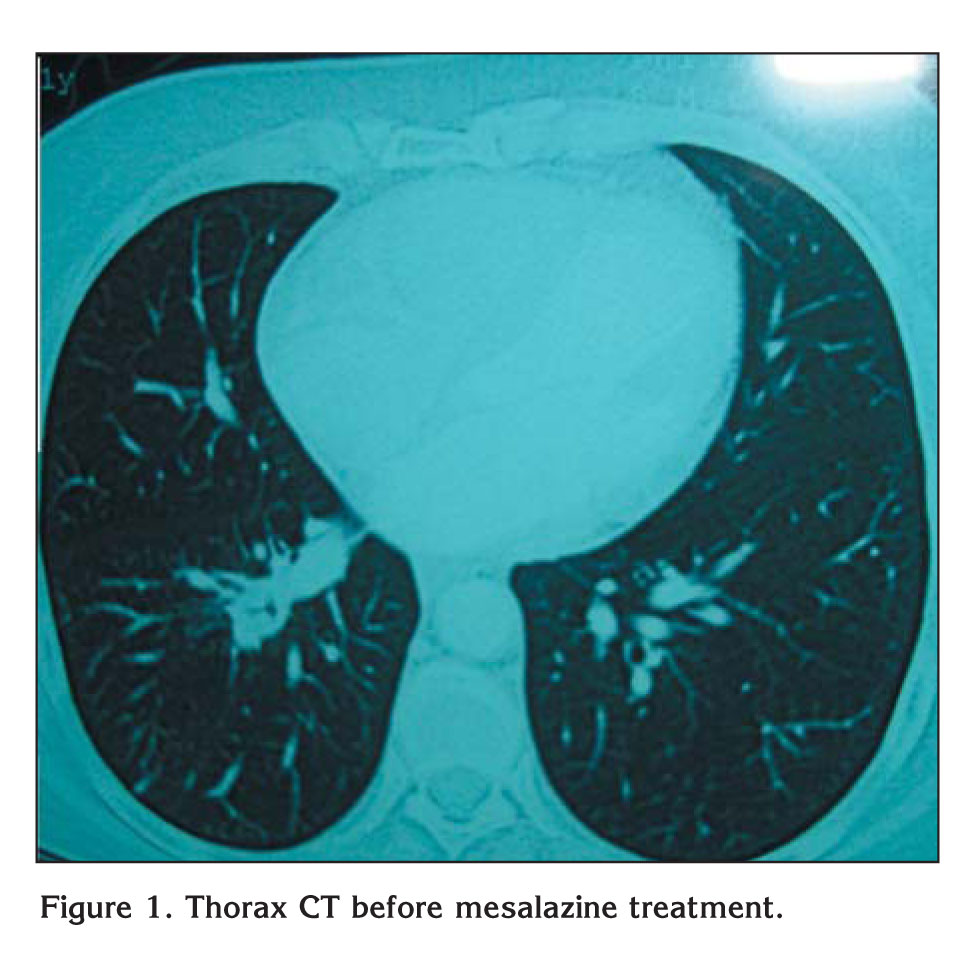
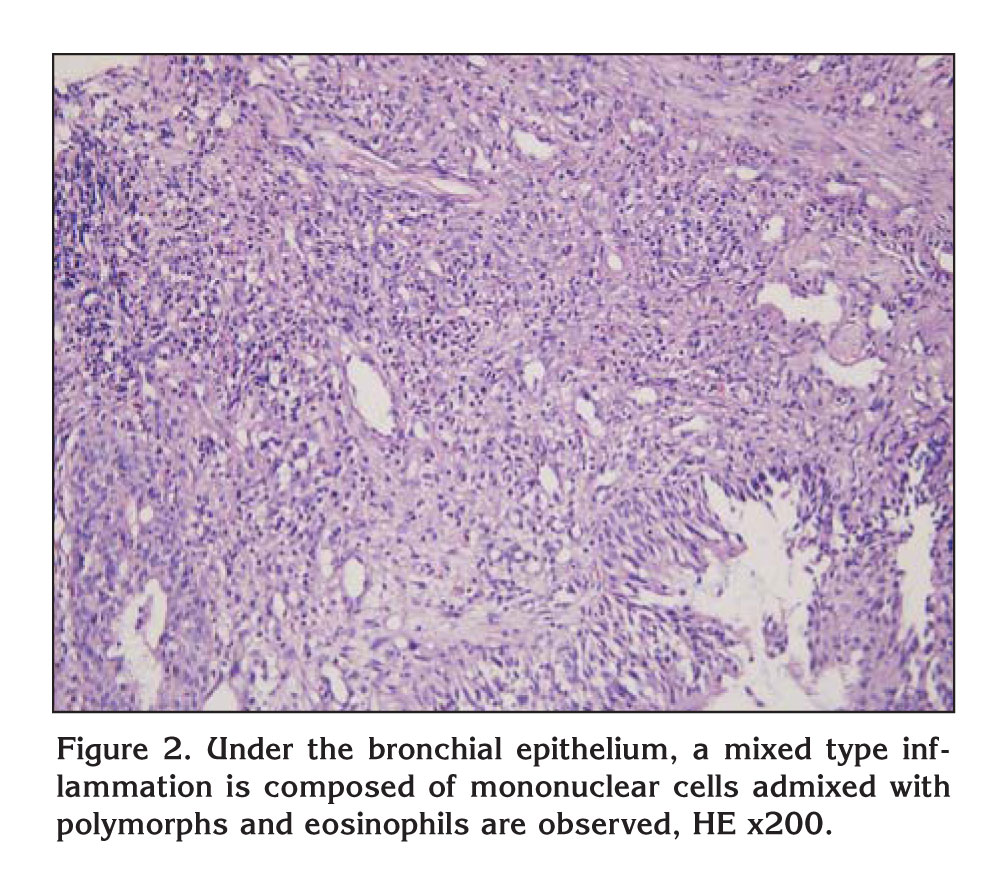
Chest X-ray revealed infiltration at the right lower zone. Pulmonary function test was normal. Connective tissue markers including ANA, anti-dsDNA, RF were negative. Erytrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were high. Contrast-enhanced computed tomography revealed segmental atelectasis on the right lower lobe and infiltration around atelectasis (Figure 1). A bronchoscopy was performed; there was endobronchial polypoid lesion on the posterior wall of the posterior segment of right lower lobe. Bronchoscopic biopsy revealed subepithelial fibrosis and under the bronchial epithelium, a mixed type inflammation is composed of mononuclear cells admixed with polymorphs and eosinophils were observed (Figure 2). Extensive search for bacterial (including mycobacterium), fungal and parasitic infectious agents were all negative.
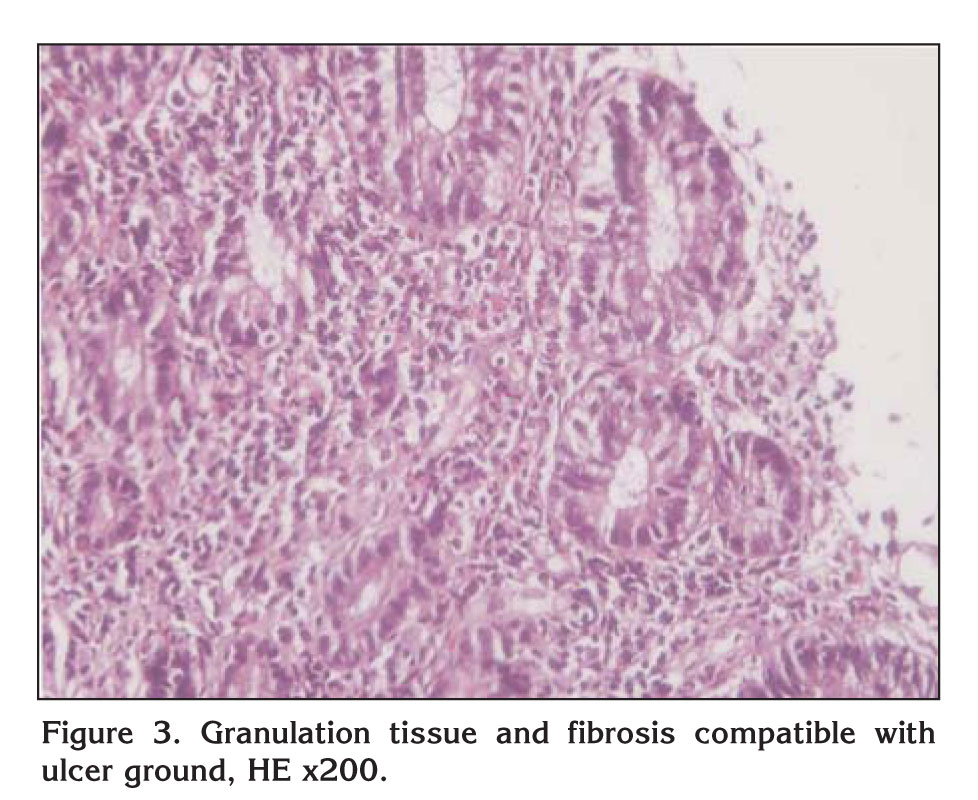
A colonoscopy was also performed. Because there were ulcerations and pseudopolips on transverse colon mucosa, multiple biopsies were taken. Focal inflammation was seen on pathological examination of colonic biopsies (Figure 3). When colonoscopy and pathologic examination considered together, patient was diagnosed as Crohn?s disease. Endobronchial lesion of the lung was evaluated as Crohn?s disease after other causes of endobronchial lesions including neoplasms and infectious causes were excluded. Oral mesalazine (500 mg for three times a day) was started. Both respiratory symptoms and abdominal symptoms of the patient were totally improved at the first month of the mesalazine treatment. On laboratory examination ESR and CRP levels were in normal limits. Complete radiological and bronchoscopic resolution were also revealed in follow up examination.
Respiratory system may be involved in very different patterns in Crohn?s disease (6). However, to our knowledge, this is the first case of Crohn disease?s pulmonary involvement as endobronchial polypoid lesion.
Overt and clinically significant lung involvement of Crohn?s disease is rare. However, lung function test abnormalities were seen more often especially during attack periods of the disease (6,7,8). The decrease in carbon monoxide diffusion capacity (DLCO) is the pulmonary function test abnormality that is most often seen in IBD, especially in active phase of the disease, both in pediatric and adult patients (6,9,10). Small airway dysfunction, hyperinflation with increased functional residual capacity and residual volume bronchial hyperreactivity was also detected among patients with IBD (6,8,10,11). Pulmonary function test and DLCO of our patient were normal, possibly due to localized segmental involvement.
Clinically significant lung involvement of Crohn?s disease is rare, but quite variable. Respiratory system may be affected from upper airway to alveoli. The large airways are the most common location of IBD involvement (2,12,13). Stridor may be a presenting symptom due to subglottic inflammation and stenosis. Tracheobronchitis with or without upper airway obstruction and laryngitis in different studies as pulmonary involvement of Crohn?s disease have been shown (2,12,13,14). Severe tracheobronchial stenosis in a case was also reported by Kuzniar et al. (15). All these patients with upper airway disease responded dramatically to oral or inhaled steroid treatment.
Bronchiectasis is mostly known pulmonary manifestation of IBD involving large airways. Acute or chronic bronchitis, suppurative airway disease may also be seen as large airway disease in IBD patients. Surprisingly, a high proportion of these patients are non-smokers (6,16).
Unlike other forms of lung involvement, small airway involvement in IBD commonly starts before gastrointestinal symptoms as in our case. Pathologically, although bronchiolitis and peribronchial granuloma formation are fairly common, endobronchial polypoid lesion at segmental level has not been reported before our case.
Interstitial lung involvement has been reported to accompany both clinical IBD entities, Ulcerative colitis and Crohn?s disease (17). In addition to bronchial eosinophilic infiltration, pulmonary infiltrates with eosinophilia, nonspesific interstitial pneumonia, desquamative interstitial pneumonitis also were reported as pulmonary involvement of IBD (2,18). Treatment with corticosteroids or with appropriate medication such as sulfasalazine or mesalamine for the basic gastrointestinal disease appeared to be satisfactory for both diseases. Pneumonitis, in contrast, due either to sulphasalazine or mesalamine is a well-recognized adverse drug reaction in these patients (19).
Infrequently, Crohn?s disease may present as sterile multiple necrobiotic nodules even though the disease was in remission with mesalazine treatment (20).
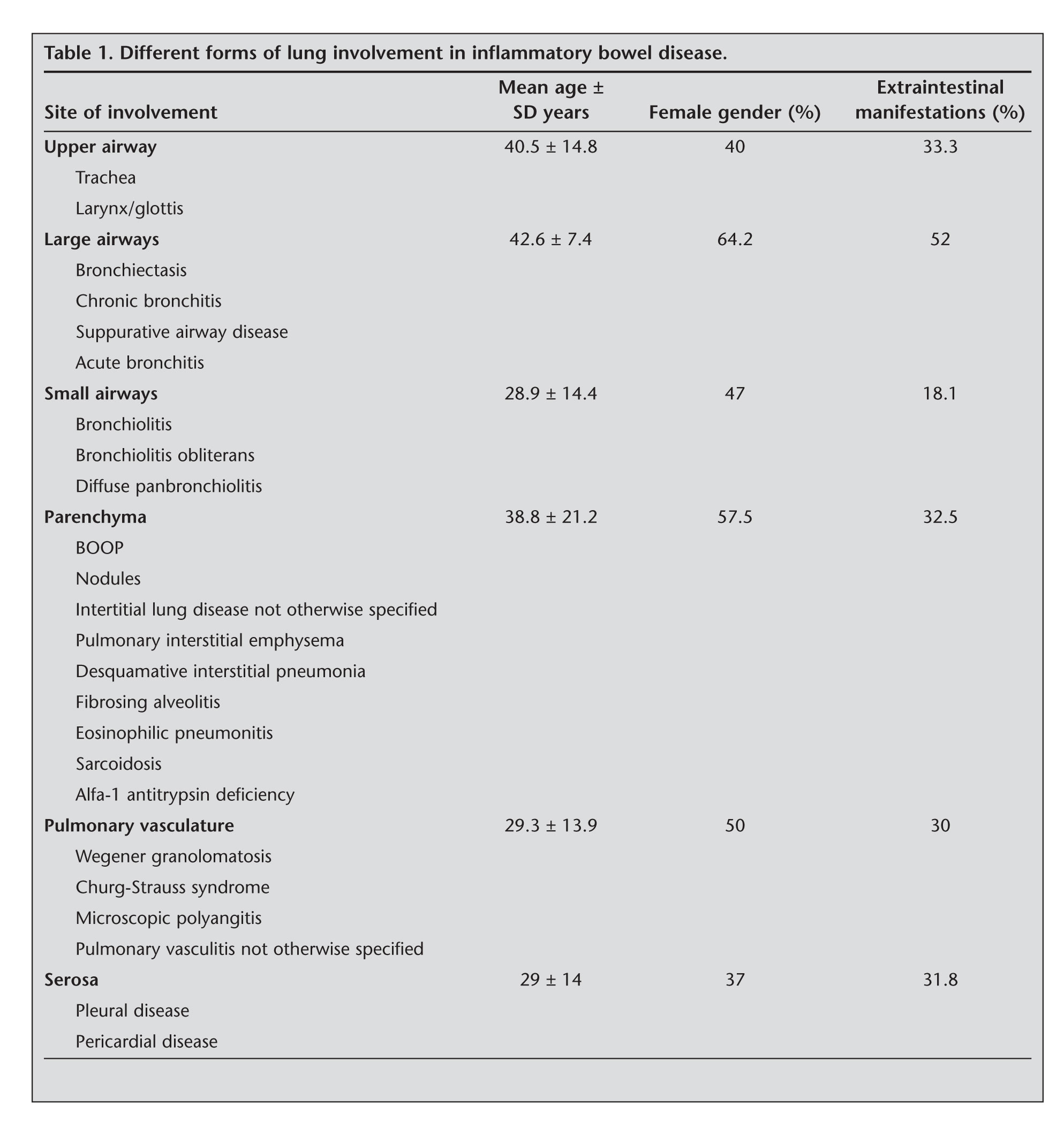
Pleura may also be affected in IBD, but rarely. Pleural involvement is almost always unilateral and pleural fluid is usually exudative in nature (21). Pleural fibrosis has also been reported in a patient with Crohn?s disease (22). Colobronchial fistula is another rare complication of Crohn?s colitis. Different forms of pulmonary involvement in IBD were presented in Table 1 (7).
In conclusion; Crohn?s disease may involve respiratory system in variable forms, even as endobronchial lesion. In differential diagnosis of almost all pulmonary diseases including benign endobronchial polypoid lesions, the patient?s history about gastrointestinal symptoms should be evaluated carefully Crohn?s disease should be considered.
ACKNOWLEDGEMENT
The authors would like to express their appreciations to Dear Gulten Ortac for proofreading.
CONFLICT of INTEREST
None declared.
REFERENCES
- Dagl? U. Inflammatory bowel disease: epidemiology, risk factors and genetic. Turkish Clinics J Gastroenterohepatol-Special Topics 2009; 2: 1-6.
- Camus P, Piard F, Ashcroft T, Gal AA, Colby TV. The lung in inflammatory bowel disease. Medicine (Baltimore) 1993; 72: 151-83. [?zet]
- Turner-Warwick M. Fibrosing alveolitis and chronic liver disease. Q J Med 1968; 37: 133-49.
- Bamias G, Nyce MR, De La Rue SA, Cominelli F. New concepts in the pathophysiology of inflammatory bowel disease. Ann Intern Med 2005; 143: 895-904.
- Eade OE, Smith CL, Alexander JR. Pulmonary function in patients with inflammatory bowel disease. Am J Gastroenterol 1980; 73: 154-6. [?zet]
- Heatley RV, Thomas P, Prokipchuk EJ, Gauldie J, Sieniewicz DJ, Bienenstock J. Pulmonary function abnormalities in patients with inflammatory bowel disease. Q J Med 1982; 51: 241-50.
- Tzanakis NE, Tsiligianni IG, Siafakas NM. Pulmonary involvement and allergic disorders in inflammatory bowel disease. World J Gastroenterol 2010; 16: 299-305. [?zet] [Tam Metin] [PDF]
- Bonni?re P, Wallaert B, Cortot A, Marchandise X, Riou Y, Tonnel AB, et al. Latent pulmonary involvement in Crohn?s disease: biological, functional,bronchoalveolar and scintigraphic studies. Gut 1986; 27: 919-25. [?zet] [PDF]
- Tzanakis N, Bouros D, Samiou M, et al. Lung function in patients with inflammatory bowel disease. Respir Med 1998; 92: 516-522. [?zet]
- Douglas JG, McDonald CF, Leslie MJ, Gillon J, Crompton GK, Mc Hardy GJR. Respiratory impairment in inflammatory bowel disease. Does it vary with disease activity? Respir Med 1989; 83: 389-94. [?zet]
- Valetta E, Bertini M, Sette L, Braggion C, Pradal U, Zannoni M, et al. Early bronchopulmonary involvement in Crohn disease: a case report. BMC Gastroenterology 2001; 1: 13-8. [?zet] [Tam Metin] [PDF]
- Garg K, Lynch DA, Newell JDD. Inflammatory airways disease in ulcerative colitis: CT and high-resolution CT features. J Thorac Imaging 1993; 8: 159-63. [?zet]
- Iwama T, Higuchi T, Imajo M, Akagawa S, Matsubara O, Mishima Y. Tracheo-bronchitis as a complication of Crohn?s disease. A case report. Jap J Surg 1991; 21: 454-7. [?zet]
- Kuzniar T, Sleiman C, Brugi?re O, Groussard O, Mal H, Mellot F, et al. Severe tracheobronchial stenosis in a patient with Crohn?s disease. Eur Respir J 2000; 15: 209-12. [?zet] [PDF]
- Kelly JH, Montgomery WW, Goodman ML, Mulvaney TJ. Upper airway obstruction associated with regional enteritis. Ann Otol Rhinol Laryngol 1979; 88: 95-9. [?zet]
- Fireman Z, Osipov A, Kivity S, Kopelman Y, Sternberg A, Lazarov E, et. al. The use of induced sputum in the assessment of pulmonary involvement in Crohn?s disease. Am J Gastroenterol 2000; 95: 730-4. [?zet]
- Louis E, Louis R, Shute J, Lau L, Franchimont D, Lamproye A, et al. Bronchial eosinophilic infiltration in Chron?s disease in the absence of pulmonary disease. Clin Exp Allergy 1999; 29: 660-6. [?zet]
- Camus P, Colby TV. The lung in inflammatory bowel disease. Eur Respir J 2000; 15: 5-10. [PDF]
- Golpe R, Mateos A, Valcarcel JP, et al. Multiple pulmonary nodules in a patient with Crohn?s disease. Respiration 2003; 70: 306-9. [?zet]
- Lemann M, Messing B, D?Agay F, Modigliani R. Chron?s disease with respiratory tract involvement. Gut 1987; 28: 1669-72. [?zet] [PDF]
- Faller M, Gasser B, Massard G, Pauli G, Quoix G. Pulmonary migratory infiltrates and pachypleuritis in a patient with Crohn?s disease. Respiration 2000; 67: 459-63. [?zet]
- Melisch B, Schaflinger E, Smolle-Jutner FM, Schalck V, Ratschek M. Colobronchial fistula: a rare complication of Crohn?s colitis. Am Rev Respir Dis 1990; 142: 1225-7. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Evrim Eylem AKPINAR,
Ufuk ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
Konya Yolu No: 88/86 Balgat, Ankara - TURKEY
e-mail: drevrimeylem@gmail.com