Dev mediastinal paratiroid adenoma
H?seyin ?AKMAK1, Arif Osman TOKAT2, Sezgin KARASU2, Murat ?ZKAN3
1 SB Ankara Onkoloji E?itim ve Ara?t?rma Hastanesi, G???s Cerrahisi Klini?i,Ankara,
2 SB Ankara E?itim ve Ara?t?rma Hastanesi, G???s Cerrahisi Klini?i,Ankara,
3 Ankara ?niversitesi T?p Fak?ltesi, ?bn-i Sina Hastanesi, G???s Cerrahisi Anabilim Dal?, Ankara.
?ZET
Dev mediastinal paratiroid adenoma
Paratiroid adenomlar ve paratiroid hiperplazisi primer hiperparatiroidizmin en s?k g?r?len sebepleridir. Paratiroid adenomlar seyrek olarak ?ok b?y?k boyutlara ula??r. Burada mediasten yerle?imli kitle ve hiperkalsemi saptanan 63 ya??ndaki kad?n hasta sunulmaktad?r. Olguda ektopik hipersekretuar paratiroid adenomuna ba?l? y?ksek intakt parathormon seviyesi saptand? (642 pg/mL). Kesin histolojik tan? paratiroid adenoma olarak rapor edildi. Olgudaki paratiroid adenomu 7 x 5 x 4 cm boyutlar? ve 145 g a??rl??? ile literat?rdeki en b?y?k kitle idi. Kitle dev boyutlar?na ra?men hiperkalsemi semptomlar?na yol a?mam??t?.
Anahtar Kelimeler: Mediasten, hiperkalsemi, paratiroid adenomu.
SUMMARY
Giant mediastinal parathyroid adenoma
H?seyin ?AKMAK1, Arif Osman TOKAT2, Sezgin KARASU2, Murat ?ZKAN3
1 Clinic of Chest Surgery, Ankara Oncology Training and Research Hospital,Ankara, Turkey,
2 Clinic of Chest Surgery, Ankara Training and Research Hospital, Ankara, Turkey,
3 Department of Chest Surgery, Ibn-i Sina Hospital, Faculty of Medicine, Ankara University, Ankara, Turkey.
Primary hyperparathyroidism is most commonly caused by either a parathyroid adenoma or parathyroid hyperplasia. Parathyroid adenomas also rarely attain huge proportions. We present a case of a 63-year-old female patient causing hypercalcemia and the mass which is located in the mediastinum. High intact parathormone level secondary to an ectopic hypersecretory parathyroid adenoma were detected (642 pg/mL). It was removed via a right thoracic approach. In this case parathyroid adenoma measuring 7 x 5 x 4 cm and weighing 145 g; to our knowledge the greatest mass reported in the literature. Despite its huge size it did not cause many of the hypercalcemic symptoms.
Key Words: Mediastinum, hypercalcemia, parathyroid adenoma.
Primary hyperparathyroidism is most commonly caused by either a parathyroid adenoma or parathyroid hyperplasia. Giant parathyroid adenomas are very rare (1). We present a case of severe hypercalcemia and very high intact parathormone level secondary to an ectopic hypersecretory huge parathyroid adenoma. Despite its huge size it did not cause many of the hypercalcemic symptoms usually associated with large adenomas.
CASE REPORT
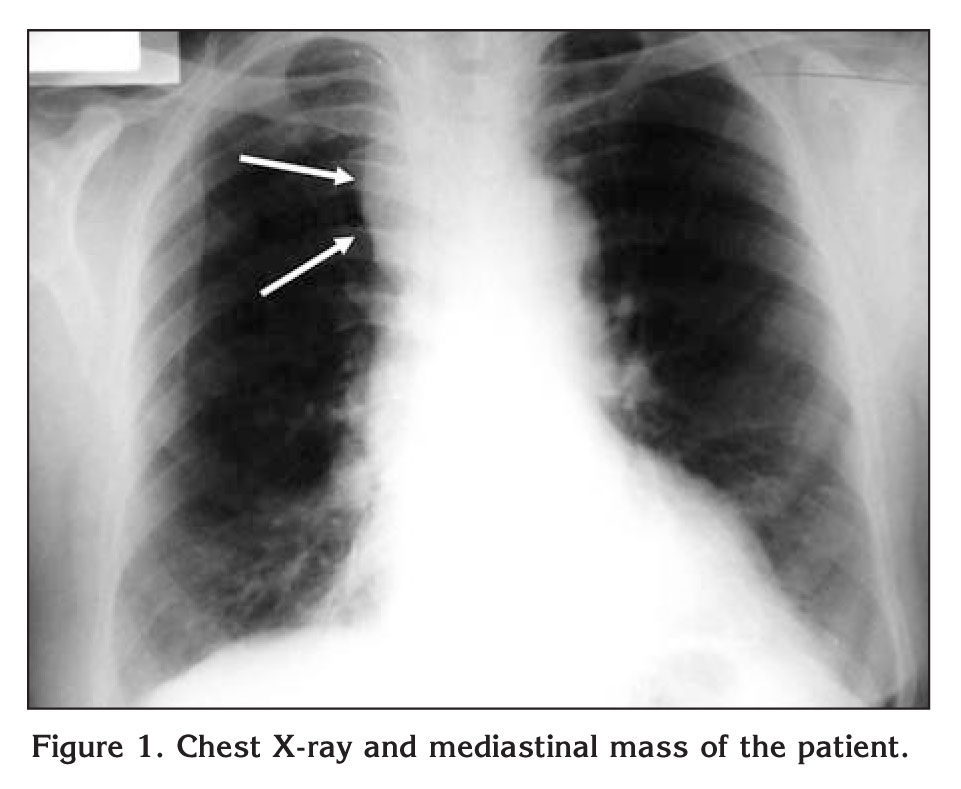
A 63-year-old woman visited her physician because of 3-months history of headache and fatigue. She denied changes in her voice, dyspnea, dysphagia, or musculoskeletal pain. There was no relevant medical or family history. Physical examination was normal. Abnormal calcium and phosphate levels were detected in blood analysis and abnormal right upper mediastinal shadow on chest x-ray film was detected (Figure 1).
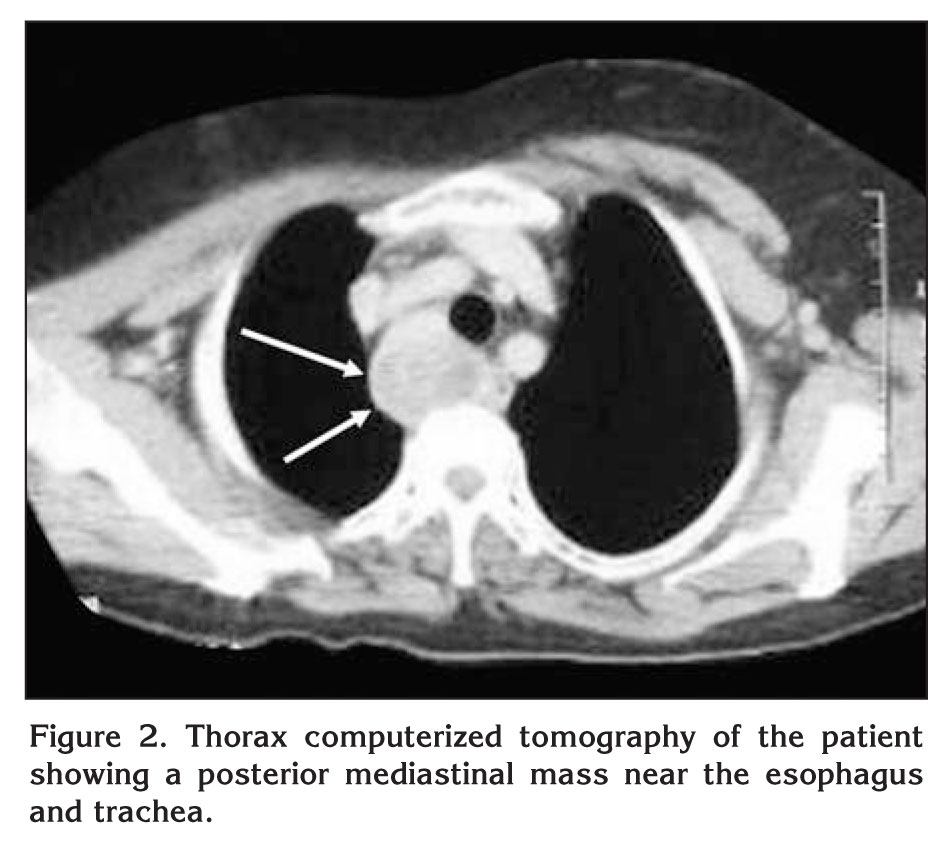
The patient was referred to the thoracic surgery department for further evaluation of mediastinal mass causing hypercalcemia. Her serum calcium and phosphorus levels were 13.2 mg/dL and 2.5 mg/dL, respectively. Intact parathormone level was 642 pg/mL (normal range 8 to 97 pg/dL). A technetium-99m pertechnetate methoxy-isobutyl-isonitrite (Tc-99 m MIBI) scan was revealed a mass in the mediastinum. Computed tomography (CT) revealed a heterogeneous hypodense right paratracheal mass compressing esophagus (Figure 2). A fine needle aspiration under CT guidance did not yield tumor cells. The thyroid gland appeared normal and no other pathologic lesion was found on USG and scintigraphy.
The right posterolateral thoracotomy was performed with a double-lumen endotracheal tube for single lung ventilation. The mass approximately 10 cm width was revealed at the posterior mediastinum. The vascular pedicle of the mass originated in the mediastinum. It was freed from the surrounding tissue and excised. The specimen was measured 7 x 5 x 4 cm in dimensions and weighing 145 g. The thoracostomy tube was removed on the first post-operative day, and there were no surgical complications. Postoperative serum calcium levels dramatically decreased to the levels of 6 mg/dL, and she was supported with oral calcium and vitamin D. The histopathological diagnosis confirmed the lesion as parathyroid adenoma. Intact parathormone level was 47 pg/mL on the postoperative day 12.
DISCUSSION
Parathyroid tumors are usually located on the posterior capsule of the thyroid but may be in other ectopic locations (1). Parathyroid glands are known to be occurring in aberrant locations, mainly in the throid parenchyma and less commonly in the mediastinum (2). An enlarged gland can descend into the mediastinum because of its increased weight as a result of intrathoracic negative pressure and esophageal movement (3). The inferior parathyroids, derived from the 3rd branchial pouch along with the thymus, have a more variable position. Less than two thirds are found close to the lower pole of the thyroid but the remainder are usually found within the thyrothymic ligament or in the mediastinum (4).
Ectopic locations is indoubtedly related to the migratory pathways of embriologic parathyroid tissue to the adult positions. Within these migratory pathways of parathyroid tissue, rare locations have been found as cephalad as carotid artery bifurcations (undescended parathyroid glands) and as caudal as pericardium (2). The mediastinum is the most frequent location for ectopic parathyroid tumors, with approximately 20% of parathyroid tumors located in the mediastinum (1).
70% of the ectopic parathyroid glands are located in the thymus. They can be removed through a cervical approach with or without a sternotomy. Rarely, the ectopic glands located deep in the mediastinum require a thoracotomy for removal including that in the present case, can not be extracted through a cervical approach because the glands are located deep in the posterior mediastinum, aortopulmonary window, and pericardium (5,6).
It has been found that an increased glandular mass correlates with the severity of primary hyperparathyroidism and the subsequent risk of transient postoperative hypocalcemia (7). Because of the high secretory output, as measured by intact parathormone levels the major proportion of this enlarged gland was probably hypereractive because of its increased cellularity.
Giant parathyroid adenomas are very rare. The usual weight of a parathyroid adenoma ranges from 1 to 70 mg. Only there are sporadic reports of tumors were reported weighing more than 20 g (2). Giant parathyroid adenomas are extremely rare. There are sporadic reports of large adenomas attaining masses of 70 g (8). The most frequent etiological association being that seen with irradiation, for example, in survivors of the atomic bomb (9).
Power et al. were reported a giant parathyroid adenoma at 2005 which measuring 8 x 5 x 3.5 cm and weighing 110 g. They claimed that it was the greatest in the literature. In our case parathyroid adenoma measuring 7 x 5 x 4 cm and weighing 145 g is the greatest mass reported in the literature in our knowledge. Extremely high intact parathormone level was detected secondary to an ectopic hypersecretory huge parathyroid adenoma. Despite its huge size and high intact parathormone levels it did not cause of the hypercalcemic symptoms which also makes this case noteworthy.
CONFLICT of INTEREST
None declared.
REFERENCES
- Fortson JK, Patel VG, Henderson VJ. Parathyroid cysts: a case report and review of the literature. Laryngoscope 2001; 111: 1726-8. [?zet]
- Power C, Kavanagh D, Hill AD, O'Higgins N, McDermott E. Unusual presentation of a giant parathyroid adenoma: report of a case. Surg Today 2005; 35: 235-7. [?zet]
- Knight R, Ratzer ER, Fenoglio ME, Moore JT. Thoracoscopic excision of mediastinal parathyroid adenomas: a report of two cases and review of the literature. J Am Coll Surg 1997; 185: 481-5. [?zet]
- Butterworth PC, Nicholson ML. Surgical anatomy of the parathyroid glands in secondary hyperparathyroidism. J R Coll Surg Edinb 1998; 43: 271-3. [?zet]
- Prinz RA, Lonchyna V, Carnaille B, Wurtz A, Proye C. Thoracoscopic excision of enlarged mediastinal parathyroid glands. Surgery 1994; 116: 999-1005. [?zet]
- Wang C, Gaz RD, Moncure AC. Mediastinal parathyroid exploration: a clinical and pathological study of 47 cases. World J Surg 1986; 10: 687-95.
- Zamboni WA, Folse R. Adenoma weight: a predictor of transient hypocalcemia after parathyroidectomy. Am J Surg 1986; 152: 611-5. [?zet]
- Tsuchiya A, Endo S, Abe R. Giant adenoma of the parathyroid: report of a case. Surg Today 1993; 23: 465-7. [?zet]
- Takeichi N, Nishida T, Fujikura T, Hiraoka T, Wakabayashi T, Yotsumoto I, et al. Two cases of large functioning parathyroid adenomas in atomic bomb survivors. Gan No Rinsho 1983; 29: 851-4. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Arif Osman TOKAT,
SB Ankara E?itim ve Ara?t?rma Hastanesi,
G???s Cerrahisi Klini?i,
06340 ANKARA - TURKEY
e-mail: aostokat@hotmail.com