Varikosel
operasyonundan sonra geli?en ve etyolojisi izah edilemeyen
bir akut solunum
s?k?nt?s? sendromu olgusu
Turgut TEKE, Emin MADEN, Celalettin KORKMAZ, Rukiye MET?NEREN, K?r?at UZUN
Sel?uk ?niversitesi Meram T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Konya.
?ZET
Varikosel operasyonundan sonra geli?en ve etyolojisi izah edilemeyen bir akut solunum s?k?nt?s? sendromu olgusu
Akut solunum s?k?nt?s? sendromu (ARDS) do?rudan ve dolayl? akci?er hasar?n? i?eren bir?ok klinik bozuklukla ili?kili ani bir solunum yetmezli?i sendromudur. Vask?ler cerrahi ge?iren hastalar ARDS a??s?ndan risk alt?ndad?r. Yirmi ?? ya??ndaki erkek hasta epidural anestezi alt?nda bir saat s?ren varikosel operasyonundan hemen sonra ani olarak geli?en nefes darl???, siyanoz ve ajitasyon ?ikayetleriyle yo?un bak?m ?nitesine yat?r?ld?. Epidural anestezi i?in bupivakain, fentanil, remifentanil ve midazolam kullan?lm??t?. Hastan?n oksijen sat?rasyonu? FiO2 0.5 iken %81 idi. Arteryel kan gazlar?nda hipoksemi ile birlikte respiratuar alkalozu vard? ve PaO2/FiO2 oran? 100 idi. Akci?er grafisinde bilateral alveoler opasiteler izlendi. Yatak ba?? yap?lan ekokardiyografisinde sol ventrik?l ejeksiyon fraksiyonu %65 ?l??ld?. ARDS tan?s? konularak hastaya noninvaziv mekanik ventilasyon (NIMV) tedavisi ba?land?. D?rd?nc? g?nde NIMV tedavisi ba?ar?l? bir ?ekilde sonland?r?larak hasta taburcu edildi. Bu olgu sunumunda epidural anestezi alt?nda varikosel operasyonundan hemen sonra geli?en, etyolojisi tam olarak izah edilemeyen ve NIMV ile ba?ar?l? bir ?ekilde tedavi edilen bir ARDS olgusu sunulmu?tur.
Anahtar Kelimeler: ARDS, epidural anestezi, noninvaziv mekanik ventilasyon, vask?ler cerrahi.
SUMMARY
Unexplained acute respiratory distress syndrome after varicocele surgery; report of a case
Turgut TEKE, Emin MADEN, Celalettin KORKMAZ, Rukiye MET?NEREN, K?r?at UZUN
Department of Chest Diseases, Faculty of Meram Medicine, Selcuk University, Konya, Turkey.
Acute respiratory distress syndrome (ARDS) is a syndrome of acute respiratory failure that is associated with several clinical disorders including direct pulmonary injury and indirect pulmonary injury. Vascular surgical patients are at risk for ARDS. A 23-year old man was admitted to our respiratory intensive care unit with short of breath, cyanosis and agitation which was developed acutely after varicocele operation under epidural anesthesia lasted for one hour. Bupivacain, fentanyl, remifentadyl and midazolam were used for epidural anesthesia. Oxygen saturation was 81% while breathing oxygen at FiO2 of 0.5. Arterial blood gas analysis showed hypoxemia with respiratory alkalosis with a PaO2/FiO2 score of 100. A chest radiograph demonstrated bilateral alveolar opacities. Bedside echocardiography was performed which revealed no evidence of global hypokinesia, all the chambers were normal, left ventricular ejection fraction was 65%. A diagnosis of ARDS was made and the patient was initiated on noninvasive mechanical ventilation. He was gradually weaned off the NIMV and discharged after a total hospital stay of four days. We report an ARDS case due to unexplained etiology after varicocele operation under epidural anesthesia and managed successfully with noninvasive mechanical ventilation.
Key Words: ARDS, epidural anesthesia, noninvasive mechanical ventilation, vascular surgery.
Acute respiratory distress syndrome (ARDS) is a syndrome of acute respiratory failure that is associated with several clinical disorders including direct pulmonary injury from pneumonia and aspiration as well as indirect pulmonary injury from trauma, sepsis, and other disorders such as acute pancreatitis and drug overdose (1,2). Overdosing of several drugs, such as tricyclic antidepressants, salicylates, and opiates, is known to induce effects like those seen in patients with adult respiratory distress syndrome (3).
On the other hand, vascular surgical patients are at risk for ARDS. Pulmonary edema is known to occur after vascular procedures in which tissue ischemia occurs. Reperfusion of dysoxic muscle causes pulmonary inflammation during vascular surgery (4).
The role for noninvasive ventilation in ARDS is less clear. A growing number of small studies suggest that bilevel noninvasive ventilation may reduce the need for intubation and improve outcomes in selected patients with early ARDS (5).
Herein, we report an ARDS case due to unexplained etiology after varicocele operation under epidural anesthesia and managed successfully with noninvasive mechanical ventilation (NIMV).
CASE REPORT
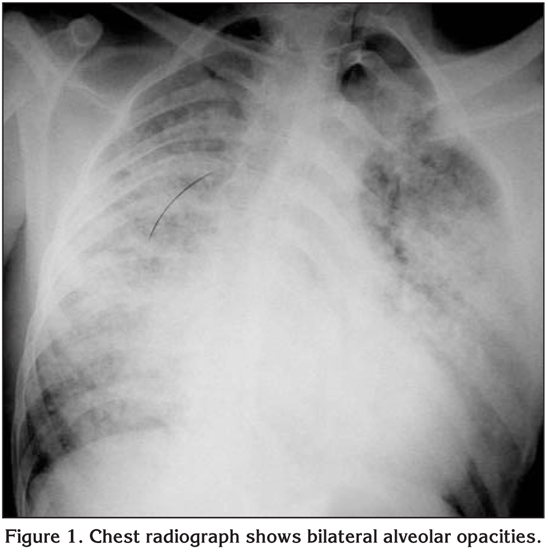
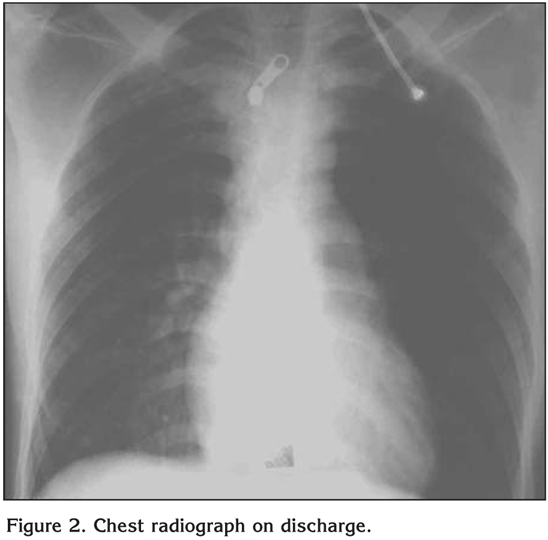
A 23-year old man was admitted to our respiratory intensive care unit with short of breath, cyanosis and agitation which was developed acutely after varicocele operation under epidural anesthesia lasted for one hour. Bupivacain, fentanyl, remifentadyl and midazolam were used for epidural anesthesia. There was no blood transfusions history of patient. On admission his temperature was 38?C, heart rate 117 was beats/minute, respiratory rate was 48 breaths/minute and blood pressure was 110/70 mmHg. He was tachypneic, agitated and cyanotic. Bilateral ralles were heart during auscultation and tachycardia was present. The rest of the physical examination was unremarkable. His blood count and biochemical analysis were normal. Oxygen saturation was 81% while breathing oxygen at FiO2 of 0.5. Arterial blood gas analysis showed hypoxemia with respiratory alkalosis with a PaO2/FiO2 score of 100. A chest radiograph demonstrated bilateral alveolar opacities consistent with ARDS (Figure 1). An electrocardiogram showed sinus tachycardia. Bedside echocardiography was performed which revealed no evidence of global hypokinesia, all the chambers were normal, left ventricular ejection fraction was 65%. The right atrium and right ventricle were normal with minimal tricuspid regurgitation. A diagnosis of ARDS was made and the patient was initiated on NIMV (BiPAP, Respironics, Inc, Murrysville, PA, ABD) with an expiratory/inspiratory positive airway pressure of 4/10 cmH2O with a FiO2 of 0.5. Over the next hour, there was partially improvement in oxygen saturation, respiratory rate and arterial blood gas parameters. PaO2/FiO2 score was calculated 116. He was continued with an expiratory/inspiratory positive airway pressure of 5/12 cmH2O with a FiO2 of 0.7. After 48 hours of continuous ventilation (with short breaks for daily activities), there was a significant improvement in the PaO2/FiO2 score and radiographic findings (Figure 2). PaO2/FiO2 score was calculated 213. He was gradually weaned off the NIMV and discharged after a total hospital stay of four days. Nonspecific antibiotic was continued for four days. At a one-week follow up, he was asymptomatic and his chest radiography was normal.
DISCUSSION
ARDS is a clinically complex picture with various etiologies and therapeutic consequences. In our patient, we could not explain etiology of ARDS, but we suspected of two reason. The two causes that might lead to the ARDS were the drug toxicity and the vascular surgery. There was no known precipitating condition for ARDS in our patient, such as blood transfusion or aspiration. There is limited information on the mechanism(s) of drug induced ARDS. One of the well known examples of drug toxicity is tricyclic antidepressant-induced ARDS. Several case reports on tricyclic antidepressant-induced ARDS have been published. Amitriptyline and likely other tricyclic antidepressants induce ARDS, probably by increasing endothelial permeability due to impaired tight junction function mediated by way of intracellular calcium changes (6). Our patient received fentanyl during epidural anesthesia. In a study evaluating the cause of unexplained postoperative ARDS, Goetz et al. showed that fentanyl infusion was administered in 6 cases underwent vascular surgery and developed postoperative unexplained ARDS (7). In the same study it was reported that none of the 17 control cases underwent the same procedure, but not developed ARDS received fentanyl infusion.
Our patient had varicocele operation as a vascular surgery. Vascular surgical patients are at a risk for ARDS. This operation is recognized to produce partial ischemia of the lower extremities, and has been reported to result in acute pulmonary edema after declamping, presumably on the basis of a reperfusion injury to the lower extremities (4). Paterson et al. observed increased pulmonary shunt and radiographic evidence of pulmonary edema within 4 hrs after surgery. The etiology of lung injury in patients undergoing vascular surgery is complex, and factors other than transfusion are involved. The effect of ischemia-reperfusion is thought to activate neutrophils, trigger a systemic inflammatory response, and in turn lead to an increase in pulmonary capillary permeability (8).
We treated our ARDS case with NIMV successfully. The selection of patients with ARDS to receive NIMV is challenging. Although NIMV has been used to treat acute respiratory failure due to exacerbations of chronic obstructive pulmonary disease, cardiogenic pulmonary edema or in immunocompromised hosts, its appropriate use to treat hypoxemic respiratory failure remains unclear (9). ARDS represents the most severe form of hypoxemic acute respiratory failure. In three randomized studies that among patients with ARDS, NIMV avoided intubation in more than 50% (10). Overall, the findings of these studies invite a prudent approach, limiting the application of NPPV to selected patients who can be closely monitored in the ICU where endotracheal intubation is promptly available. For this reason, we applied NIMV, under close ICU observation, with close clinical and laboratory monitoring.
In conclusion, it should be remembered that ARDS may develop in post operative period after vascular surgery or epidural fentanyl administration and these ARDS cases could be treated successfully with NIMV.
CONFLICT of INTEREST
None declared.
REFERENCES
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342: 1334-49.
- Matthay MA, Zimmerman GA, Esmon C, Bhattacharya J, Coller B, Doerschuk CM, et al. Future research directions in acute lung injury: summary of a National Heart, Lung, and Blood Institute working group. Am J Respir Crit Care Med 2003; 167: 1027-35. [?zet] [Tam Metin] [PDF]
- Dahlin KL, L?stbom L, Blomgren B, Ryrfeldt A. Acute lung failure induced by tricyclic antidepressants. Toxicol Appl Pharmacol 1997; 146: 309-16. [?zet]
- Paterson IS, Klausner JM, Pugatch R, Allen P, Mannick JA, Shepro D, et al. Noncardiogenic pulmonary edema after abdominal aortic aneurysm surgery. Ann Surg 1989; 209: 231-6. [?zet]
- Agarwal R, Reddy C, Aggarwal AN, Gupta D. Is there a role for noninvasive ventilation in acute respiratory distress syndrome? A meta-analysis. Respir Med 2006; v100: 2235-8. [?zet]
- Ryrfeldt A. Drug-induced inflammatory responses to the lung. Toxicol Lett 2000; 112-3: 171-6. [?zet]
- Goetz AM, Rogers PL, Schlichtig R, Muder RR, Diven WF, Prior RB. Adult respiratory distress syndrome associated with epidural fentanyl infusion. Crit Care Med 1994; 22: 1579-83. [?zet]
- Wright SE, Snowden CP, Athey SC, Leaver AA, Clarkson JM, Chapman CE, et al. Acute lung injury after ruptured abdominal aortic aneurysm repair: the effect of excluding donations from females from the production of fresh frozen plasma. Crit Care Med 2008; 36: 1796-802. [?zet]
- Erik Garpestad, Nicholas S Hill. Noninvasive ventilation for acute lung injury: how often should we try, how often should we fail? Crit Car 2006; 10: 147. [?zet] [Tam Metin] [PDF]
- Antonelli M, Conti G, Esquinas A, Montini L, Maggiore SM, Bello G, et al. A multiple-center survey on the use in clinical practice of noninvasive ventilation as a first-line intervention for acute respiratory distress syndrome. Crit Care Med 2007; 35: 18-25. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Turgut TEKE,
Sel?uk ?niversitesi Meram T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?, Meram,
KONYA - TURKEY
e-mail: turgutteke@hotmail.com