Nadir bir yabanc? cisim aspirasyonu ve literat?re bak??
Ekrem ?ENT?RK, Serdar ?EN
Adnan Menderes ?niversitesi T?p Fak?ltesi, G???s Cerrahisi Anabilim Dal?, Ayd?n.
?ZET
Nadir bir yabanc? cisim aspirasyonu ve literat?re bak??
Trakeobron?iyal yabanc? cisim aspirasyonlar?, her ya? grubunda g?r?lebilen, acil tan? ve m?dahale gerektiren bir sa?l?k problemidir. Yabanc? cisim aspirasyonlar?n?n hi?bir klinik bulgu olmayabilece?i gibi ?ks?r?k, nefes darl???, hemoptizi ve solunumsal arreste varan geni? bir semptom marj? vard?r. Yedi y?l ?nce skuamoz h?creli karsinoma tan?s?yla total larenjektomi ge?iren 72 ya??ndaki erkek olgu, trakeostomi kan?l?n?n nefes borusuna ka?mas? ?ikayetiyle acil servise ba?vurmu?tu. Fizik muayene ve akci?er grafisinde hi?bir bulgu saptanamayan olgu; anamnezindeki g?vensizlik nedeniyle acil hekimi ve kons?lte eden g???s hastal?klar? hekimi taraf?ndan acil m?dahale gerekmedi?i, yan?lm?? olabilece?i s?ylenerek poliklinik kontrol? ?nerilerek taburcu edilmi?ti. Ertesi g?n g???s cerrahisi poliklini?inde fizik muayene ve akci?er grafisi ile de?erlendirilen olguda patoloji saptanmad?. Ancak ?ekilen toraks bilgisayarl? tomografisinde sol ana bron?ta bron?un ?eklini alan ve obstr?ksiyona neden olmayan kan?l saptand?. Sedoanaljezi e?li?inde rijid bronkoskopi ile kan?l forseps yard?m?yla ??kar?ld? ve olgu ertesi g?n sorunsuz taburcu edildi. Sonu? olarak; etyoloji ve patogenezin bilinmesi olguya yakla??m zaman? ve ?eklini belirlemede yararl?d?r. Yabanc? cisim ??phesi olan olguda muayene ve akci?er bulgular? yeterli olmayabilir, toraks bilgisayarl? tomografi ve tan? konam?yorsa bronkoskopi mutlaka yap?lmal?d?r. Fleksibl bronkoskopi tan?sal ama?l? kullan?labilmekte, k???k ve uygun yabac? cisimlerin ??kar?lmas?nda ?ncelikli olmaktad?r. ?ocuklarda, komplike olgularda, penetran veya amorf ?ekilli yabanc? cisimlerin ??kar?lmas?nda rijid bronkoskopi se?ilmelidir.
Anahtar Kelimeler: Yabanc? cisim aspirasyonu, trakeostomi kan?l?, fleksibl bronkoskopi, rijid bronkoskopi.
SUMMARY
An unusual case of foreign body aspiration and review of the literature
Ekrem ?ENT?RK, Serdar ?EN
Department of Chest Surgery, Faculty of Medicine, Adnan Menderes University, Aydin, Turkey.
Tracheobronchial foreign body aspiration is a health problem that can be seen in all age groups, and it requires urgent diagnosis and intervention. We report a case of an unusual foreign body aspiration in a laryngectomized patient and we aim to discuss this situation according to the literature. A 72-year-old man, who underwent total laryngectomy 7 years ago for a squamous cell carcinoma of the larynx, was reported with complaint of aspiration of a silicone tracheostomy canula. Foreign body aspiration can present with a wide variety of symptoms. Although it is sometimes asymptomatic, mostly there exists cough, dispnea, hemoptisis and even respiratory arrest. Clinical history and radiological examinations are enough for the diagnose but in some cases, it is difficult to diagnose even by bronchoscopy. In this report, ethiology, pathogenesis, clinical presentation, diagnose and treatment of foreign body aspirations are discussed under the light of the literature. Ethiology and pathogenesis are beneficial for the assessment of treatment time and method. Appropriate and ontime clinical intervention makes the diagnosis to be easier. Treatment timing and methods are important to prevent the complications. Flexible bronchoscopy can be used for the diagnose and is preferential to remove small and fit foreign bodies. For children, for complicated cases and in order to remove penetrating or amorph-shaped bodies rigit bronchoscopy should be preferred.
Key Words: Foreign body, flexible bronchoscopy, rigit bronchoscopy, tracheostomy canula.
Tracheobronchial foreign body aspiration can be seen in all age groups but it is mostly seen in childhood and can be a fatal problem (1,2,3). In these cases, it is very important to diagnose rapidly and to remove the foreign body safely (4).
Although recently, advanced methods are used to remove the foreign bodies, foreign body aspiration is still an important health problem that it is mortal in more than 3000 cases per year and has complications with different sequelas (5).
FBA accounted for 7% of all accidental deaths in children under 4 years of age in the US during the year 1986. About 75% to 85% of all FBAs occur in children younger than 15 years old; however, most are younger than 3 years of age (6). Boys are affected more frequently than girls (7).
In our study, we reported an unusual foreign body aspiration case with difficult diagnosis. We aimed to discuss this laryngectomised patient according to the literature.
CASE REPORT
A 72-year-old man, who underwent total laryngectomy 7 years ago for a squamous cell carcinoma of the larynx, was admitted to emergency service with complaint of aspiration of a silicone tracheostomy canula. He was in a habit of cleaning secretions of the upper airway, with his finger via tracheostomy. However, at this time the tracheostomy canula has slipped into the trachea. The patient was admitted to emergency department. But he has not got any symptomps.
So the emergency doctors did not believe him. He had no abnormal sonority in both lungs at physical examination. He did not have fever showing signs of infection and he was very calm. The chest X-ray was normal (Figure 1). And the emergency doctor has convinced him that he didn't have any problems.
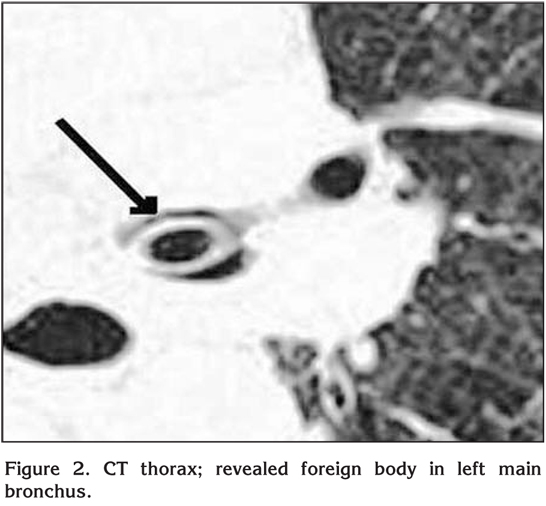
He applied to thoracic surgeon policlinic the day after. Physical examination and X-ray was normal again. But CT of the thorax revealed foreign body in left main bronchus (Figure 2). This foreign body was seen as long tube in his left main bronchus. But it was not blocking the air-way passage. A topical aerolized lidocaine spray and sedoanalgesia was performed to the patient. The trachea and left main bronchus was observed by RB. The tracheostomy canula had taken the shape of the left main bronchus. The forceps had been introduced through the RB to grasp gently the object for retrieval. Therefore, the RB, forceps and the tracheostomy canula were removed as a single unit. It was quite surprising to discover the silicone tracheostomy canula (Figure 3). The patient tolerated the procedure unexpectedly well and was discharged the following day.

DISCUSSION
Most of the foreign body aspiration patients apply to the hospital in first six hours after aspiration. The knowledge and experience of the doctors to whom the patient applies is very critical.
The type of foreign body aspirated differs according to countries. Some studies from USA and Europe show that the most common foreign bodies aspirated are peanut and foods in children but dental prosthesis and food remnants in adults (4,8,9,10).
Foreign body aspiration in adults, is often seen in geriatric population because of some underlying diseases. Alcohol consumption, use of sedative and hypnotic drugs, senility, convulsion, general anesthesia, intoxication, traumatic intubation, trauma with unconsciousness, mental retardation, dental prosthetic interventions, primary neurological diseases are the factors that lead to foreign body aspiration. Also, some anomalities, and some postoperative problems like laryngectomy or tracheostomy may cause risk for the foreign body aspiration. Although only seven cases of aspiration in patients with a permanant post laryngectomy tracheal stoma have previously been published, we think that the presence of such a stoma should be added to the risk factors for foreign body aspiration in adults (11,12,13,14).
The localisation of foreign body is related with constution of bronchial tree and posture of patient during aspiration (15). The most common localisation is right main and distal bronchus (16). Because, right main bronchus is in more vertical position and has bigger diamater than left (17). 2/3 of foreign bodies are placed in main bronchus.
Miscellaneous aspirated objects have been reported worldwide, although the most frequents are nuts, vegetable matter, bones, metal and plastic objects or pills. There are also many unusual objects such as doll shoes, safety pins, turban scarf pins, plastic spoons, fishing weight, cockroaches, straight pin, or iron pill, tetracycline and sucralfate tablet, wood branch, plastic whistle and metalic fractured tracheostomy canula via tracheostomy (18).
The patients often applie to emergency services after aspiration. Sometimes there is no symptoms or sometimes there are several symptoms like cough, dispnea, and hemopthisis. In our patient, there were not any symptoms. Because our patient was elderly and his answers were suspicious, diagnosis was difficult. Occult foreign bodies can remain undetected for months to years and often are misdiagnosed (19).
In oscultation of patient with foreign body aspiration, wheezing can often be heard and ipsilateral chest sounds are limited (20,21). 21.8 % of patient with foreign body aspiration has delayed diagnosis (> 30 days) (22). For the diagnose, history, physical and radiological examination, and laboratory testing are frequently requaried and enough. Silvia et al. reported that sensitivity and specifity of radiological imaging methods for foreign body aspiration are 73% and 45% respectively (23). In the literature, rates of negative radiological finding show a huge variety of 8-80% (6,24,25). Most of foreign body can not be seen in chest radiogram but diagnosed by thorax CT like in our case. In some patients CT can not diagnose because of organized secretions.
Bronchoscopy should be done for the patients with respiratory problems without any clinical findings. Most of times, the first preference is flexible bronchoscopy (FB). FB is often enough to diagnose aspiration and to remove the foreign body. Some authors reported that FB is succesfull in about 100% in foreign body aspiration. However, it is a fact that these authors ignored the cases of thoracic surgery and pediatric surgery. FB has some advantages like facility of use, requires no anesthesia, enables to see distal bronchus. However, FB requires anesthesia but not general anesthesia. Against all these developments, rigit bronchoscopy (RB) is still the most effective method in diagnosis and treatment of foreign body aspiration. RB has some advantages like easy manipulation, facility of practical montage of telescopic systems, cost-effectiveness, good visualisation, and control of airway safety (20,26,27). RB is usually the first and correct preference in children. Also, the number of cases who are directly treated by a thoracic surgeon or whom FB was not succesful and proposed RB is fairly great (24,25,26,27,28). In patients with tracheostomy and in some emergency cases, RB can be done without general anesthesia like in our case. FB have many advantages and recommended to be the first application in most of the adult cases. On the other hand, RB should be selected as first line procedure in only selected cases.
According to the literature, negative bronchoscopies are unavoidable. In the studies rates of negative bronchoscopy are 8.5%, 15.8% and 10.6% respectively. RB has usually important rates of morbidity and mortality. But this morbidity rate of bronchoscopy is very low with experienced surgeons. These rates are about 2-22%. It is reported that the complication rates are increased following urgent bronchoscopy (20,21,29). These complications consist of pathologies like simple respiratory infections, subcutaneous emphysema, bronchial irritation, pneumonitis, bronchospasma, pneumothorax, cardiac arrest and even death (20,21,30,31). It is a reality that most of the authors ignore the cases treated by Thoracic Surgeons and Pediatric Surgeons. RB is the treatment of choise in childhood population. Besides the number of cases that are treated directly by thoracic surgeons or that are proposed RB following an unsuccesful intervention with FB is fairly great (24,25,26,27,28,30).
The complications of foreign body aspirations are seen frequently. These complications differerent with the type, localisation, aspiration time of the foreign body and with underlying medical conditions and other risk factors. The rate of bronchiectasis related with foreign body aspiration varies about 7.6-25% (31,32,33). In some cases with delayed diagnosis, foreign body may rarely cause hemopthisis (34,35). In these cases inflamation and granulation tissue appear surronding the foreign body (29,36). Complications like persistant fever, chronical cough, recurrent lung infections, bronchiectasis, bronchial stricture, athelectasis, lung abscess, pneumothorax and pneumomediastinum can be seen frequently (37,38).
Foreign body aspiration is still important for diagnose and treatment. In the patient with risc factors, foreign body aspiration should be persistently searched and questioned. It should not be forgotten that bronchoscopy is the gold standart for diagnose and treatment besides the clinical and radiological examinations.
CONFLICT of INTEREST
None declared.
REFERENCES
- Midulla F, Guidi R, Barbato A, et al. Foreign body aspiration in children. Pediatr Int 2005; 47: 663-8. [?zet]
- Steen KH, Zimmermann TH. Tracheobronchial aspirated of foreign bodies in children: a study of 94 cases. Laryngoscope 1990; 100: 525-30. [?zet]
- Ciftci A, Bingol-Kologlu M, Senocak ME, Tanyel FC, Buyukpamukcu N. Bronchoscopy for evaluation of foreign body aspiration in children. J Ped Surg 2003; 38: 1170-6. [?zet]
- Friedman EM. Tracheobronchial foreign bodies. Otolaryngol Clin North Am 2000; 33: 179-85. [?zet]
- Black RE, Choi KJ, Syme WC, et al. Bronchoscopic removal of aspirated foreign bodies in children. Am J Surg 1984; 148: 778-81. [?zet]
- Manto PC, Tuggle DW, Tunell WP. An appropriate negative bronchoscopy rate in suspected foreign body aspiration. Am J Surg 1989; 158: 622-4. [?zet]
- Marquette CH, Martinot A. Foreign body removal in adults and children. In: Bolliger CT (ed). Interventional bronchoscopy. Basel: S Karger AG, 2000: 96-107.
- Baharloo F, Veyckemans F, Francis C. Tracheobronchial foreign bodies presentation and management in children and adults. Chest 1999; 115: 1357-62. [?zet] [Tam Metin] [PDF]
- Nakhosteen JA. Tracheobronchial foreign bodies. Eur Respir J 1994; 7: 429-30. [PDF]
- Swanson KL, Prakash UBS, Midthun DE. Flexible bronchoscopic management of airway foreign bodies in children. Chest 2002; 121: 1695-700. [?zet] [Tam Metin] [PDF]
- Chen CH, Lai CL, Tsai TT, et al. Foreign body aspiration into the lower airway in Chinese adults. Chest 1997; 112: 129-33. [?zet] [PDF]
- Uzaslan E, Ursavas A, Ediger D, Karadag M. An unusual way of tracheal stoma cleaning could end up with foreign body aspiration in a laryngectomized patient. Tuberk Toraks 2005; 53: 61-4. [?zet] [PDF]
- Erdozain Rodriguez I, Sanchez Galan L, Zabaleta Lopez M, Sanchez del Hoyo A. Am tracheobronchial foreign body in the laryngectomized patient. An Otorrinolaringol Ibero 1998; 25: 185-92. [?zet]
- Krempl GA, Otto RA. Fracture at fenestration of synthetic tracheostomy tube resulting in a tracheobronchial airway foreign body. South Med J 1999; 92: 526-8. [?zet]
- Rafanan AL, Mehta AC. Adult airway foreign body removal. What's new? Clin Chest Med 2001; 22: 319-30. [?zet]
- Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: clinical utility of flexible bronchoscopy. Postgrad Med J 2002; 78: 399-403. [?zet] [PDF]
- Celik P, Yorganc?oglu A, Celik O. Laringotrakeobronsial yabanci cisim aspirasyonu. KBB Klinikleri 2000; 2: 50-6.
- Eliashar R, Sichel JY, Dano I, Saah D. Foreign body aspiration in a laryngectomized patient. Am J Emerg Med 1998; 16: 103-4.
- Y?lmaz A, Akkaya ED, Damadoglu E, Gungor S. Occult Bronchial body aspiration in adults: analysis of four cases. Respirology 2004; 9: 561-3. [?zet]
- Bodart E, de Biderling G, Tuerlinckx D, Gillet JB. Foreign body aspiration in childhood: management algorithm. Eur J Emerg Med 1999; 6: 21-5. [?zet]
- Metrangelo S, Monetti C, Meneghini L. Eight years experience with foreign body aspiration in children: what is really important for timely diagnosis? J Ped Surg 1999; 34: 1229-31. [?zet]
- Saquib MM, Rauf KA, Al-Bassam A. Late presentation of tracheobronchial foreign body aspiration in children. J Trop Pediatr 2005; 51: 145-8. [?zet]
- Silvia AB, Muntz HR, Clary R. Utility of coventional radiography in the diagnosis and management of pediatric airway foreign bodies. Ann Otol Rhinol Laryngol 1998; 107: 834-8. [?zet]
- Y?ld?r?m M, Dogusoy I, Okay T, et al. Trakeobronsial yabanci cisimler. TGKDCD 2003; 11: 228-31.
- Kolbak?r F, Kecelioglu T, Arikan A ve ark. Yabanci cisim aspirasyonu suphesiyle bronkoskopi yapilan 152 vakanin retrospektif analizi. TGKDCD 1994; 2: 2-6.
- Mathur NN, Pradhan T. Rigid pediatric bronchoscopy for bronchial foreign bodies with and without Hopkins telescope. Indian Pediatrics 2003; 46: 761-5. [?zet]
- Limper AH, Parakash UBS. Tracheobronchial foreign bodies in adults. Ann Intern Med 1990;112: 604-9. [?zet]
- Kisacik E, Gulhan E, Sirmali M, Sarica E ve ark. Trakeobronsiyal Yabanci Cisim Aspirasyonlari: 261 Olgunun Analizi. Solunum Dergisi 2004; 2: 86-91. [?zet] [PDF]
- Karakoc F, Cakir E, Ersu R, et al. Late diagnosis of foreign body aspiration in children with chronic respiratory symptoms. Int J Pediatr Otorhinolaryngol 2007; 71: 241-6. [?zet]
- Eren S, Balci A, Dikici B, Doblan M, Eren MN. Foreign body aspiration in children: experience of 1160 cases. Ann Trop Paed 2003; 23:31-7. [?zet]
- Findlay CA, Morrissey S, Paton JY. Subcutaneous emphysema secondary to foreign body aspiration. Ped Pulmon 2003; 36: 81-2. [?zet]
- Pasteur M, Helliwell S, Houghton S, Webb SC, Foweraker JE, Coulden RA, et al. An investigation into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med 2000; 162: 1277-84. [?zet] [Tam Metin] [PDF]
- Pogorzelski A, Zebrak J, Pawlik J, Cherian Z, Buchwald J. Broncho-pulmonary comlications due to aspiration of foreign bodies by children. Pediatr Pol 1995; 70: 325-31. [?zet]
- Cataneo AJ, Reibscheid SM, Ruiz Junior RL, Ferrari GF. Foreign body in the tracheobronchial tree. Clin Pediatr 1997; 36: 701-6. [?zet]
- Amir K, Ron S, Moshe G, Isaak S. Persistent cough and failure to thrive: a presentation of foreign body aspiration in a child with asthma. Pediatrics 2006; 117: 1057-60. [?zet] [Tam Metin] [PDF]
- Zuniga S, De Manana M, Monge M, et al. Vegetal foreign body in the airway: an unusual cause of hemoptysis in childhood: clinical case. Rev Med Chil 2000; 128: 323-9. [?zet]
- Tokar B, Ozkan R, Ilhan H. Tracheobronchial foreign bodies in children: importance of accurate history and plain chest radiography in delayed presentation. Clin Radiol 2004; 59: 609-15. [?zet]
- Sahni JK, Mathur NN, Kansal Y, Rana I. Bronchial foreign body presenting as an accidental radiological finding. Int J Pediatr Otorhinolaryngol 2002; 64: 229-32. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Ekrem ?ENT?RK,
Adnan Menderes ?niversitesi T?p Fak?ltesi,
G???s Cerrahisi Anabilim Dal?,
09100 AYDIN - TURKEY
e-mail: ekremsenturk@hotmail.com