G???s duvar? kondrosarkomuna sekonder spontan masif hemotoraks: Bir olgu sunumu
Mohammad
Ghasemi RAD1, Rahim MAHMODLOU1, Afshin MOHAMMADI1,
Nikol MLADKOVA2,
Farahnaz NOOROZINIA2
1 Urmiye ?niversitesi T?p Fak?ltesi, Urmiye, Bat? Azerbaycan, ?ran,
1 H?cre ve Molek?ler Bilimler Enstit?s?, Londra, Birle?ik Krall?k.
?ZET
G???s duvar? kondrosarkomuna sekonder spontan masif hemotoraks: Bir olgu sunumu
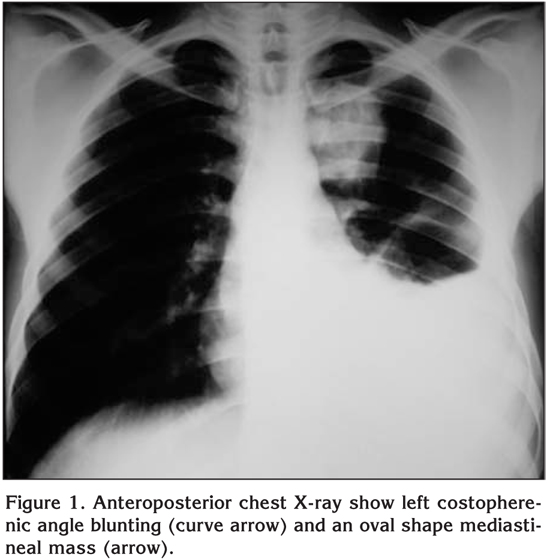
Otuz ya??nda, daha ?nce hastal?k ?yk?s? ve yak?n zamanda travma ?yk?s? olmayan, sol hemitoraksta keskin a?r? ile acil serviste g?r?len bir hastay? sunuyoruz. G???s radyografisinde kostofrenik sin?ste k?ntle?me ve sol mediastende oval bir kitle saptand?. Bilgisayarl? tomografide, manyetik rezonans g?r?nt?leme ile do?rulanan, kalsifiye ekstraplevral kitle ve plevral ef?zyon izlendi. Torakotomi yap?larak biyopsi al?nd? ve t?m?r ??kar?ld?. Patolojik incelemede spontan masif hemotoraks?n nadir bir nedeni olan kondrosarkom saptand?. Bu hastada, interkostal damarlar?n t?m?rle invazyonu hemotoraks?n muhtemel nedeniydi.
Anahtar Kelimeler: Spontan masif hemotoraks, g???s duvar?, kondrosarkom.
SUMMARY
Spontaneous massive hemothorax secondary to chest wall chondrosarcoma: a case report
Mohammad
Ghasemi RAD1, Rahim MAHMODLOU1, Afshin MOHAMMADI1,
Nikol MLADKOVA2,
Farahnaz NOOROZINIA2
1 Faculty of Medicine, Urmia University, Urmia, West Azerbaijan, Iran,
2 Institute of Cell and Molecular Science, London, United Kingdom.
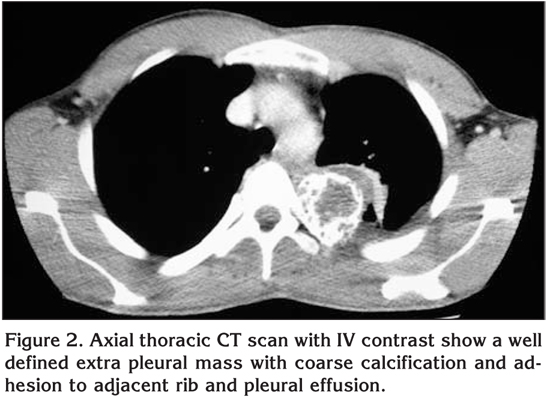
We present the case of a 30-year-old man with no past history of disease or recent trauma, who was seen in the emergency room after developing sharp pain in the left hemithorax. Chest roentgenogram showed costopherenic angle blunting and an oval mass in the left mediastinum. A computed tomographic scan showed extrapleural mass with coarse calcifications and pleural effusion, confirmed by magnetic resonance imaging. The tumor was biopsied and removed during thoracotomy. The pathology reported revealed chondrosarcoma, which is a rare cause for a spontaneous massive hemothorax. Invasion of the intercostals vessels by the tumor was the probable cause of hemothorax in this patient.
Key Words: Spontaneous massive hemothorax, chest wall, chondrosarcoma.
Hemothorax is defined as an extraction of pleural fluid with a hematocrit greater than 50% of the blood hematocrit and it may relatively commonly occur in the context of a chest trauma or medical procedures such as central venous catheterization (1). Spontaneous hemothorax, on the other hand, is a rare clinical presentation that can be caused by heterogeneous factors including malignancies, vascular abnormalities, hematological abnormalities (hemophilia), pulmonary affections (tuberculosis, infarctions), spontaneous and idiopathic causes (2). We describe a case of spontaneous hemothorax caused by chest wall chondrosarcoma.
CASE REPORT
A 30-year-old Azari male without previous history of disease or recent trauma was admitted to our emergency department after he has developed pleural chest pain in the left hemithorax. The pain was described as sharp in character and radiating to the back and the left shoulder. The pain was constant, accompanied by severe shortness of breath and allegedly started suddenly when the patient was working in the bakery.
Three days prior to the onset of the pain the patient recalled having dry cough, low-grade fever and shortness of breath. The patient had no past medical history including psychiatric and was not on any medication, but took regular acetaminophen for a headache. The patient was a non-smoker and denied alcohol or opium consumption.
Originally, the patient went to emergency in nearby hospital, and a chest roentgenogram revealed the presence of costopherenic angle blunting and an oval mass in the left mediastinum (Figure 1). On chest drain insertion, a total of two liters of blood was drained. Subsequently, the patient received four units of packed red blood cell (RBC) transfusion and two units of fresh frozen plasma (FFP). After he was stabilized, he was transported to our tertiary center for further work-up.
Upon arrival to the emergency department, physical examination revealed a young asthenic male not in distress. Blood pressure (BP) was 125 on 70, pulse rate was 86 BPM and respiratory rate of 18 breaths/min. The axillar temperature was 37.1 degree Celsius. The patient was normocephalic without bitemporal atrophy; other examinations were unremarkable except for dullness to percussion and the absence of breath sounds at the left lung base. The chest drain was inserted in the left hemithorax, in the fifth intercostal space-anterior axillary line. The chest drain collected 500cc of bloody non-clotting fluid which was shown to have 33% of hematocrit and was negative for bacterial culture. Computed tomographic (CT) scan of the chest showed a well-defined, extra-pleural mass with coarse calcification and adhesions to adjacent rib, and a pleural effusion (Figure 2). Magnetic resonance imaging (MRI) of the chest showed a well-defined, intermediate signal mass of oval shape in the posterior part of the chest wall accompanied by a pleural effusion (Figure 3). After the patient was stabilized (5 days later), he underwent left posterolateral thoracotomy under general anesthesia, which yielded 500-600 cc of old, clotted blood in the chest cavity. Based on the imaging techniques and presentation within the chest cavity, the tumor was believed to originate from the posterior part of the fourth rib and to extend towards vertebrae.

The upper lung lobe had adhesions to the tumor, but the lobe was intact and with no signs of gross invasion from the tumor. When the upper lobe was detached from the tumor, mild blood oozing from the tumor was noted.
The fourth rib and the posterior part of the third and fifth rib were completely removed, together with a segment of the fourth vertebrate body which was removed by a neurosurgeon, but the dura was not opened. Since the malignant lesion was located mostly below the left scapula, it was not necessary to reconstruct the rib cage. No other mass was observed in other areas of the lungs, mediastinum or the diaphragm.
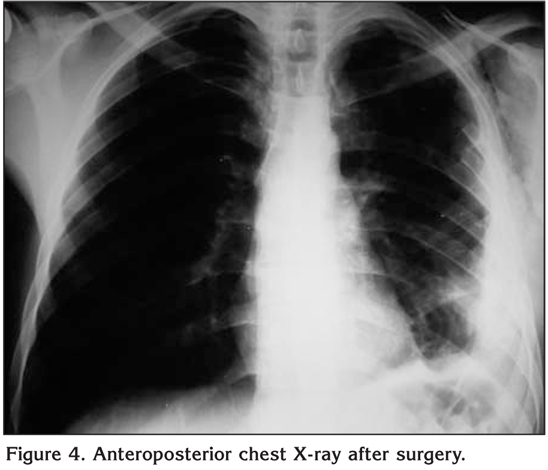
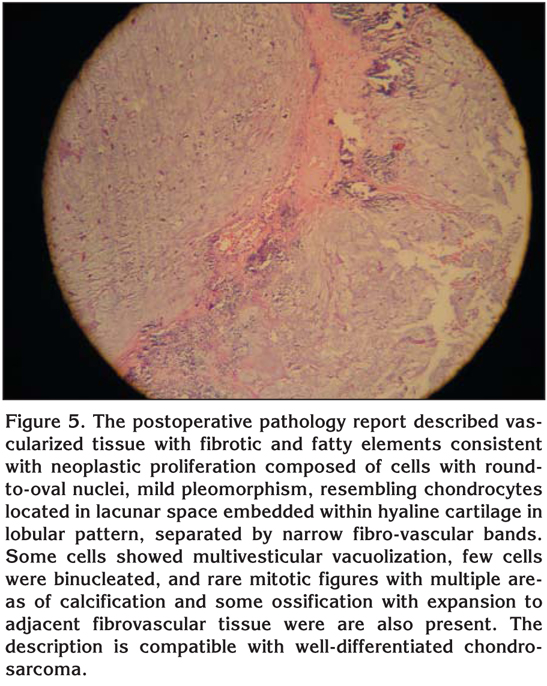
After the operation, the patient was transferred to the intensive care unit where he remained for 24 hours before being transferred to the ward. He was discharged five days after the operation. The post-operative chest roentgenogram showed no mass in the chest (Figure 4). The post-operative pathology report confirmed a Well-differentiated chondrosarcoma (Figure 5).
DISCUSSION
Chondrosarcoma is a malignant mesenchymal tumor that arises from developed cartilage and constitutes about 9% of primary bone cancers (3). It is the most common primary chest wall tumor (4). The incidence peaks between the ages of 40 and 60 years for primary chondrosarcoma and between 25 and 45 years of age for secondary chondrosarcoma (3). The most common symptoms of chest wall chondrosarcoma include pain in the chest wall or a palpable mass (4). These tumors mostly arise in the sternum, anterior costochondral junction, vertebral body and costal angles (4). The computed tomography (CT) scan shows low density mass with coarse calcification as in this case (4). Histologically, chondrosarcomas are differentiated from benign cartilage lesions by plump nuclei, hypercellularity, a permeative pattern, more than occasional binucleate cells and the entrapment of bony trabeculae (3).
A spontaneous hemothorax is a rare clinical condition in the absence of trauma or iatrogenic causes (2). Hemothorax is defined as pleural fluid extraction with more than 50% of the concomitant hematocrit, and massive hemothorax is defined as the extraction of more than 1500 cc of blood upon chest drain insertion (1). It is a well-identified consequence of a blunt or penetrating chest trauma, intrathoracic vessel cannulation, chest drain insertion, thoracentesis, pleural biopsy, aortic aneurysm rupture, anticoagulation therapy, necrotizing lung infection, pulmonary infarcts, spontaneous pneumothorax, arteriovenous, malformation, endometriosis, exostoses, tuberculosis, uremia, hemophilia and diverse pleural malignancies (1,5). The most common malignancies associated with hemothorax comprise of schwanommas of von Recklinghausen disease, and soft tissue tumors (sarcoma, angiosarcoma, and hepatocellular carcinoma) (1). In the case of our patient, a possible cause for the sudden development of the hemothorax could have been the involvement of intercostal vascular structures by the tumor, or alternatively, given the vascularity of the tumor, its adhesions with the upper lobe of the left lung. This explanation is less likely since the bleeding from the tumor observed during thoracotomy was of mild character.
The successful management of hemothorax depends on many factors, namely the severity of the blood loss and subsequent hemodynamic stability of the patient. In our case, the patient did not require cardio-pulmonary resuscitation, but required repeated transfusion for stabilization, followed by thoracotomy a few days later during which the cause of hemothorax was removed.
The main treatment of high-grade chondrosarcoma is a radical resection or amputation. Radiotherapy and chemotherapy have proven ineffective unless the tumor is surgically inaccessible. In such cases, radiotherapy can be useful (3,6). The 10-year survival of patients with high-grade chondrosarcoma is reported to reach between 20% to 40% (3). Local recurrence and distant metastasis is high even in low-grade primary tumors and recurrence can occur years or decades after the primary tumor has been removed (3,6). This corroborates the recommendation of tumor resection with sufficient tumor-free margin (3-4 cm) (6).
Previously reported malignancies causing spontaneous hemothroax include lymphangiosarcoma and vascular mediastinal schwannoma, lymphangioma, mediastinal teratoma metastatic choriocarcinoma, mediastinal or pulmonary malignancy, metastatic renal carcinoma, Abrikossoff tumor, pulmonary angiosarcoma, osterochondroma, Kaposiform endodermal sinus tumour, hemangioendothelioma, epithelioid hemangioendothelioma, hemangioma, hemangiopericytoma fibrous tumor of the pleura, hepatocarcinoma, periosteal chondroma, chondroblastoma of the rib, synovial sarcoma, osteosarcoma, Ewig sarcoma, neurofibrosarcoma, thymoma, mediastinal meningioma, thoracic neuroblastoma, pleural mesothelioma, chronic myeloid leukaemia (2,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32).
Hemothorax is a severe, life-threatening condition that requires immediate medical attention. We described a case of massive spontaneous hemothorax in otherwise healthy young male secondary to chondrosarcoma of the chest wall. So far, there was only one such case described (33).
Although hemothorax is an extremely rare presentation of this tumor, chondrosarcoma represents the most common malignant tumor of the chest wall (34) and due to its ability to recur many years after the first presentation, its local recurrence should be clinically excluded as a possible cause of blood accumulation in the chest cavity in patients with the history of chest wall chondrosarcoma. The treatment of the tumor consists mainly of surgical excision with wide (3-4 cm) surgical margin and the prognosis is relatively favourable. Our case is the second to describe hemothorax in chest wall chondrosarcoma patient and underscores the importance of systemic approach to each case of this life-threatening condition.
CONFLICT of INTEREST
None declared.
REFERENCES
- Ali HA, Lippmann M, Mundathaje U, Khaleeq G. Spontaneous hemothorax: a comprehensive review. Chest 2008; 134: 1056-65. [?zet] [PDF]
- Chetcuti K, Barnard J, Loggos S, Hassan M, Srivastava V, Mourad F.? Massive hemothorax secondary to metastatic renal carcinoma. Ann Thorac Surg 89: 2014-6. [?zet]
- S. Terry Canale JHb. Campbell's Operative Orthopaedics. 11th ed. Philadelphia: Mosby Elsevier, 2008.
- Shimoyama T, Suzuki R, Yoshiya K, Yamato Y, Koike T. Chondrosarcoma of the rib. Jpn J Thorac Cardiovasc Surg 2003; 51: 167-71. [?zet]
- Dimitri WR. Massive idiopathic spontaneous haemothorax. Case report and literature review. Eur J Cardiothorac Surg 1987; 1: 55-8. [?zet] [PDF]
- Yamamoto NIS, Motohiro K, Shiota Y, Sato N, Nakayama H. A case of chnodrosarcoma of the low grade malignancy originated in the rib. Kyobu Geka 1995; 48: 1141-3. [?zet]
- Larriew AJ HS, Allen P. Spontaneous massive hemothorax in von Recklinghausen's disease Thorax 1982; 37: 151-2. [PDF]
- Menth M, Balmer MC, Ris HB. Blunt thoracic trauma with hemorrhage into a mediastinal lymphangioma-case report. Swiss Surg 1998; 4: 58-60. [?zet]
- Yang WM, Chen ML, Lin TS. Traumatic hemothorax resulting from rupture of mediastinal teratoma: a case report. Int Surg 2005; 90: 241-4. [?zet]
- Shiota S, Nakaya Y, Sakamoto K, Iwase A, Aoki S, Matsuoka R, et al. Spontaneous hemothorax secondary to immature teratoma of the mediastinum. Intern Med 1999; 38: 726-8. [?zet]
- De Franc JH BJ, Ricci JA, Patterson MD. Massive haemothorax: two unusual cases. Chest 1974; 66: 82-4. [PDF]
- Honigmann P, Walz A, Bussmann C, Lerf B. Spontaneous bleeding of an Abrikossoff's tumor-a case report. J Cardiothorac Surg 2009; 4: 57. [?zet] [Tam Metin] [PDF]
- Campione A, Forte G, Luzzi L, Comino A, Gorla A, Terzi A. Pulmonary angiosarcoma presenting as spontaneous recurrent hemothorax. Asian Cardiovasc Thorac Ann 2009; 17: 84-5. [?zet] [Tam Metin] [PDF]
- Asmat A, Tam J. Spontaneous haemothorax from an osteochondroma. Eur J Cardiothorac Surg 2009; 36: 394.
- Schiller PH, Finlay BL, Volman SF. Quantitative studies of single-cell properties in monkey striate cortex. III. Spatial frequency. J Neurophysiol 1976; 39: 1334-51. [?zet]
- San Miguel FL, Spurbeck W, Budding C, Horton J. Kaposiform hemangioendothelioma: a rare cause of spontaneous hemothorax in infancy. Review of the literature. J Pediatr Surg 2008; 43: e37-41. [?zet]
- Gan S, Bannon PG. Spontaneous malignant haemothorax: pulmonary haemangioendothelioma. ANZ J Surg 2003; 73: 966-7.
- Bhaskar J, Sharma AK. Spontaneous hemopneumothorax as a result of venous hemangioma: a unique case? Tex Heart Inst J 2006; 33: 91-2. [?zet] [Tam Metin] [PDF]
- Mori M, Nakanishi N, Furuya K. Hemangiopericytoma of the mediastinum causing spontaneous hemothorax. Ann Thorac Surg 1994; 58: 1525-7. [?zet]
- Kushner DH. The frequency and fate of pregnancy after age 45. Med Ann Dist Columbia 1974; 43: 491-2.
- Lin HH, Liew CT, Liaw YF. Hepatocellular carcinoma presenting as acute spontaneous haemothorax. J Gastroenterol Hepatol 1990; 5: 362-4. [?zet]
- Matsushima K, Matsuura K, Kayo M, Gushimiyagi M. Periosteal chondroma of the rib possibly associated with hemothorax: a case report. J Pediatr Surg 2006; 41: E31-3. [?zet]
- Varsano S, Edelstein E, Gendel B, Smorzik J. Bilateral and unilateral spontaneous massive hemothorax as a presenting manifestation of rare tumors. Respiration 2003; 70: 214-8. [?zet]
- Sakurai H, Hosokawa H, Hada M, Miyashita Y, Oyama T, Ashizawa I. Spontaneous hemothorax caused by intrathoracic synovial sarcoma. Jpn J Thorac Cardiovasc Surg 2006; 54: 217-20. [?zet]
- Tsuda K, Nishi M, Yamada K, Yamamoto K. Spontaneous hemothorax in a patient with lung metastases of osteosarcoma. Masui 2005; 54: 1027-9. [?zet]
- Eroglu A, Kurkcuoglu IC, Karaoglanoglu N, Alper F, Gundogdu C. Extraskeletal Ewing sarcoma of the diaphragm presenting with hemothorax. Ann Thorac Surg 2004; 78: 715-7. [?zet] [Tam Metin] [PDF]
- Lim R, de Souza AD, Beggs D. Neurofibrosarcoma presenting as spontaneous haemothorax. Br J Clin Pract 1990; 44: 289-91.
- Shimokawa S, Watanabe S, Sakasegawa K, Tani A. Ruptured thymoma causing mediastinal hemorrhage resected via partial sternotomy. Ann Thorac Surg 2001; 71: 370-2. [?zet] [PDF]
- Palimento D, Picchio M. Meningioma of the mediastinum causing spontaneous hemothorax. Ann Thorac Surg 2006; 81: 1903-4. [?zet] [Tam Metin] [PDF]
- Minola E, Gambacorta M. Hemothorax in congenital neuroblastoma. Tumori 1987; 73: 81-3. [?zet]
- Cifrian Martinez JM, Aguero Balbin R, Garcia Perez MM. Spontaneous massive hemothorax as initial manifestation of malignant pleural mesothelioma. Arch Bronconeumol 1994; 30: 474.
- Kuo YC, Wang HC, Chu KA, Lu JY. Chronic myeloid leukemia initially presenting with spontaneous mediastinal hematoma and hemothorax. Zhonghua Yi Xue Za Zhi (Taipei) 2000; 63: 170-4. [?zet]
- Karlawish JH, Smith GW, Gabrielson EW, Liu MC. Spontaneous hemothorax caused by a chest wall chondrosarcoma. Ann Thorac Surg 1995; 59: 231-3. [?zet] [PDF]
- Grodzki T, Wojcik J, Pierog J, Kubisa B. Long-term survival after resection of giant chondrosarcoma of the chest wall weighing 9.6 kg. Eur J Cardiothorac Surg 2007; 32: 394-6. [?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Mohammad Ghasemi RAD,
No 300, 1st Ally jonobi St, Farhangian
57167 URMIAN - IRAN
e-mail: medman11@gmail.com