?n g???s duvar? t?m?r?n? taklit eden primer sternal t?berk?loz: Bir olgu sunumu
Nikolaos BARBETAKIS, Christos ASTERIOU, Athanassios KLEONTAS, Christos KARVELAS
Theagenio Hastanesi, G???s Cerrahisi B?l?m?, Thessaloniki, Yunanistan.
?ZET
?n g???s duvar? t?m?r?n? taklit eden primer sternal t?berk?loz: Bir olgu sunumu
Burada, g???s duvar? t?m?r?n? taklit eden ve primer sternal t?berk?loz tan?s? alan sternal kitleli olgu sunulmaktad?r. ?nce i?ne aspirasyonu tan?sal de?ildi ve cerrahi i?lemle, tutulan kemik etraf?ndaki yumu?ak dokuda b?y?k bir apsenin eksizyonu ve drenaj? yap?ld?. Patolojik incelemede t?berk?loz osteomiyelit ile uyumlu multipl gran?lomat?z ve nekrotik lezyon saptand?. D?rtl? antit?berk?loz tedavi ile alt? ay sonra belirgin iyile?me sa?land?.
Anahtar Kelimeler: T?berk?loz, sternum, t?m?r.
SUMMARY
Primary sternal tuberculosis mimicking anterior chest wall tumor: case report
Nikolaos BARBETAKIS, Christos ASTERIOU, Athanassios KLEONTAS, Christos KARVELAS
Department of Chest Surgery, Theagenio Hospital, Thessaloniki, Greece.
A case of a sternal mass mimicking a chest wall tumor and finally diagnosed as primary sternal tuberculosis is presented. Fine needle biopsy was inconclusive and surgery included excision and drainage of a large abscess in the soft tissues around the involved bone. Pathology revealed multiple granulomatous and necrotic lesions consistent with tuberculous osteomyelitis. On a 4-drug antituberculous regimen the patient is an excellent condition 6 months later.
Key Words: Tuberculosis, sternum, tumor.
Primary tuberculous osteomyelitis of the sternum is a form of extrapulmonary tuberculosis (TB) that is extremely rare and belongs to the differential diagnosis of chest wall masses. It accounts for 1.5% of osteoarticular TB (1). Management involves standard antituberculous therapy with antibiotics, as well as consideration of surgical intervention depending on diagnostic dilemmas or the extent of osteomyelitis.
Approximately 60% to 80% of skeletal TB cases involve the spine or weight-bearing joints (2). Thus diagnosis of sternal TB is often not considered, especially in developed countries. The diagnosis is usually made until the disease is well advanced, with 25 cases reported in peer-reviewed journals in the literature review (3).
A case of a sternal mass mimicking a chest wall tumor and finally diagnosed as primary sternal tuberculosis is presented.
CASE REPORT
A 48-year-old male presented with a 6-months history of a gradually-enlarged anterior chest wall mass. Low grade fever with evening rise, sternal discomfort and anorexia were present for last 3 months. There was no significant past history.
Clinical examination demonstrated a lower presternal swelling next to the xiphoid process. On palpation and percussion, there was tenderness over sternum. However there was no tenderness over spine and paraspinal muscles in the thoracic region. The range of motion of spine was within normal limits. There was no lymphadenopathy. The abdomen was soft and non tender with no organomegaly. Other systems were normal.
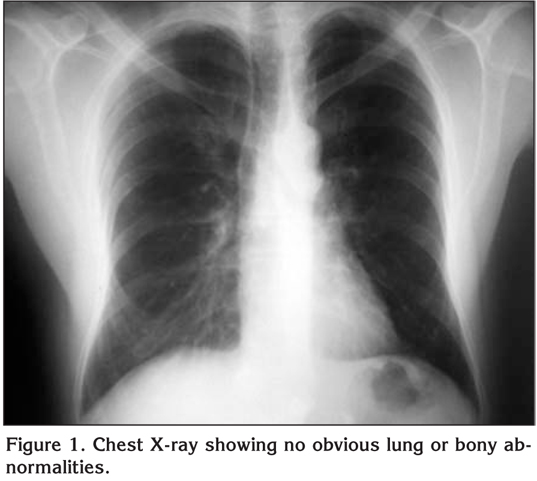
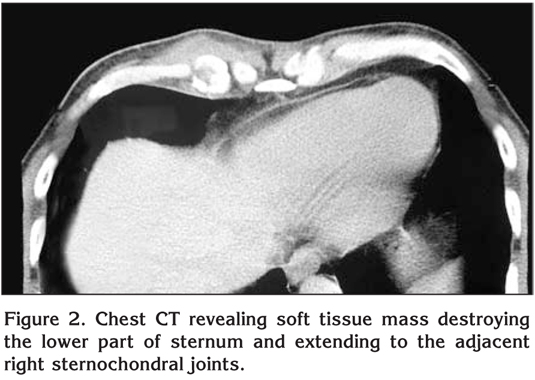
Laboratory findings revealed elevated erythrocyte sedimentation rate (ESR) of 60 mm/hour and a positive C-reactive protein (CRP) test. A plain chest radiograph posterior-anterior and lateral views, showed no lung infiltration, pleural effusion, enlargement of hilar lymph nodes and any bony involvement (Figure 1). A chest computed tomography (CT) was consistent with a soft tissue lesion destroying the lower part of sternum and extending anteriorly to the adjacent right sternochondral joints (Figure 2).
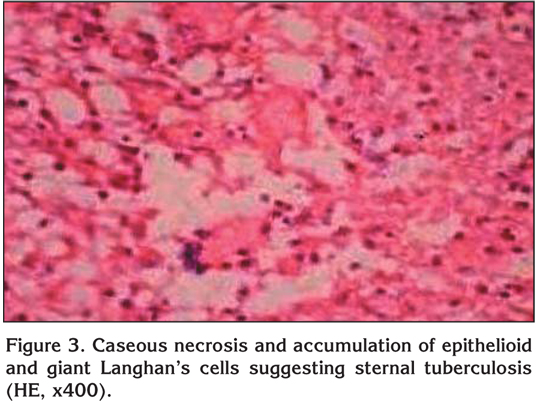
The patient underwent complete staging with brain and abdomen CT scans and a bone scan which were negative for possible metastatic disease. Fine needle aspiration (FNA) cytology was inconclusive and did not rule out malignancy. Surgical management required parasternal mass excision with en bloc excision of two right costochondral joints. Infected granulation tissue composing of a white cheesy discharge was extending to the inner table of the sternum. The granulation tissue was curetted until healthy bleeding bony surface was observed. The pectoralis major muscle was mobilized to cover the defect and the wound was closed in layers over two suction drains. The patient had an uneventful recovery. Pathology was consistent with caseous necrosis and accumulation of epithelioid and giant Langhan's cells suggesting sternal tuberculosis (Figure 3). Polymerase chain reaction (PCR) from the white cheesy discharge came positive for Mycobacterium tuberculosis. The patient was started a 4-antituberculous regimen (rifampin 600 mg/day, pyrazinamide 2000 mg/day, ethambutol 1600 mg/day and isoniazide 300 mg/day). Six months later the patient had significant improvement and a weight gain of 6 kg. He denied any symptoms, draining sinuses, sternal erythema or pain.
DISCUSSION
Sternal TB is an extremely rare condition. It can be presented as a painful mass at the sternal level with general symptoms of fever, weight loss, and anorexia, thus diagnosing is necessary for a high index of suspicion and to rule out a malignancy (4). However, when there is a high index of clinical suspicion, histologic examination of affected tissues and mycobacterium cultures are necessary (5).
Up to one third of such patients had a detectable tuberculous lesion in other parts of the skeleton or in the lungs (6). Our patient had no evidence of skeletal TB, and his chest radiography showed no evidence of prior TB. Radiographic findings of sternal TB occur much later than those taken with clinical measurements.
The CT scan is more sensitive for anatomical localization and in detecting osseous destruction and soft tissue abnormalities. Khalil et al. reviewed the utility of CT scan findings for the diagnosis of chest wall TB and described characteristic ring enhancing hypodense soft tissue lesion (7). Atasoy et al. suggested the role of magnatic resonance imaging (MRI) for detecting early marrow and soft tissue involvement due to high contrast resolution of MRI (8). Tuberculous osteomyelitis is characterized by low signal replacement of the normal marrow fat signal on T1-weighted images, with high signal intensities on T2-weighted images and enhancement on T1-weighted images (4).
Definitive diagnosis rests largely with the histological and microbiological examination of sternal tissue. Needle aspiration, as compared to surgical exploration, is less invasive and may represent the diagnostic procedure of first choice. However, it demonstrates positive cultures less frequently than excisional biopsy (9).
Possible complications of sternal tuberculous osteomyelitis include secondary infection, fistula formation, spontaneous fractures of the sternum, compression or erosion of the large blood vessels, compression of the trachea and migration of tuberculous abscess into the mediastinum, pleural cavity or subcutaneous tissues (10).
Treatment is based on long duration antituberculous multidrug therapy. Although there is no consensus guideline to the precise regimen and duration for sternal TB, extrapulmonary TB is generally treated with a 6 to 9 month regimen (six months of rifampin, isoniazide, ethambutol and pyrazinamide followed by 3 months of isoniazide and rifampin) unless the organisms are known or highly suspected to be resistant to these first line drugs. Lesions can be seen radiologically to start healing by 6 months. Response depends on the stage of disease when treatment was started.
Surgical excision is justified in refractory cases, whenever there is a doubt in diagnosis, in the presence of a large abscess in the soft tissues around the involved bone, or to remove large sequestrum. Surgical treatment for tuberculous osteomyelitis of the sternum involves extensive debridement and curettage of all involved tissue. The defect can be closed primarily if possible or more commonly by mobilization of the overlying pectoralis major as a flap. Another method described in the literature includes vacuum-assisted closure with a drain (11).
The possibility of sternal TB should be kept in mind in any patient with a mass, non healing ulcer or abscess in the sternal region. The most appropriate management scheme would be to perform first a needle aspiration or biopsy; if tuberculous infection is then confirmed or strongly suspected, a combination regimen of antituberculous chemotherapy should be considered as initial treatment. If definitive diagnosis is lacking or if the lesion fails to improve after 1 to 3 months of medication or worsens, surgical intervention is indicated. Extensive resection is the basis of removing osteochrondritic lesions and additional adjuvant antituberculotic therapy is essential to avoid recurrence.
CONFLICT of INTEREST
None declared.
REFERENCES
- Tuli SM. Tuberculosis of rare sites, girdle and flat bones. In:? Tuli SM (ed). Tuberculosis of the Skeletal System. Bursal Sheaths. 2nd ed. Delhi: Jaypee Brothers Medical Publishers, 2000: 159-160.
- Zhao X, Chen S, Deanda A. A rare presentation of tuberculosis. Am Surg 2006; 72: 96-7. [?zet]
- Vasa M, Ohikhuare C, Brickner L. Primary sternal tuberculous osteomyelitis: a case report and discussion. Can J Infect Dis Med Microbiol 2009; 20: 181-4. [?zet] [Tam Metin] [PDF]
- Shah J, Patkar D, Parikh B, Parmar H, Varma R, Patankar T, Prasad S. Tuberculosis of the sternum and clavicle: imaging findings in 15 patients. Skeletal Radiol 2000; 29: 447-53. [?zet]
- Stewart KJ, Ahmed OA, Laing RB, Holmes JD. Mycobacterium tuberculosis presenting as sternal osteomyelitis. J R Coll Surg Edinb 2000; 45: 135-7. [?zet]
- Gopal K, Raj A, Rajesh MR, Prabhu SK, Geothe J. Sternal tuberculosis after sternotomy for coronary artery bypass surgery: a case report and review of the literature. J Thorac Cardiovasc Surg 2007; 133: 1365-6. [Tam Metin] [PDF]
- Khalil A, Le Breton C, Tassart M, Korzec J, Bigot J, Carette M. Utility of CT scan for the diagnosis of chest wall tuberculosis. Eur Radiol 1999; 9: 1638-42. [?zet]
- Atasoy C, Oztekin PS, Ozdemir N, Sak SD, Erden I, Akyar S. CT and MRI in tuberculous sternal osteomyelitis: a case report. Clin Imaging 2002; 26: 112- 5. [?zet]
- McLellan DGJ, Philips KB, Corbett CE, Bronze MS. Sternal osteomyelitis caused by Mycobacterium tuberculosis: case report and review of literature. Am J Med Sci 2000; 319: 250-4. [?zet]
- Sharma S, Juneja M, Garg A. Primary tubercular osteomyelitis of the sternum. Indian J Pediatr 2005; 72: 709-10. [?zet]
- Ford SJ, Rathinam S, King JE, Vaughan R. Tuberculous osteomyelitis of the sternum: successful management with debridement and vacuum assisted closure. Eur J Cardiothorac Surg 2005; 28: 645-7. [?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Nikolaos BARBETAKIS,
A. Simeonidi 2 54007
THESSALONIKI - GREECE
e-mail: nibarbet@yahoo.gr