Migration of a fractured totally implantable venous access catheter into the right ventricle
Nikolaos BARBETAKIS, Christos ASTERIOU, Athanassios KLEONTAS, Christos KARVELAS
1 Theagenio Kanser Hastanesi, G???s Cerrahisi B?l?m?, Thessaloniki, Yunanistan.
Totally implantable venous catheters are increasingly being utilized for venous access in patients requiring long-term chemotherapy.
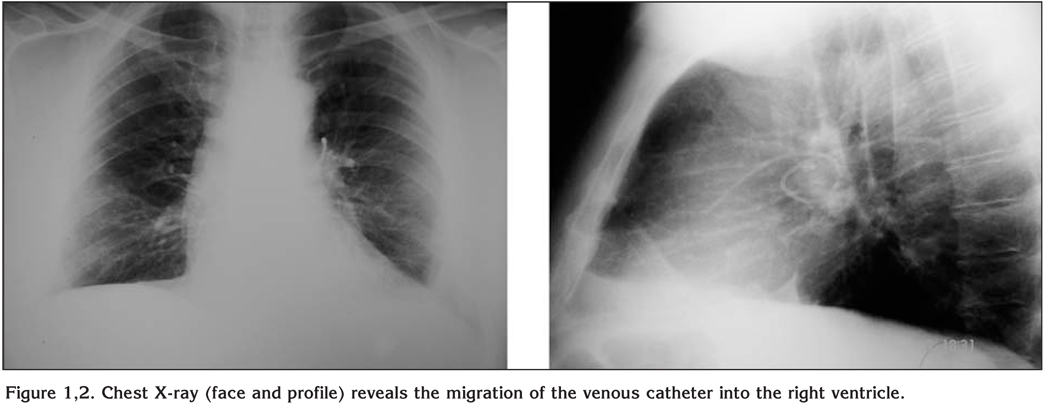
A 42-year-old woman with a history of breast cancer and hepatic metastatic disease underwent insertion of an implantable venous access catheter into the right subclavian vein (Seldinger technique). After eight months of treatment it was decided to remove the catheter due to reported possible thrombosis and obstruction. The patient was totally asymptomatic. A preoperative chest X-ray was consistent with migration of the catheter into the right ventricle (Figure 1,2). Percutaneous retrieval through right internal jugular vein and right femoral vein was unsuccessful as the catheter end was embedded in the myocardium. The catheter was removed via a median sternotomy through the main pulmonary artery without any further complications.
The two most important risk factors for catheter fracture and migration include pinch-off syndrome (compression of the catheter between first rib and clavicle), inadequate heparinization and excessive pressure later, for return in normal function (1). We would like to alert clinicians for this rare and significant complication. Further guidelines include the following (2):
a. Totally implantable venous access catheters require heparinised saline flushing once a month, even not in use,
b. Periodic chest X-rays are mandatory in order to detect pinch-off syndrome,
c. Any implanted catheter should be removed after completion of treatment, or the system's integrity has to be monitored on a regular basis.
CONFLICT of INTEREST
None declared.
REFERENCES
- Filippou D, Tsikkinis C, Filippou G, et al. Rupture of totally implantable central venous access devices in patients with cancer: report of four cases. World J Surg Oncol 2004; 2: 36. [?zet] [Tam Metin] [PDF]
- Sumit K, Rajiv P, Tarun G, Ajay Y. Catheter fracture and cardiac migration of a totally implantable venous device. Indian J Cancer 2005; 42: 155-7. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Nikolaos BARBETAKIS,
A. Simeonidi 2 54007
THESSALONIKI - GREECE
e-mail: nibarbet@yahoo.gr