Forgotten but an important risk factor for pulmonary embolism: ophthalmic surgery
Asiye KANBAY1, Hatice Canan HASANO?LU2, Ay?eg?l KARALEZL?2, G?khan AYKUN2, Fatma Y?LEK3
1 Erciyes ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Kayseri,
2 Ankara Atat?rk E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? Klini?i, Ankara,
3 Ankara Atat?rk E?itim ve Ara?t?rma Hastanesi, G?z Klini?i, Ankara.
To the Editor,
There is increasing evidence that venous thromboembolism (VTE) which includes deep vein thrombosis and pulmonary embolism (PE) has a significant mortality and morbidity due the challenge in application of prophylaxis and immediate treatment (1). Consequently the recommendations in clinical guidelines for applying prophylaxis to prevent PE are being updated continuously (2). However awareness of this problem there is no perioperative prophylaxis recommendation for ophthalmic surgery in current guidelines. Herein, we present 6 cases of whom did not receive prophylaxis had PE after ophthalmic surgery to notice to an important risk factor for PE.
The clinical characteristics of the patients are presented in Table 1. There were no hemorrhagic events noted perioperatively in none of the patients. None of the patients had history of connective tissue disease and had predisposing factor for VTE except surgery. One had vitrectomy and other 5 patients had cataract surgery.
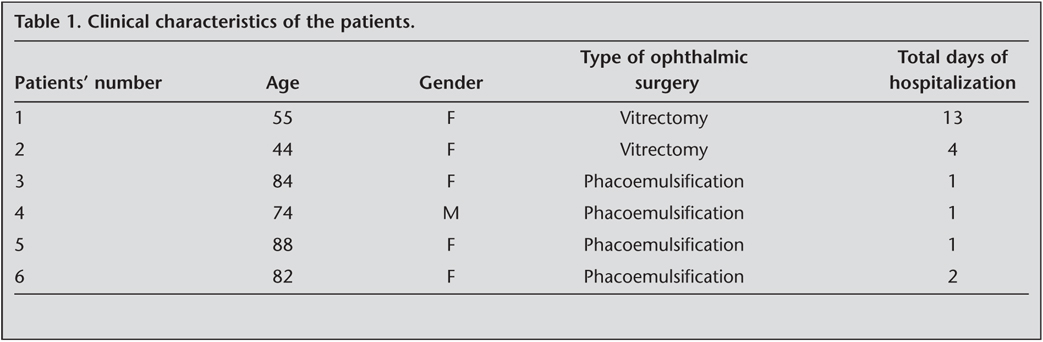
The symptoms of the PE developed 2-7 days after the surgery in all of the patients. The first patient was hospitalized for a long period for controlling post operatively raised intraocular pressure. Four cases received thrombolytic therapy with the diagnosis of massive PE. One of the patients with massive PE who had vitrectomy operation was died even aggressive therapy including thrombolytic and vasopressor agents. Other 2 cases who had submassive PE were treated with heparin and intravasculer fluid support.
Generally, patients have mobilization problem after ophthalmic surgery due to serious vision problem. These cases highlighted that microsurgeries including ophthalmic surgery might be a risk factor for VTE even in patients without any predisposing factor (3). We therefore speculate that ophthalmic surgery might be an independent risk factor for VTE. We wish to alert physicians to keep in mind PE as a severe complication after ophthalmic surgery even in subjects without any predisposing factor for VTE (4). Since ophthalmic surgery is in the microsurgery class, prophylaxis for VTE is usually not recommended due to the risk of bleeding (5). In conclusion, we strongly recommend early mobilization after surgery in subjects who underwent ophthalmic surgery to prevent development of VTE. Notwithstanding we recommend in the selected patients such as susceptibility to thrombosis should be evaluate for medical prophylaxis before ophthalmic surgery.
CONFLICT of INTEREST
None declared.
REFERENCES
- Kanbay A, Kokturk N, Kaya MG, et al. Electrocardiography and wells scoring in predicting the anatomic severity of pulmonary embolism. Respir Med 2007; 101: 1171-6. [?zet]
- Kearon C, Kahn SR, Agnelli G, et al. American College of Chest Physicians. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133(Suppl 6): 454-545.
- Stashenko GJ, Tapson VF. Prevention of venous thromboembolism in medical patients and outpatients. Nat Rev Cardiol 2009; 6: 356-63. [?zet] [Tam Metin] [PDF]
- Chu TG, Pince KJ. Deep venous thrombosis following immobilization after retinal detachment surgery. Ophthalmic Surg 1993; 24: 598-99. [?zet]
- Neuhaus RW, Meyer KT. Chest pain in the postoperative ophthalmic patient. Ophthalmology 1981; 88: 445-6. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Asiye KANBAY,
Alpaslan Mahallesi ?mit Sokak
Alpaslan Apartman? No: 25/14 Melikgazi
KAYSER? - TURKEY
e-mail: kanbaydr@yahoo.com