Multipl mediastinal hidatik kist: Olgu sunumu
Afshin MOHAMMADI, Maryam KHODABAKHSH
1 Urmiye ?niversitesi T?p Fak?ltesi, Radyoloji Anabilim Dal?, Urmiye, Bat? Azerbaycan, ?ran.
?ZET
Multipl mediastinal hidatik kist: Olgu sunumu
Hidatik kist hastal???, ?zellikle Ortado?u ve Orta Asya olmak ?zere bir?ok ?lkede endemik olmaya devam etmektedir. Mediastinal hidatidoz ?ok nadir olup (t?m hidatik kist hastal?kl? olgular?n %0.1'inden az) literat?rde sadece anekdotal olarak bildirilmi?tir. Bilgilerimize g?re, ?imdiye kadar multipl mediastinal hidatik hastal?kl? sadece bir olgu bildirilmi?tir. Biz multipl mediastinal hidatik hastal?kl? ikinci olguyu sunuyoruz ve endemik ?lkelerde multipl mediastinal kitlelerin ay?r?c? tan?s?nda d???n?lmesini ?neriyoruz.
Anahtar Kelimeler: Mediasten, kist, hidatik hastal?k.
SUMMARY
Multiple mediastinal hydatic cyst: a case report
Afshin MOHAMMADI, Maryam KHODABAKHSH
1 Department of Radiology Faculty of Medicine, Urmia University, Urmia, West Azerbaijan, Iran.
Hydatid disease is a parasitic infection that is remains endemic in many countries, particularly the Middle East and Central Asia. Mediastinal hydatidosis is very rare (less than 0.1% of all hydatid disease cases) that have been only anecdotally in the literature. To the best of our knowledge only one case of multiple mediastineal hydatid cysts has been reported previously. We report the second cases of multiple mediastineal hydatid cysts and recommend that it can be considered in the differential diagnosis of multiple cystic mediastineal masses in endemic countries.
Key Words: Mediastinum, cyst, hydatid disease.
Hydatid disease, or echinococcosis, is a parasitic infection by the larvae of Echinococcus granulosus that has been known since the time of Hippocrates (1). It remains endemic in many countries, particularly the Middle East and Central Asia (2).
Mediastinal hydatidosis is very rare (less than 0.1% of all hydatid disease cases) that have been only anecdotally in the literature (3). To the best of our knowledge only one case of multiple mediastineal hydatid cyst has been reported previously by Rahimi-Rad et al. (3).
CASE REPORT
A 20-year-old man reffered to our center with chief complaints of dyspnea, dysphagia and chest pain since six months. There was no history of any previous disease, but he frequently came into contact with sheep. There was no history of fever, trauma and sputum. Physical examination was normal.
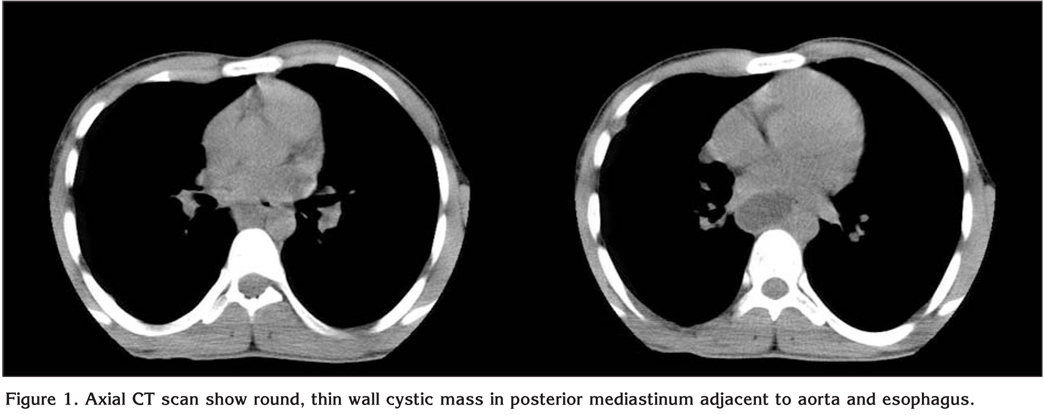
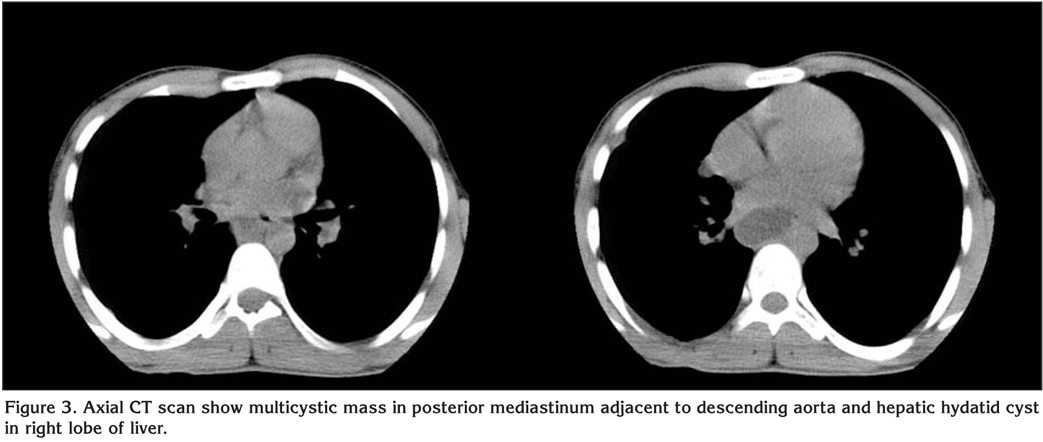
Laboratory datas were normal. There was no eosinophilia. Serology for hydatid disease was negative. Antroposterior chest X-ray showed mild cardiomegally and posterior mediastineal (retrocardiac) mass without calcification. Computed tomography (CT) without contrast revealed posterior mediastineal cystic masses without calcification adjacent to aorta and with compression on esophagus Figure 1, 2.
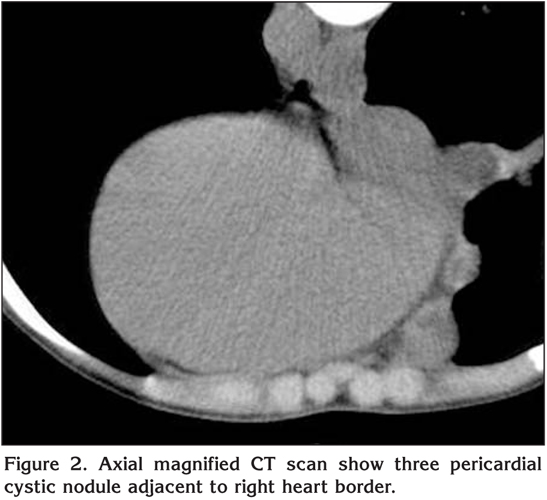
Multiple small cystic nodule adjacent to right sided heart border on pericardium were seen Figure 3.
Right posterolateral thoracotomy was performed. Multiple cystic masses were identified in the posterior mediastinum.
Cysts have adhesions to esophagus and aorta. After packing of the field with saline soaked long gauze aspiration of one of cysts showed clear fluid and diagnosis of hydatid cyst was done.
Total excision of mediastineal cysts and liver cyst were performed.
DISCUSSION
We presented a patient with multiple cystic masses in mediastinum. The differential diagnosis of cystic mediastineal masses in adults and children are neuroenteric, bronchogenic, pleuropericardial, thymic lymphangioma, as well as other rare entity (3).
Mediastinal hydatid cysts are extraordinarily rare condition (1). When cysts appear intrathoracically but in extrapulmonary locations, fatal complications, such as bronchial rupture, fistulas to the pleural and pericardial cavities, and severe bleeding may occur (4).
Two types of mediastinal involvement have been described: primary involvement and secondary to costal, pulmonary and vertebral hydatid disease.
Although hydatid cysts may be asymptomatic, but usually produce various symptoms due to compressive effect on surrounding vital structures such as dyspnea, retrosternal chest pain, cough, dysphasia, back pain, and superior vena cava syndrome (3,5). The most serious complications are invading to aorta and anaphylactic shock due to allergic reaction to cyst materials. Our patients chiefly experienced chest pain, dyspnea and dysphagia consequent to esophageal compression.
Most of posterior mediastinal hydatid cysts are multivesicular and formation of daughter cysts is common vice versa of lung hydatid cyst (6).
Calcification has not been reported in mediastinal hydatid cyst and in the presence of calcification other mediastineal masses should be considered. It possible to establish satisfactory and reliable suspicion with the use of conventional radiography in concert with computed tomographic scanning in pulmonary hydatid cysts but conversely in the case of intrathoracic extrapulmonary cysts, preoperative diagnostic methods are not always reliable.
Many serologic testes are being proposed today. However, due to their low diagnostic value, variable sensitivity and specificity, these testes are not routinely performed in most studies (7).
Diagnosis can be reached with combined assessment of clin ical, radiological, and historical and laboratory data.
Cystectomy and resection of the adjacent pericystic structures is the gold standard method for treatment hydatid cyst (3). When total excision of cyst is impossible because of the location of cyst and invasion to the vital structures, partial pericystectomy is the treatment of choice after the removal of germinative membrane.
To avoid recurrence, it is necessary to place patients on an anthelmintic medical regimen postoperatively.
In conclusion multiple hydatid cysts of the mediastinum are clinical entity that must be considered when caring for a patient with a multiple mediastinal mass in endemic regions. Because of surrounding vital structures the cyst should be treated without delay.
CONFLICT of INTEREST
None declared.
REFERENCES
- Ozyurtkan MO, Kocyigit S, Cakmak M, et al. Case report: mediastinal hydatid cysts. Turkiye Parazitol Derg 2009; 33: 177-8. [?zet] [Tam Metin] [PDF]
- Ulku R, Eren N, Cakir O, et al. Extrapulmonary intrathoracic hydatid cysts. Can J Surg 2004; 47: 95-8. [?zet]
- Rahimi-Rad MH, Mahmodlou R. Multiple mediastinal hydatid cysts: a case report. Pneumologia 2009; 58: 230-2. [?zet]
- Oguzkaya F, Akcali Y, Kahraman C, et al. Unusually located hydatid cysts: intrathoracic but extrapulmonary. Ann Thorac Surg 1997; 64: 334-7. [?zet] [Tam Metin]
- Nazaroglu H, Balci A, Bukte Y, Simsek M. Giant intrathoracic extrapulmonary hydatid cyst manifested as unilateral pectus carinatum. South Med J 2002; 95: 1207-8. [?zet]
- Goenka AH, Das CJ, Goel P, et al. Giant primary posterior mediastinal hydatid cyst in a child: report of a case and review of literature. Pediatr Surg Int 2009; 25: 647-9. [?zet]
- Aletras H, Symbas PN. Hydatid disease of the lung. In: Shields TW, LoCicero J, Ponn RB (eds). General thoracic surgery. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2000:1113-22.
Yaz??ma Adresi (Address for Correspondence):
Dr. Afshin MOHAMMADI,
Urmia, Modaress BLVD, Imam Hospital
URMIA - IRAN
e-mail: mohamadi_afshin@yahoo.com