T?p
fak?ltesi ??rencilerinin sigara i?me oranlar?, yedi y?l s?resince
ger?ekle?tirilen
programs?z t?t?n kontrol? ?abalar? ile azald? m??
Celal KARLIKAYA1, Levent ?ZDEM?R2
1 Trakya ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Edirne,
2 SB D?rtyol Devlet Hastanesi, Hatay.
?ZET
T?p fak?ltesi ??rencilerinin sigara i?me oranlar?, yedi y?l s?resince ger?ekle?tirilen programs?z t?t?n kontrol? ?abalar? ile azald? m??
T?p fak?ltesi ??rencileri t?t?n?n ?l?mc?l etkileriyle m?cadele etmede ?nemli rollere sahip olacaklard?r. Bu ?al??mada, bir?ok t?t?n kontrol? giri?iminin sonucu olarak yedi y?ll?k bir s?rede t?p fak?ltesi ??rencileri aras?nda sigara prevalans?nda de?i?iklik olup olmad???n? de?erlendirmek ama?lanm??t?r. Toplam 854 t?p fak?ltesi ??rencisinden 764 (%89.4)'?ne t?t?n kullan?m? ile ilgili bilgi, tutum ve davran??lar?n? ortaya ??karmaya y?nelik kendi kendine yap?lan bir anket uyguland?. Sonu?lar ayn? y?ntemlerin kullan?ld??? ve yedi y?l ?nce yap?lan tarihi kontrolle kar??la?t?r?ld?. ??rencilerin %25.9'u sigara i?icisi idi (erkeklerin %36.6's?, k?zlar?n %16.3'?), %4.9'u b?rakm??t? ve %69.2'si hi? i?memi?ti. B?rakma h?zlar? erkeklerde k?zlardan daha y?ksekti (%6.8'e kar?? %3.3, p< 0.05). 1999 y?l?ndaki tarihi kontrole g?re sigara i?me h?z? erkeklerde sadece %3.8, k?zlarda %5.5 azalm??t? ve b?rakma h?zlar? daha y?ksek de?ildi. Fak?ltenin ilk y?llar?nda olmak, sigara i?menin ve ?evresel sigara duman?n?n zararlar?na dair d???k bilgi d?zeyi, bekar evinde ya?amak, ka?ak sigaralara kolay ula?mak ve sigara d???nda t?t?n ?r?n? kullanmak sigara i?imi i?in ba?l?ca etkenlerdi. Bu yedi y?ll?k s?rede bir?ok yerel ve ulusal t?t?n m?cadele y?nteminin y?r?rl??e girmesine kar??n t?p fak?ltesi ??rencilerinin sigara i?me h?zlar?nda ?ok az bir azalma saptand?. Sonu? olarak, T?rkiye'deki t?p fak?ltelerinde, ?zel dikkate, organize ve programl? ?abalara gereksinim vard?r.
Anahtar Kelimeler: Sigara, t?p fak?ltesi ??rencileri, t?t?n kontrol?.
SUMMARY
Did unprogrammed tobacco control efforts over seven years decrease smoking prevalence in the medical school?
Celal KARLIKAYA1, Levent ?ZDEM?R2
1 Department of Chest Diseases, Faculty of Medicine, Trakya University, Edirne, Turkey,
2 Dortyol State Hospital, Hatay, Turkey.
Medical students will have significant roles in combating against death tool of tobacco. The aim of this study is to evaluate whether any decrease in the smoking prevalence of the medical students over seven years of many tobacco control efforts. A self-administered questionnaire was carried out among 764 of 854 (89.4%) medical students in order to determine the knowledge, attitudes and behaviors towards tobacco use. Chi-square tests, Student's t-test and multiple logistic regression methods were used. Results were compared with the historical control study that was done seven years ago with same methods. 25.9% of the students were smoker (36.6% of males, 16.3% of females), 4.9% was exsmoker and 69.2% was non-smoker. Quit rate was high among males than females (6.8% versus 3.3%, p< 0.05). When compared with historical cohort in 1999, smoking rate decreased only 3.8% for males and 5.5% for females, and quit rates were not higher. Lower curriculum year, and lower knowledge level about the harms of smoking and environmental tobacco smoke in lower grades, living in bachelor homes, easy access to smuggled cigarettes, using non-cigarette tobacco products were main factors for smoking. There was little decline in smoking rates of medical students despite of many local and national tobacco control efforts over seven years. Special attention and organized, programmed efforts are needed in medical schools in Turkey.
Key Words:? Smoking, medical students, tobacco control.
Tobacco products, primarily cigarettes, cause serious illnesses and deaths all around the world. Tobacco control efforts must be increased promptly especially in developing countries where smoking rates are increasing. Since many smokers have to visit the doctor, doctors and medical students as future doctors have a significant role in combating against this death tool. It has been noted that smoking is widely common among doctors and a meaningful difference from the general population was not stated for the doctors who are considered to contribute in fighting against the tobacco to a large extent with their attitudes and behaviors (1). To train doctors of the future against smoking is one of the primary objectives of Turkey's National Tobacco Control Program. More effective education for Tobacco Control is an inescapable and urgent necessity in Medical Faculties of Turkey (2). Already, the World Health Organisation (WHO) has suggested that training of medical students has to be restructured to include competencies to help health workers manage today's most prevalent health problems like tobacco control (3).
The purpose of our study is to research the smoking prevalence of medical students and the knowledge, behaviors and attitudes towards the tobacco use and to compare with historical control to evaluate whether any decrease in the smoking prevalence despite of many local and national tobacco control efforts over seven years, and to determine educational needs and get clues to develop effective programs.
MATERIALS and METHODS
764 students out of 854 students, who were attending Medical Faculty in 2006-2007, formed the study group. To reach all the students was aimed, so sampling procedure was not performed. A self-administered survey questionnaire, which was prepared based on WHO questionnaires, was first administered to 20 nursing students, and the framework of the survey was formed after it was validated in aspects of reliability and consistency. The survey questionnaire consisted of questions about demographics, smoking status, accommodation conditions, and knowledge level about harms of smoking and environmental tobacco smoke. In addition, the questionnaire consisted of questions on attitude and behaviors about smoking and tobacco control efforts. The definitions for smoking status were as in WHO's criteria [never smoker, current smoker (occasional and daily smoker) and exsmoker] (4).? These definitions and questions to asses that were identical with our study done in 1999.
Pearson and Fisher's exact chi-square methods for univariate analysis were used as descriptive statistics. Student t-test was used to compare the difference between means. Multiple logistic regression method was used in multi-variate analysis of nominal values. Statistica 7.0 was used for statistical analysis.
RESULTS
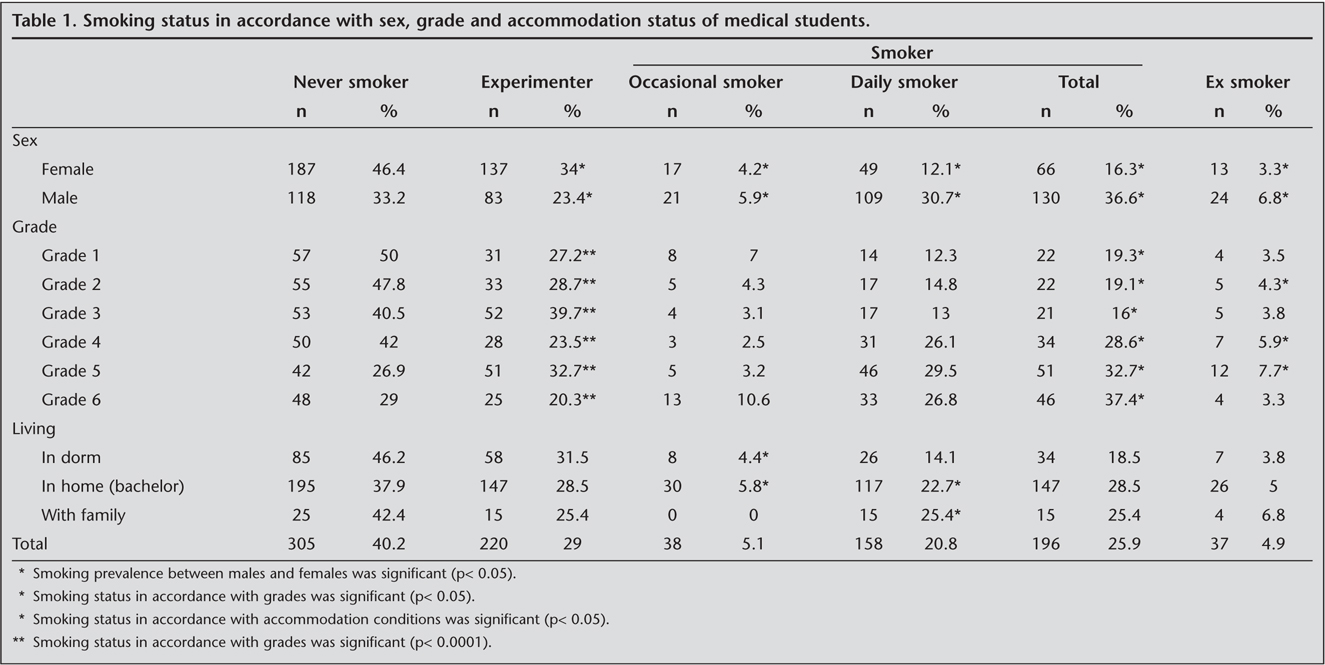
764 out of 864 students (89.4%) were reached and completed the questionnaire. Answers of eight students were out of consistency, so they were excluded and 758 questionnaires (88.7%) were taken into evaluation. Out of 758, 355 (46.8%) were males and 403 (53.2%) were females. Average age of trying smoking for the first time was 14.3 ? 4.2 years for males and 15.3 ? 3.8 years for females (p< 0.05). It was found that 25.9% of the students was current smoker (36.6% of males, 16.3% of females), 4.9% was exsmoker, and 69.2% was non-smoker (29% experimenter, 40.2% never smoker). It was found that smoking rate was increasing from the first grade to the sixth grade and smoking rate was low in the first three years (19.3%, 19.1%, 16%). Students staying in dormitories had lower smoking prevalence (18.5%) than the ones staying in bachelor homes (28.5%) or living with their families (25.4%). Smoking status in regard to sex, grade and accommodation conditions is shown in Table 1.
Average age for regular or frequent smoking was 18.2 ? 2.7 years for males and 18.8 ? 3.2 years for females. Males were smoking much more than females (11.9 ? 8.9 cigarettes/day for males and 7.1 ? 7.2 cigarettes/day for females, p< 0.05). When smoking periods were compared, it was found that males smoked for 4.2 ? 3.2 years and females smoked for 3.1 ? 2.4 years, p< 0.05).
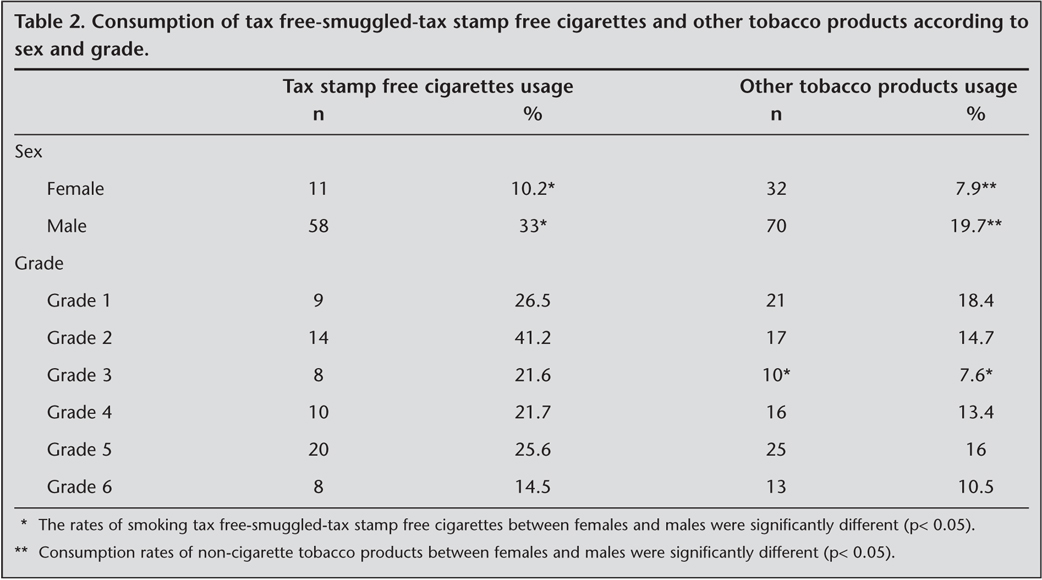
Consumption of duty free/smuggled/tax stamp free cigarettes was significantly more common among males than females (33% vs. 10.2%, p< 0.05) (Table 2). Consumption of tobacco products other than cigarettes was also more common among males (19.7% vs. 7.9%, p< 0.05), and the rate was lower among third year students. Students who stated using other tobacco products had used water-pipes (37.2%), cigars (9.2%) and pipes (0.5%).
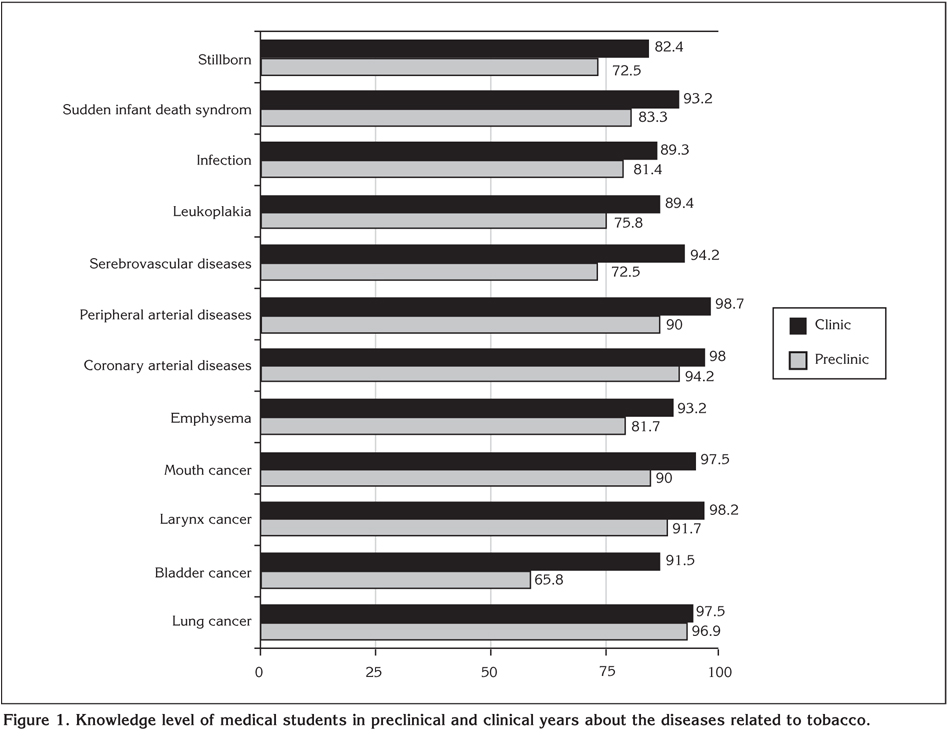
When the knowledge level about the harms of tobacco was evaluated, it was found that knowledge about the harms of active smoking was increasing as the grade was higher (grade 1: 77.4%, grade 2: 81.6%, grade 3: 88.9%, grade 4: 94.4%, grade 5: 94%, grade 6: 94.5%). The knowledge level of students who had been smoking for a long time was lower (p< 0.05). Knowledge level of females in grade 1 was significantly higher than males (p< 0.05). The most known illnesses related to smoking were lung cancers, heart diseases, larynx cancers, peripheral vascular diseases, mouth cancers, infections, sudden infant death syndromes, emphysema, cerebral vascular diseases, leukoplakia, and the least known were bladder cancers and stillbirths. Knowledge level about the harms of active smoking was found to be lower in preclinical classes (grade 1, 2, 3) than clinical classes (grade 4, 5, 6) (p< 0.05). Bladder cancer (65.8%) and stillbirth (72.5%) were significantly less known in preclinical grades (Figure 1).
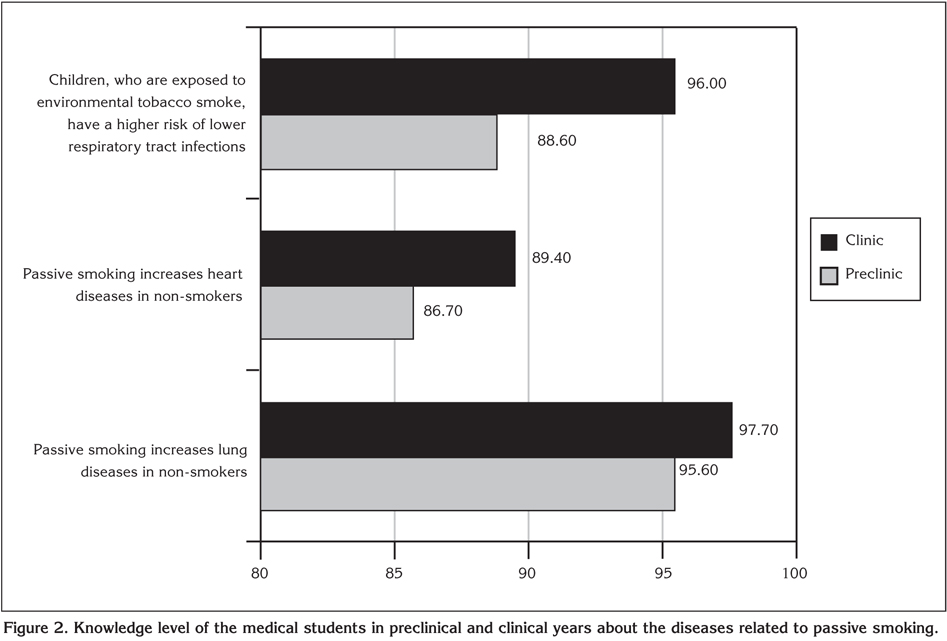
It was found that the knowledge level about harms of passive smoking was higher in higher grades (grade 1: 82.3%, grade 2: 93.6%, grade 3: 93.6%, grade 4: 94.9%, grade 5: 94%, grade 6: 94.2%, p< 0.05). Females knew significantly more than males about the harms of passive smoking (p< 0.05). Knowledge level about passive smoking and lung diseases was higher in preclinical grades (95.6%) than knowledge of heart diseases (86.7%) and lower respiratory tract infections in children (88.6%) (Figure 2).
Attitudes of students towards protecting people from passive smoking, and their thoughts about medical staff as role models for smoke-free life, behaviors of tobacco industry, minors' access to tobacco products and their knowledge level about addiction are shown in Table 3. There was general consensus on need for legislations on passive smoking in public places. However, there was some confusion about smoking restrictions and total ban. While 94% of students agreed on banning smoking in public places like hospitals and schools, 80.1% disagreed on annihilation of smoking rooms.
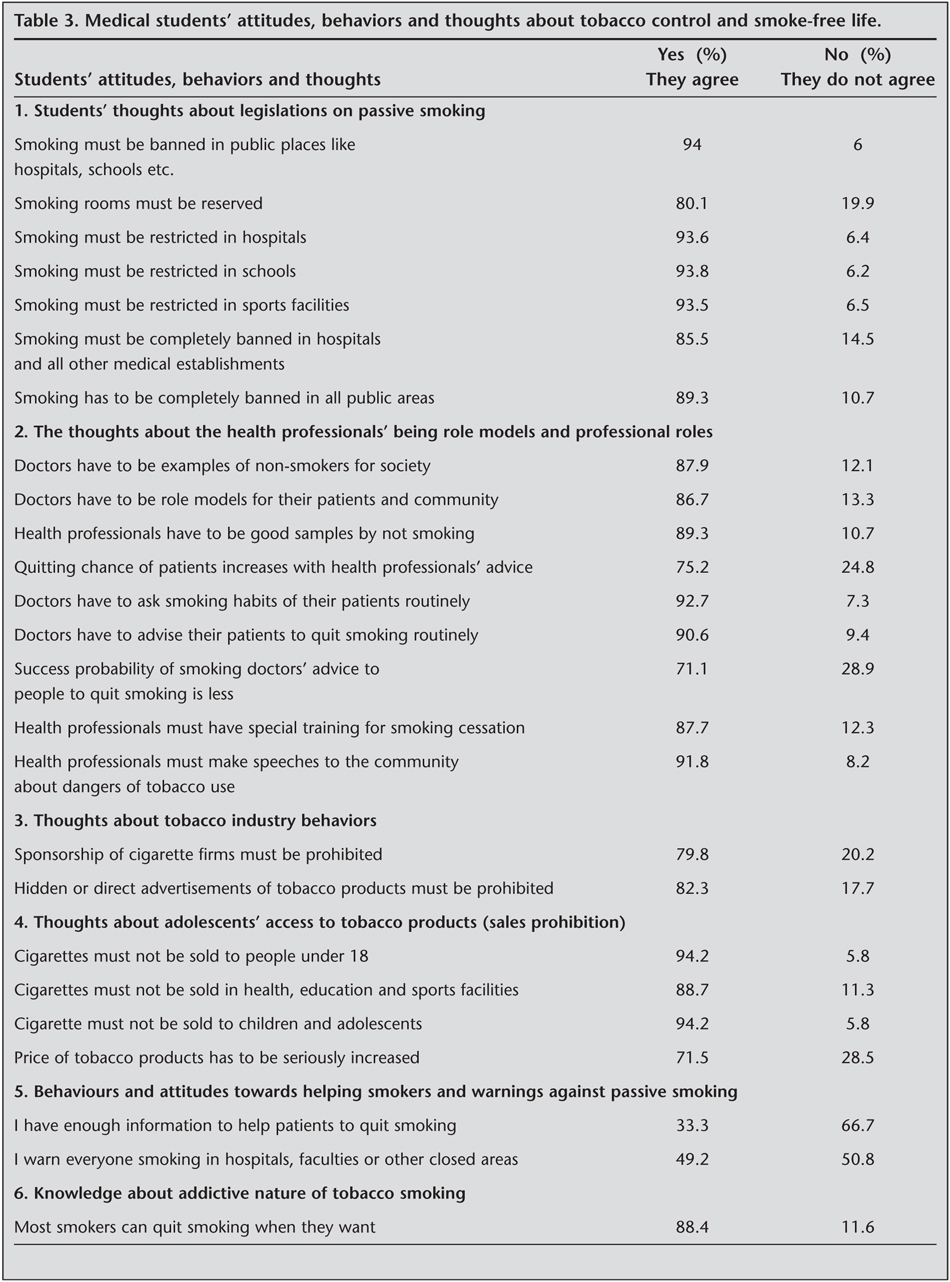
In general, there were agreements (> 85%) about the health professionals' being role models in society. In general, they thought that doctors must help for smoking cessation. However, 24.8% of students thought that professional advice could not help. And 28.9% of students thought smoker doctors can help smokers as much as non-smoker doctors. Their thoughts about behaviors of tobacco industry were that sponsorship must be prohibited (79.8%), and explicit and hidden advertisements of tobacco products must be prohibited (82.3%). And also, they thought that adolescents' access to tobacco products must be restricted. But, their knowledge about the fact that tobacco price policy is an effective tobacco control method was lower (71.5%). Only 33.3% of students were confident about helping people for quitting. More than half (50.8%) of the students did not warn smokers smoking in hospitals, faculties or other closed areas. Most of the students (88.4%) did not have enough knowledge about how addictive smoking is.
DISCUSSION
In this study, we found that smoking prevalence among medical students was 25.9% (36.6% for males and 16.3% for females). In our 1999 historical control study, smoking prevalence was 30.5% (40.4% for males, 21.8% for females) (5). We thought that decrease in smoking prevalence is not significant over these seven years (only 3.8% drop for males and 5.5% for females) (5). Local tobacco control efforts during these seven years from 1999 to 2006 were local awareness campaigns twice or thrice in a year, institutions of smoking cessation clinic in the hospital (in 2001), organizing uncoordinated lectures about harms of tobacco smoking from grade 1 to 5 (from 2001), public declarations and setting the hospitals as smoke-free in 2005. During these seven years, at national level, health warnings appeared in 2006 and national public awareness campaigns on mass media were seen twice or thrice in a year from 2000s.
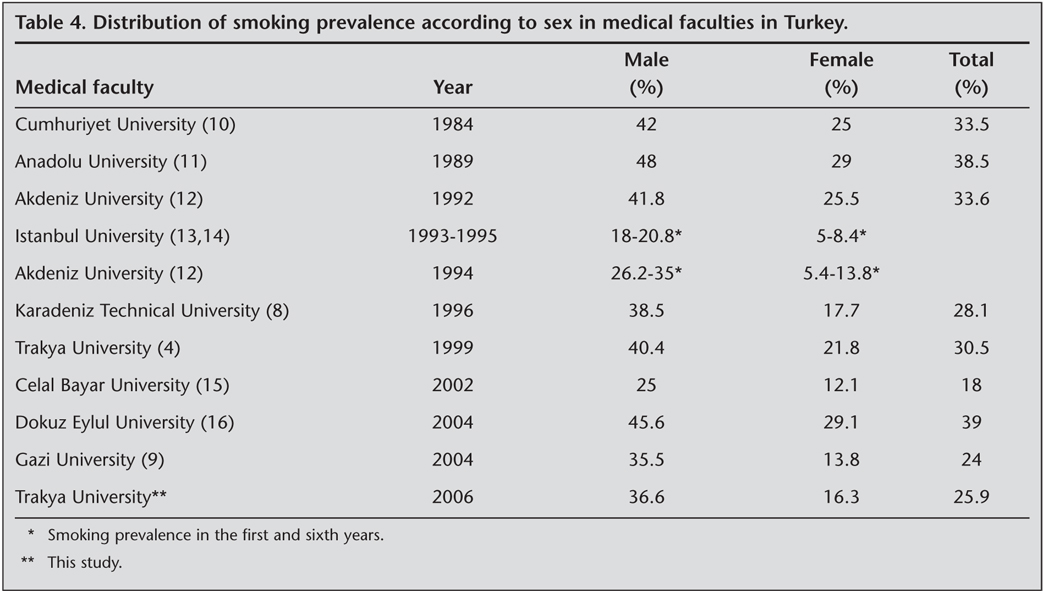
In the studies worldwide, which included more than 9000 medical students in 51 faculties in 42 countries, smoking prevalence was 0-56.9% for males and 0-44.7% for females (6,7). The surveys done among the students of faculty of medicine in Turkey are shown on Table 4 (5,8-16). When compared, our findings are similar with the results of the studies done by Can et al. and Ilhan et al (8,9).
One of the proposed reasons for medical students' starting to smoke or smoking more during their university years is insufficient education (6,17). Like some other studies done in Turkey, attention was drawn to the fact that smoking habit of the medical students grew as their grades did (5,9,11,16). In the present study, it was found that smoking rises from grade 1 to grade 6 except that it is in the lowest rate in grade 3 (16%). As in other studies, smoking was distinctly low in the first three years in this study as well (9,15). Hence, we concluded again that education against tobacco must start from grade 1st. In present study, it was found that quit rate among grade 4th students was higher. We evaluated that it was due to special lectures against tobacco and effective encouraging for smoking cessation.
When the relationship between accommodation and smoking status was evaluated, we found that smoking rate for students living with their families and staying in bachelor homes were much more than those staying in dormitories. These results were consistent with the study done by Ilhan et al. and our historical control study (5,9). The reason for that may be that the students staying with their families or in bachelor homes could behave more freely in social and economic aspects.
As a difference from the other studies done in Turkey, we investigated the effects of tax free, smuggled or tax stamp free cigarettes on smoking behaviors. Because Edirne is a cross country border city, access to tax free, smuggled or tax stamp free tobacco products is easier than some other cities (18). In this study, 33% of males and 10.2% of female students declared consuming such products. These results were lower than 1999 study (50% for males, 23.1% for females) (5). We speculated that this might be due to some socio-economical improvements, some additional official measures for preventing smuggling and some awareness against such products. We speculated that reasons for higher consumption rate of such products among males are mostly economic and it is easier for them to get access to such sellers.
Water-pipe smoking has increased significantly among the adolescents in Turkey, recently (19). Using tobacco product other than cigarette was asked as well in the present study and the rate was stated as 19.7% for males and 7.9% for females using other tobacco products. It was stated that 37.2% of students using water-pipe, 9.2% cigar and 0.5% pipe. We concluded that harms of all tobacco products must be learned during curriculum.
When the students' knowledge level was investigated according to curriculum taught, It?l et al. found a significant difference between preclinical and clinical years (16). They found that students knew more on the relationship between tobacco and lung cancers and coronary artery diseases. However, their knowledge about the relationship with peripheral vascular diseases, bladder cancer and esophagus cancer was insufficient. Yildirim et al. found that students knew that lung cancers, coronary artery diseases, throat cancers and mouth cancers were caused by smoking, but the effects of cigarettes on bladder cancers, infant deaths and cerebrovascular diseases were known less (15). In our study, the most known diseases caused by cigarettes were respectively lung cancers, heart-artery diseases, throat cancers, peripheral artery diseases, mouth cancers, infections, sudden infant death syndromes, emphysema, strokes and leukoplakia, and the least known were bladder cancers and stillbirth. It was stated that in the first three years (preclinical term), knowledge level was low in comparison with the clinic term and knowledge level increased as the grades did. As a difference from the other studies, in our study, knowledge level of medical students about passive smoking was evaluated and we concluded that lectures about the harms of passive smoking must be increased.
Since the behaviors of health professionals have the potential to affect the community, they have important missions and responsibilities. Although students accepted that the doctors have to be role models, smoking of some medical lecturers led them to experience a lack of role model or even exposure to a wrong model. When the thoughts of the students about health professionals' role model were asked, it was said that primarily university lecturers and health professionals have to be role models.
Advertisements, promotions and sponsorship of tobacco industry, easy access to tobacco products and low prices affect smoking behaviors of adolescents (20). Legislations for adolescents' access to tobacco products are important for tobacco control. We analyzed thoughts of the students about industry behavior and adolescents' access. Most of the students stated that advertisements, sponsorship, sales to people under 18 years old and sales in health, education and sports facilities must be banned. But, consensus on raising cigarette prices was not so high.
In conclusion, smoking prevalence was not significantly decreased during the last seven years and it is still high in the Medical School. We thought the reason for that as lack of knowledge, social and cultural context and tobacco industry efforts like smuggling. As in many medical schools of Turkey, special and comprehensive tobacco control efforts must be organized and coordinated. Education for tobacco control and smoking cessation treatment must be revised and programmed in medical schools of Turkey.
CONFLICT of INTEREST
None declared.
REFERENCES
- Beyer J, Waverly I. Tobacco Control Policy, Strategies, Successes and Setbacks, Washington: The World Bank, 2003: 1-12.
- Republic of Turkey Ministry of Health, National Tobacco Control Programme and Action Plan of Turkey 2000-2012. Ankara: T?OF Plaka Matbaac?l?k, 2008.
- Pruit SD, Epping-Jordan JAE. Preparing the 21st century global healthcare workforce. BMJ 2005; 330: 637-9. [Tam Metin] [PDF]
- World Health Organization. Guidelines for the Conduct of Tobacco-Smoking Surveys of the General Population. WHO/SMO/Geneva, 1983; 4: 83.
- Karl?kaya C, Erdo?an S, ?ak?r E, Hatipo?lu ON. Smoking habits and related factors of students in Trakya University, Faculty of Medicine. Journal of Trakya University Faculty of Medicine 2000; 17: 161-9.
- Richmond R. Educating medical students about tobacco. Thorax 1999: 54: 70-8. [PDF]
- Crofton JW, Freour PP, Tessier JF. Medical education on tobacco: implications of a worldwide survey. Tobacco and Health Committee of the International Union against Tuberculosis and Lung Disease (IUATLD). Med Educ 1994; 28: 187-96. [?zet]
- ?an G, ?zl? T, B?lb?l Y, Torun P. Smoking habits of students in Karadeniz Technical University, Faculty of Medicine. Tuberk Toraks 1998; 46: 245-9.
- ?lhan F, Aksakal NF, ?lhan MN, Ayg?n R. Smoking State of Students in Gazi University Medical Faculty. TAF (Turkish Armed Forces) Protective Medicine Bulletin 2005; 4: 188-98.
- Yard?mc? E, K?yan A, ?zbilen T.? Meta-analysis related to prevalence of smoking of medical students in Turkey. (Summary) V. Public Health Congress Book.? ?stanbul, 1996: 175-7.
- U?kun ?, Metinta? S, ?zdemir N, et al. Smoking habit of beginner university pupils and their families: first results of four years' cohort study. Tuberk Toraks 1999; 47: 305-10.
- ?zdemir T, Saka O, Artvinli M. Smoking habits of medical students in Akdeniz University and their thoughts about cigarette effect on health. Journal of Akdeniz University Faculty of Medicine 1992; 9: 7-10.
- Erkan F, Sabuncu H, Ertu?rul E. Smoking behaviours of lecturers and students in Istanbul University, Faculty of Medicine. (Summary) Istanbul Faculty of Medicine 12th General Assembly Summary Book, 1993.
- Sahip Y, ?zbilen T, Erkan F. Knowledge, attitude and behaviours of Istanbul Medical Faculty students related to smoking. (Summary) Istanbul Faculty of Medicine General Assembly Summary Book, 1995.
- Y?ld?r?m ?, ?elik P, ?akar A, Din? G. Attitude of medical students against cigarette. Respiration 2004; 6: 30-5.
- Itil O, Erg?r G, Ceylan E. Knowledge and Attitudes about smoking student in a medical faculty. Turkish Respiratory Journal 2004; 5: 86-91.
- Allen MB. Medical students' knowledge of smoking. Thorax 1999; 54: 2. [PDF]
- Karl?kaya C. Smoking prevalence of high school students in Edirne. Smuggling, advertisements and accessing cigarette of adolescents. Tuberk Toraks? 2002; 3: 6-12.
- Suba?? N, Bilir N, ?lhan E, Avluk A. Knowledge, Attitude and Behaviours of Hookah Smokers about Smoking Hookah. Tuberk Toraks 2005; 6: 137-43.
- Benowitz N. Nicotine addiction. Prim Care Clin Office Prac 1999; 26: 6111-31.
Yaz??ma Adresi (Address for Correspondence):
Dr. Celal KARLIKAYA,
Trakya ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,?
22030 ED?RNE - TURKEY
e-mail: celalk@trakya.edu.tr